
Abstract
Objective:
To investigate the morbidity and comorbidity of nonalcoholic fatty liver disease (NAFLD) and different glucose intolerance strata in a community-based population and to explore the association between glucose tolerance levels and NAFLD.
Methods:
A community-based cohort established for Pinggu Metabolic Disease Study in a suburb of Beijing, China, was established from September 2013 to July 2014 using a random sampling method. Participants were eligible if they were born in Pinggu and had been living there for at least 5 years within the age range of 26–76 years. A 75 grams oral glucose tolerance test was used to determine the strata of glucose tolerance. Unenhanced abdominal computed tomography scan was performed to identify NAFLD.
Results:
A total of 3122 subjects were included in this analysis. The prevalence of NAFLD was 22.68% (27.58% vs. 19.97% among men and women). The prevalence of type 2 diabetes (T2D) was 18.03% (20.83% vs. 16.22% among men and women). Up to 7.21% of residents had both T2D and NAFLD. 39.96% of diabetic patients and 28.77% of prediabetic patients combined with NAFLD. Compared with adults with normal glucose tolerance, the incidence of NAFLD in T2D patients was more than three times higher after adjusting for sex, age, body mass index (BMI), sedentary time, and dietary habit [odds ratio (OR) = 3.58, confidence interval (95% CI) 2.80–4.58, P < 0.001]. NAFLD was also more common in individuals with prediabetes, especially patients with impaired glucose tolerance (IGT) (OR = 2.27, 1.75–2.95) or impaired fasting glucose+IGT (OR = 2.78, 1.92–4.03).
Conclusions:
The morbidity and comorbidity of NAFLD and glucose intolerance are high in the Pinggu population in northern China, highlighting the importance of early prevention and treatment of these two diseases at the same time.
Introduction
Type 2
Previous studies have shown a high prevalence and comorbidity rate of NAFLD and T2D, and the correlation between fatty liver and glucose metabolism has also been assessed. 5,8,9 However, a majority of studies have focused on the impact of NAFLD on the incidence of T2D, but few studies have explored the effects of T2D on the development of fatty liver. 10,11 Using the fatty liver index as a proxy of diagnosis of NAFLD, the AMD-Annals Study Group reported that more than half of T2D patients presenting with NAFLD in Italy. 10 Silaghi et al. found that outpatients with T2D had a high prevalence of NAFLD even with normal levels of liver function. 11 Because diabetes and fatty liver are both a progressive disease spectrum, gradually worsening glucose intolerance may exacerbate NAFLD by promoting progression to hepatic fat accumulation and steatohepatitis and even fibrosis. 6,7,12 Mechanically, the imbalance between islet cell secretion and insulin resistance contributes differently to the phenotype of hyperglycemia. 13 However, the impact of prediabetes on NAFLD has been less well defined, especially at different levels of glucose intolerance. Recently, Rajput and Ahlawat reported that the prevalence of NAFLD was significantly higher in prediabetics (59%) compared with controls (26%) in a cross-sectional study. 14 Regrettably, most of the participants in these studies were hospitalized patients or subjects on whom a physical examination or a clinical study was performed. To date, no study has investigated the prevalence of NAFLD defined by different glucose tolerance strata in the level of community population.
The Pinggu (PG) cohort is a community-based population that was established in the district of Beijing in northern China to study how genetic and environmental factors might contribute to the growing chronic metabolic disease epidemic. We have determined the strata of glucose metabolism in all nondiabetic patients according to a 75 grams oral glucose tolerance test (OGTT) and identified fatty liver using noninvasive abdominal computed tomography (CT) scan in the PG cohort. Here we tried to estimate the comorbidity of NAFLD under different glucose tolerance strata and to analyze the potential association between NAFLD and glucose intolerance levels in this population.
Patients and Methods
Study population
The analyzed data come from a community-based cohort that was established for the Pinggu Metabolic Disease Study (PGMDS) focused on the natural course and pathogenesis of chronic metabolic diseases. This survey was performed in the Pinggu District of Beijing, China, from September 2013 to July 2014. Participants were eligible if they were born in Pinggu and had been living there for 5 or more years between the ages of 26 and 76 years. Based on the national Civil Registration system, a total of 6583 participants were identified using the multiple-stage random sampling process according to sex and age compositions. Five towns were randomly selected from 16 towns in rural areas, 5 villages were randomly selected from each town, and half of the participants were randomly selected from the 25 villages. The remaining participants were randomly selected from randomly selected urban areas (one of the two). The population sample studied here reflected a typical Chinese community. The protocol of PGMDS has been described in detail previously. 15,16 Finally, 4002 individuals attended the program, which gave a response rate of 60.8%.
Participants with the following conditions were excluded: 656 participants had a history of heavy alcohol consumption in the past year (men >210 g/week or women >140 g/week), 140 participants had hepatitis B or C infection, 18 did not perform CT scans, and 5 were missing data on glucose. We further excluded 61 participants with overt hyperthyroidism or hypothyroidism, severe hepatic or renal dysfunction, or advanced cancer. Finally, a total of 3122 individuals (1229 men and 1893 women) with complete data remained for the current study (Fig. 1). The study is approved by the Ethics Committee of Peking University Health Science Center. All participants provided written informed consent.
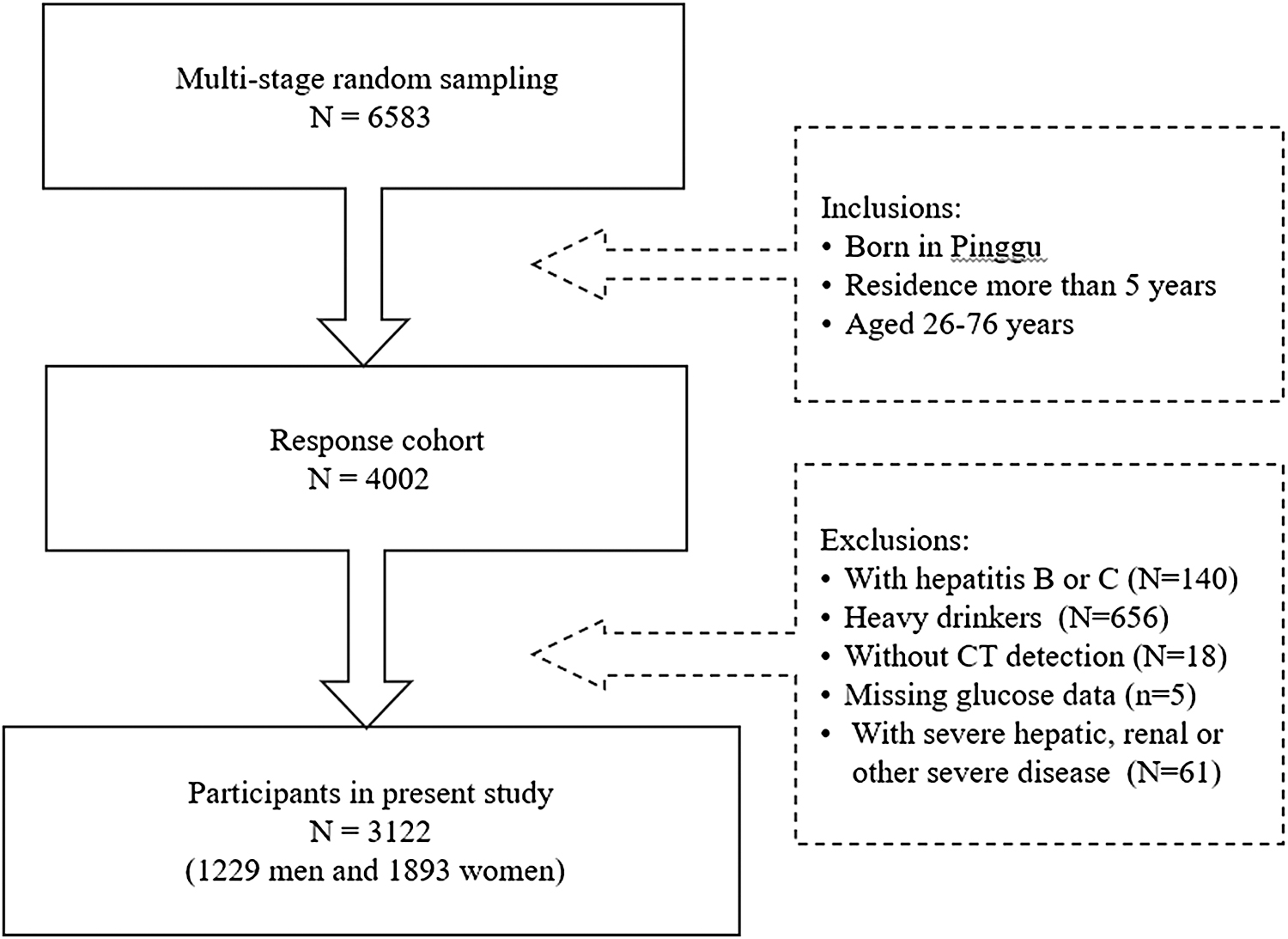
The flowchart for the selection of the study participants.
Investigation
A detailed questionnaire on sociodemographics, family history of chronic disease, medical history, lifestyle, and other health-related topics was completed during a face-to-face interview in the study center. In the present study, we chose daily sedentary time as the representative indicator of lifestyle and classified it as follows: <1.5, 1.5–2.5, 2.5–3.5, 3.5–4.5, or ≥4.5 hr/day (Supplementary Table S1
Comprehensive anthropometric measurements, including height, weight, waist circumference (WC), hip circumference (HC), and blood pressure, were performed by trained doctors and nurses according to standardized protocols. BMI was calculated as weight in kg divided by height in m2. The waist-to-hip ratio was calculated as WC divided by HC. Blood pressure was measured three times after 5 min of resting in a seated position and the mean of the measures was used. All participants underwent standard 12-lead ECGs in a supine position.
Laboratory measurements
All participants had blood samples taken in the morning after an ∼10-hr fast to evaluate glucose, lipids, and biochemical profiles. A standard 75 grams 2-hr OGTT was conducted for individuals without known diabetes. Participants with history of diabetes had fasting plasma glucose measured only. Cation-exchange high-pressure liquid chromatography method (Adams A1c HA-8160; Arkray, Kyoto, Japan) was used to measure hemoglobin A1c (HbA1c). Serum hepatitis B virus surface antigen (HBsAg) and hepatitis C antibodies (anti-HCV) were tested by chemiluminescence assays (Ortho-Clinical Diagnostics, NJ). Fasting serum biochemical profiles, including liver function, kidney function, and lipids, were measured using a biochemical analyzer.
Abdominal CT
Nonenhanced abdominal CT scans were performed for each participant using a 64-slice multidetector scanner with continuous 5-mm-thick slices (120 kVp, 120–150 mA) from the lung base to the pubic symphysis (LightSpeed VCT; General Electric Healthcare, Milwaukee, WI). The mean Hounsfield units of three 1 cm2 areas in the liver and two 1 cm2 areas in the spleen were used to calculate the L/S ratios.
Disease definition
According to criteria issued by the working group on obesity in China, 19 participants were classified as underweight (BMI <18.5 kg/m2), normal weight (18.5–23.9 kg/m2), overweight (24.0–27.9 kg/m2), or obese (≥28.0 kg/m2).
Hypertension was defined as an average systolic blood pressure ≥140 mmHg or an average diastolic blood pressure ≥90 mmHg, previously diagnosed hypertension, and/or the use of antihypertensive medication. 20
Based on the definition of the “Chinese Guidelines on the Prevention and Treatment of Dyslipidemia in Adults,” 21 dyslipidemia was defined as total cholesterol ≥5.18 mmol/L, triglycerides ≥1.7 mmol/L, high-density lipoprotein cholesterol <1.04 mmol/L, low-density lipoprotein cholesterol ≥3.37 mmol/L, and/or the treatment of abnormal blood lipids.
In this study, diabetes mellitus (DM) was defined as fasting plasma glucose (FPG) ≥7.0 mmol/L and/or 75 grams OGTT 2-hr plasma glucose (2-hPG) ≥11.1 mmol/L (WHO criteria in 1999), 22 a self-reported history of diabetes diagnosed by a physician, or the use of antidiabetic agents. Prediabetes was defined as impaired glucose tolerance (IGT, FPG <7.0 mmol/L and 7.8 ≤ 2-hPG <11.1 mmol/L) or impaired fasting glucose (IFG, 6.1 ≤ FPG <7.0 mmol/L and 2-hPG <7.8 mmol/L).
Individuals were diagnosed with NAFLD in the current study according to the following definitions: (1) fatty liver based on abdominal CT scan with an L/S ratio ≤1.1, 23 (2) a negative test of HBsAg and anti-HCV, (3) no history of significant alcohol consumption (men >210 g/week or women >140 g/week), and (4) no other special cause of secondary hepatic disease, such as steatogenic drug administration. 24
Statistical analysis
Continuous variables are expressed as mean and standard deviation (
Results
Characteristics of the study population
The sex and age compositions of the total survey population and the analyzed population are shown in Table 1. A total of 4002 individuals attended the community-based program, of which 3122 eligible individuals (1229 men and 1893 women) were included in this analysis. Participants excluded from the analysis were mainly males who drank heavily (16.39%). As shown in Table 1, the mean age of the study population was 50.11 years, with an SD of 11.92 years. The mean BMI was 26.10 ± 3.85 kg/m2, with a high prevalence of overweight (40.52%) and obesity (28.92%). The BMIs of the T2D group and NAFLD group were 27.62 ± 3.78 and 27.73 ± 4.09 kg/m2, respectively, which were higher than the average BMI of the analyzed population. The mean HbA1c in the T2D group (about 1/3 newly diagnosed diabetic patients) was 7.15%, which was significantly higher than the average HbA1c level (5.85%) of the analyzed population. The liver function (ALT/AST) of most participants, including T2D, NAFLD, and coexisting patients, was within the normal reference range. Menopausal status was reported by 49.17% of the women. Given the different prevalences of diabetes and NAFLD between women and men, we divided subjects by sex in the following analyses.
Characteristics of the Participants
The data are presented as mean ± standard deviation, median, and interquartile range.
2hPG, 2-hr plasma glucose; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; Cr, creatinine; DBP, diastolic blood pressure; FPG, fasting plasma glucose; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; HOMA-IR, homeostasis model assessment for insulin resistance; LDL, low-density lipoprotein; SBP, systolic blood pressure; SD, standard deviation; TG, triglycerides; UA, uric acid; WHR, waist-to-hip ratio.
The prevalence of T2D and NAFLD
In this study population, the prevalence of T2D was 18.03% (20.83% men vs. 16.22% women). The prevalence of different glucose tolerance strata by sex and age is shown in Table 2. The distributions of glucose intolerance strata were not only different between men and women (χ 2 = 48.41, P < 0.001) but also varied by age group, both in men and women (χ 2 = 61.55, P < 0.001 and χ 2 = 286.40, P < 0.001). The prevalence of T2D in participants aged ∼26, ∼45, and ≥60 years was 13.19%, 25.25%, and 25.45% in men, and 3.05%, 18.25%, and 31.46% in women, respectively. Among male residents, the prevalence of diabetes showed a very significant trend of early onset. The prevalence of diabetes in women after menopause increased rapidly and even exceeded that of men. The prevalence of IGT of each age group in women was generally higher than that in men.
The Prevalence of Different Glucose Tolerance Strata and Nonalcoholic Fatty Liver Disease by Sex and Age (χ 2 Test)
The data are presented as %. P value is for the trend across age groups.
IFG, impaired fasting glucose; IGT, impaired glucose tolerance; NAFLD, nonalcoholic fatty liver disease; non-NAFLD, without nonalcoholic fatty liver disease; NGT, normal glucose tolerance; T2D, type 2 diabetes mellitus.
The prevalence of NAFLD was 27.58%, 19.97%, and 22.68% in men, women, and both together, respectively. As shown in Table 2, the distribution of NAFLD was significantly different between men and women (χ 2 = 20.13, P < 0.001) and varied among age groups in women (χ 2 = 14.91, P = 0.001) but not in men (χ 2 = 4.45, P = 0.108). Among adults <45 years, the prevalence of NAFLD in men was twice that of women. The prevalence of NAFLD in women increased rapidly after menopause and was close to men.
The prevalence of NAFLD in different glucose tolerance strata
The prevalence of NAFLD in different glucose tolerance strata is listed in Table 3. The prevalence of NAFLD in individuals with NGT, IFG, IGT, IFG+IGT, and T2D was 19.50%, 19.78%, 35.11%, 40.54%, and 40.63% in men, respectively (χ 2 = 57.30, P < 0.001). The corresponding prevalence of NAFLD was 11.34%, 24.32%, 26.79%, 29.59%, and 39.41% in women, respectively (χ 2 = 139.41, P < 0.001). Among 563 T2D patients, 39.96% also had NAFLD. Nearly 30.0% of individuals in the prediabetic state had fatty liver, especially in participants with IGT or IFG+IGT. It is noted that more than half of the younger T2D patients (25–45 years) also had NAFLD. Among the 3122 participants included in this analysis, 225 had both T2D and NAFLD, with a comorbidity rate as high as 7.21%.
The Prevalence of Nonalcoholic Fatty Liver Disease in Different Glucose Tolerance Strata by Sex (χ 2 Test)
The data are presented as N and %. P value is for the trend of NAFLD across the status of IGT.
DM, diabetes mellitus.
Correlation between glucose intolerance levels and the incidence of NAFLD
In this analysis, a multivariable regression model was adopted to assess the impact of different degrees of glucose intolerance (DM, IFG, IGT, and IFG+IGT) on the incidence of NAFLD before and after adjustment for possible confounding factors sequentially for sex (male, female), age (youth, middle age, old age), BMI (underweight, normal weight, overweight, or obese), sedentary time (<1.5, 1.5–2.5, 2.5–3.5, 3.5–4.5, or ≥4.5 hr/day) and dietary habit (the frequency of red meat intake, never/rarely, monthly, 1–3 days per week, 4–6 days per week, and daily) in models 1–7, as shown in Supplementary Table S2. Compared with adults with NGT, the odds of NAFLD in T2D patients increased more than three times after adjustment for the potential confounders (OR = 3.58, 95% CI 2.80–4.58, P < 0.001). NAFLD was also more common in individuals with prediabetes, especially in patients with IGT (OR = 2.27, 95% CI 1.75–2.95, P < 0.001) or IFG+IGT (OR = 2.78, 95% CI 1.92–4.03, P < 0.001).
Discussion
The prevalence of diabetes is increasing worldwide, with distinct evidence of a high prevalence among Asians, especially in China. 25 Consistent with the global trends, the mean prevalence of NAFLD in China has dramatically increased from 18% to 29% within a decade, at more than twice the rate in Western countries. 26 –28 Higher prevalence rates of NAFLD were also reported in other Asian countries, such as Japan, Korea, and India, currently estimated to be 29.6%. 29,30 In this representative population in northern China, the prevalence of T2D and NAFLD was 20.83% and 26.85% in men and 16.22% and 19.97% in women, respectively; up to 7.21% of patients had both T2D and NAFLD, which confirmed the high morbidity and comorbidity of these two chronic metabolic diseases along with the rapid socioeconomic and lifestyle changes that have occurred in recent decades, thereby imposing a huge burden on human health and society.
China has a special geographical distribution and socioeconomic differences. The composition and distribution of the population are complex. Many studies have shown differences in the prevalence of T2D and NAFLD between different regions and between different populations. 31 Based on the data of the China Noncommunicable Disease Surveillance 2010, a national health survey of 109,023 adults older than 18 years, an 11.6% overall prevalence of diabetes 32 was reported, with a twofold geographic variation in diabetes prevalence across China. Within the northern region, the prevalence of diabetes ranged from 9.1% (northwest) and 9.9% (northeast) to 15.7% (north). A systematic review of population-based surveys showed a correlation between the economy and the prevalence of fatty liver disease in China, increasing at a mean rate of 0.594% per year. 4 Recently, a meta-analysis including 2 million of participants from 392 studies showed that the overall estimated prevalence of NAFLD was 29.2% in China, stratified by age, sex, body type, socioeconomic status, and geographical region, especially with the higher prevalence in the northwest region. 28 Our findings confirm the previous studies of a higher prevalence of NAFLD in the northern region of China than in the south. In fact, we may have underestimated the prevalence of NAFLD in this population because 20% of the participants who were hepatitis or heavy drinkers were excluded. Pinggu, close to Beijing, the capital of China, is a suburban community that is undergoing rapid gentrification. Both urban and rural populations have experienced rapid economic improvements and changes in their daily lives. A westernized diet and sedentary lifestyle, along with the consequent epidemic of overweight (40.52%) and obesity (28.92%), have probably led to the rapid increase in the burden of metabolic disease in this population.
Although the BMIs of the T2D group and NAFLD group were above average, individuals with lean fatty liver or nonobese diabetes are also numerous. Many studies have shown that despite a lower mean BMI and waist/hip ratio, East Asians have a relatively higher possibility for the progression of NAFLD and T2D than those with similar body type in Western countries. 33,34 One plausible explanation is the greater genetic predisposition to hepatic fat deposition and pancreatic islet cell dysfunction. 35,36 The underlying hereditary and environment reasons for NAFLD and T2D predisposition in the Chinese population warrant further investigation. In this analysis, we did not observe significant differences in liver function levels (AST/ALT) between participants with or without NAFLD. It is likely that the prevalence of fatty liver has only increased rapidly in the past decade and has not caused serious hepatic damage. In addition, patients coexisting with alcoholism and viral hepatitis were excluded, which may cause some patients with abnormal liver function to be excluded from the analysis. Although ultrasound is the most commonly used diagnostic tool for fatty liver, it is incapable of detecting steatosis at degrees <20%. 4,37 Here, the CT could noninvasively measure the hepatic fat content at a steatosis degree as low as 5%, to identify morbid and moderate NAFLD individuals with normal enzymatic indicators. 4,37
The prevalence of NAFLD among patients with diabetes or abnormal glucose tolerance is higher than that among the general population. In patients with T2D, the prevalence of NAFLD can be as high as 70%. 38 The SPRINT study reported 56.5% NAFLD in T2D patients with higher prevalence in females (60%) than in males (54.3%) and with prevalence of NAFLD varying from 44.1% in western India to 72.4% in the northern state.39 Similarly, in the current population, nearly 40% of diabetes patients had NAFLD; notably, more than half of the younger diabetes patients suffered from fatty liver. In addition, it should not be overlooked that a large number of prediabetes patients, accounting for nearly a quarter of the analyzed population, will be the reserve population for diabetes and fatty liver. Although previous studies have reported a significant increase in the prevalence of NAFLD in prediabetic populations, few studies have conducted detailed subgroup analyses according to glucose intolerance strata. 14 Here, we identified fatty liver using the CT scan and classified the strata of glucose metabolism by standard OGTT and found that nearly a quarter of residents were in a prediabetic state, of which approximately one-third had NAFLD, especially men with IGT or IFG+IGT. Multivariate regression analyses after adjustment for potential confounders also showed that the odds of NAFLD in patients with IGT or IFG+IGT increased by approximately three times, close to that of diabetics. Jimba et al. showed that the prevalence of NAFLD in diabetic patients increased with elevated fasting glucose levels. 40 In the JSG-NAFLD study with 1365 biopsy-proven NAFLD patients, T2D was shown to be a significant risk factor for advanced liver fibrosis. 41 These results indicated that with the deterioration in glucose metabolism from NGT, prediabetes to diabetes, the incidence of NAFLD increased gradually. Hyperglycemia combined with NAFLD is often associated with severe lipid disorders and insulin resistance and an increased difficulty of obtaining stable blood glucose control. 5 However, despite mounting evidence pointing to the importance of “vicious cycle” between obesity and insulin resistance in modulating the development of T2D and NAFLD, 6 much remains unexplored about the mechanisms by which these two diseases interact at an early stage.
To the best of our knowledge, this is the first community-based study investigating the morbidity and comorbidity of NAFLD and different glucose intolerance strata in a large and well-characterized population in China. However, the baseline data of the study limited our ability to infer causal relationships between fatty liver and glucose metabolism. In addition, the current study population is from northern China. Due to differences in regions, ethnicities, and lifestyles, the data of this study cannot be generalized to all of China or other regions. More large-scale longitudinal studies are needed in the future to explore the relationship between these two common metabolic diseases.
In short, the high morbidity and comorbidity of T2D and NAFLD in the Pinggu community of Beijing in northern China emphasize the importance of early prevention and treatment of these two metabolic diseases at the same time.
Footnotes
Acknowledgments
We thank all the participants and investigators in this study.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This work was funded by a grant from the Beijing Science and Technology Committee (D131100005313008) and the NIH research training grant R25 TW009345 funded by the Fogarty International Center. This study was also supported by Sanofi China.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.