
Abstract
Background:
Pioglitazone is an effective treatment option in clinical practice for managing type 2 diabetes mellitus. It is challenged by a lot of adverse effects, primarily body weight gain, peripheral edema, as well as congestive heart failure.
Case Report:
This is a case of a 76-year-old woman with no evidence of cardiac disease, who developed edema as well as bilateral pleural effusion after using pioglitazone. She got a weight decrease and complete resolution of the pleural effusion after stopping use of pioglitazone and rational use of diuretics.
Conclusion:
Common side effects of pioglitazone have been widely reported. However, little attention was drawn on pleural effusion in diabetic patients with no pre-existing heart dysfunction. In this case, we show the use of pioglitazone results in pleural effusion, with emphasis on the clinical recognition and management.
Introduction and Background
Pioglitazone, a member of thiazolidinediones, predominantly functions as an insulin sensitizer by activating nuclear peroxisome proliferator-activated receptor-γ (PPAR-γ) in peripheral and hepatic tissues. 1 Food and Drug Administration approved pioglitazone for the treatment of type 2 diabetes mellitus (DM) in 1999. 2 In clinical practice, the common adverse events such as fluid retention, weight gain, bone loss, and congestive heart failure have been well documented. 3 However, few cases of pleural effusion have been reported in the literature in patients with normal cardiac function. 4,5
Case Report
A 76-year-old woman was diagnosed with type 2 DM 20 years ago. She started injecting Novolin 30R about 5 years ago. Owing to suboptimal glycemic control, she stopped Novolin 30R and received insulin Lispro, pioglitazone (15 mg once a day) in combination with acarbose (50 mg three times a day) last year. The patient was on olmesartan to treat hypertension and aspirin to treat cerebral infarction in addition. She came to the outpatient department for progressive swelling and breathlessness 1 week ago. Pioglitazone was discontinued although she had not got other treatment for the dyspnea. She felt that breathlessness was slightly better but still suffered from edema. She had no paroxysmal nocturnal dyspnea during the course of the disease.
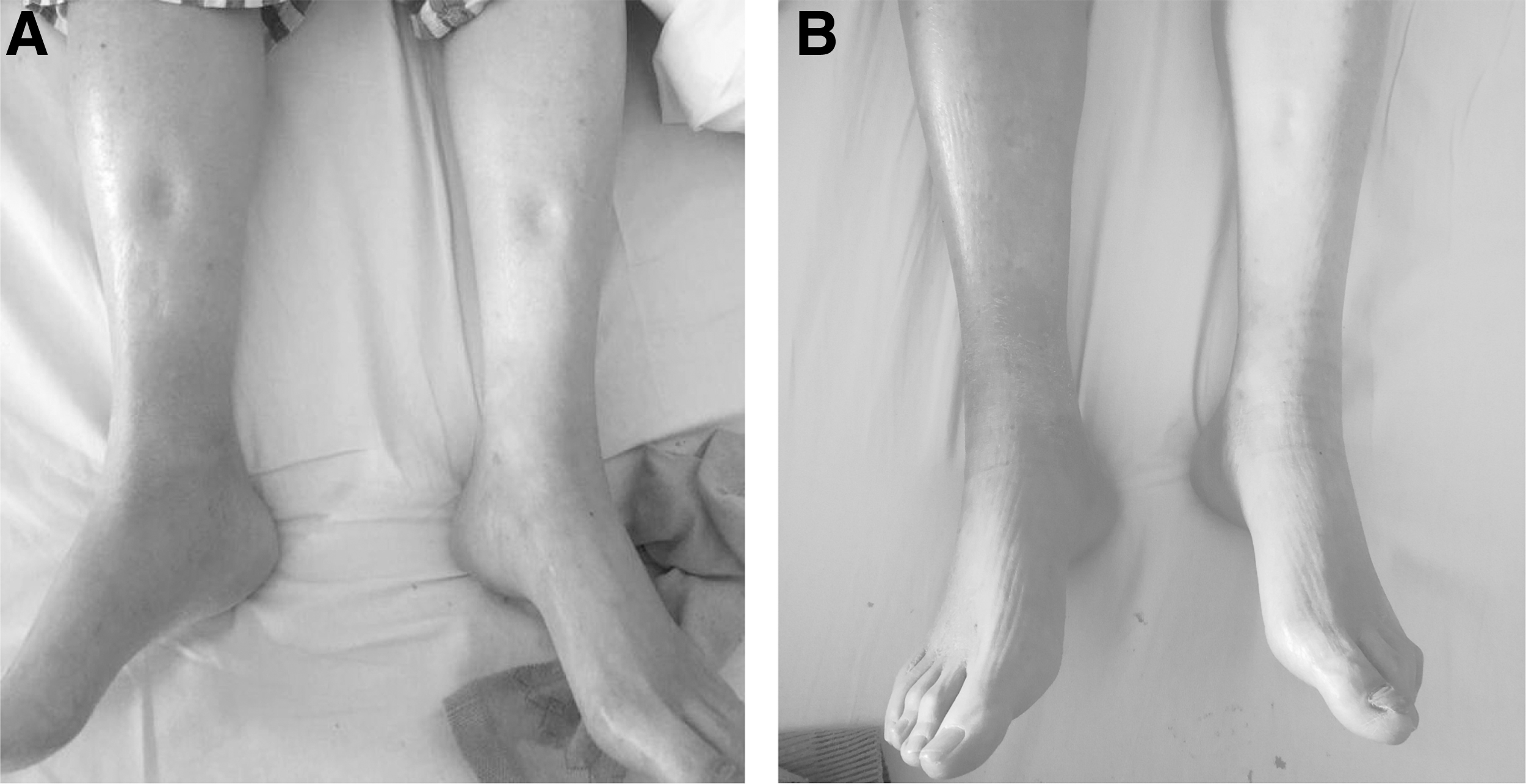
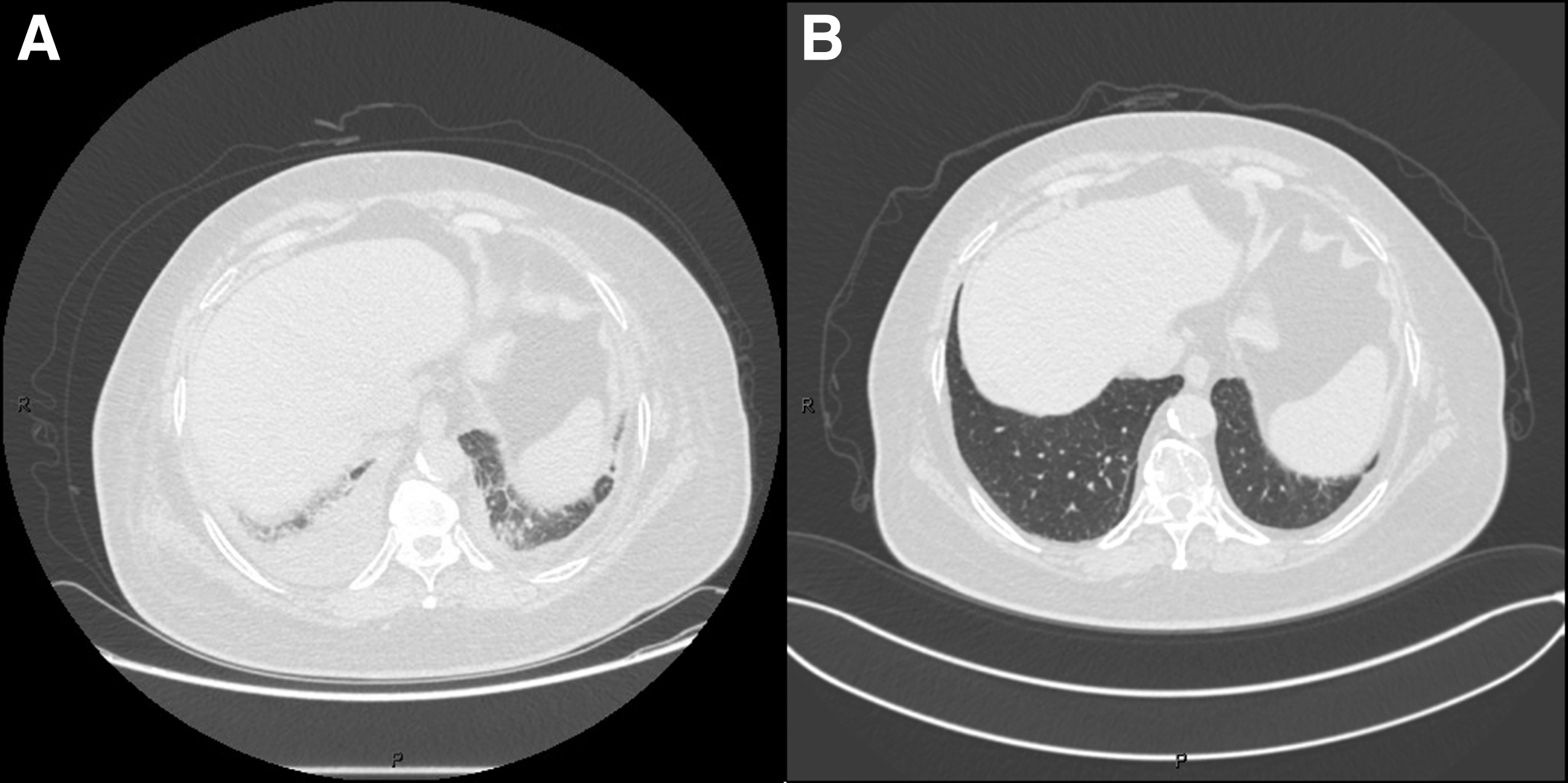
On arrival, her vital signs were stable with no evidence of hypoxemia. Physical examination revealed there were no extra heart sounds, jugular venous distension, hepatojugular reflux, or other classic signs of heart failure. But she displayed pitting edema of the extremities (Fig. 1A). The breath sounds were diminished in both lower lung fields and no rales were heard. Chest computed tomography (CT) showed moderate bilateral pleural effusion (Fig. 2A). Subcutaneous edema in abdominal were also found by abdominal CT scan. Her laboratory findings showed that erythrocyte sedimentation rate were elevated, but C-reactive protein and procalcitonin were unchanged from baseline. Albumin, full blood count, serum electrolytes, liver functions, renal functions, and urine albumin creatinine ratio were in the normal range. Serum autoantibodies and antineutrophil cytoplasmic antibodies were negative. No ascites or organic abnormality was found on the abdominal CT other than gallstone. Echocardiography demonstrated normal ventricular function with an ejection fraction of 65%.
Serial chest computed tomography:
A presumptive diagnosis of pioglitazone-induced pleural effusion was made as she had no pre-existing evidence of cardiac disease or fluid overload before use of pioglitazone. Pioglitazone was discontinued and the patient was treated with furosemide 20 mg and spirolactone 20 mg at 12 hours intervals immediately. We also restricted her fluid and salt intake. After 7 days, She got a weight decrease from 80 to 72 kg (Fig. 3), and the anasarca and dyspnea began to improve (Fig. 1B). On subsequent follow-up (1 month later) in the outpatient department, she had no breathing difficulties, and her weight was dropped to 68 kg. The chest CT showed complete resolution of the pleural effusion (Fig. 2B).

The associated weight change during hospitalization.
Discussion
In clinical practice, pioglitazone is the most commonly used thiazolidinedione drug that improves insulin resistance in type 2 DM by activating PPAR-γ. It can reduce the risk of stroke or myocardial infarction in patients without diabetes who had insulin resistance along with a recent history of ischemic stroke. 6 Compared with glimepiride, pioglitazone results in a significantly delayed progression of coronary atherosclerosis in patients with type 2 diabetes and coronary artery disease. 7 Pioglitazone also exerts favorable effects in patients with nonalcoholic steatohepatitis. 8 As all the other drugs, pioglitazone has some side effects that include edema, weight gain, bone loss, congestive heart failure, and the risk of bladder cancer. 9 It has been shown in a meta-analysis that pioglitazone monotherapy was significantly associated with risk of peripheral edema in type 2 DM patients. 9 The incidence of edema was higher, in particular among patients who were treated with oral hypoglycemic agents or insulin at baseline. 3
Renal sodium retention 10 and vascular permeability 11 may contribute to pioglitazone-induced edema. It has been reported edema in feet, ankles, and legs as a complication of pioglitazone in most studies, 12 whereas pleural effusion is uncommon and has rarely been reported. In fact, pleural effusion, a special type of edema, is an unusual amount of fluid collected in the pleural space. In our case, we ruled out other diseases that may cause pleural effusion, such as heart disease, kidney disease, vascular disease, as well as rheumatic diseases. Insulin edema is a rare complication of insulin therapy and usually occurs in patients with type 1 DM. 13 It has been mainly attributed to insulin's anabolic action, increased vascular permeability, and altered renal sodium processing. 14 Insulin changes the permeability of sheep pleura and may interfere in pleural effusion formation. 15 Pleural effusions have rarely been reported and were usually presented 4 weeks after use of insulin. 13,16,17 In previous reports, patients were found to have pleural effusions after 5 months using pioglitazone in combination with other oral hypoglycemic agents. 4 There were no reports of pleural effusion caused by the combination of insulin and pioglitazone. Our patient started insulin therapy 5 years ago, and she did not have any obvious symptoms of edema and breathing difficulties at that time. She developed symptoms of pleural effusion 1 year after the combination of pioglitazone, acarbose, and insulin. Her body weight decreased significantly before discontinuing insulin injection. Studies have shown that the edema caused by pioglitazone can be aggravated by combination of insulin, 3,18 which may further cause pleural effusion. Although we cannot completely rule out the possibility that the interaction with insulin may contribute to the edema caused by pioglitazone and eventually lead to pleural effusion, we should think of potential possibilities of pleural effusion in patients receiving both pioglitazone and insulin.
After pioglitazone was discontinued and diuretics were used, the patient got a distinct weight decrease as well as the improvement of anasarca and dyspnea. She got a score of seven points based on the patient's Naranjo adverse drug reaction probability scale, 19 which suggested that there was a probable association between the use of pioglitazone and pleural effusion (Table 1). Animal study reported the diuretic spironolactone could attenuate rosiglitazone effects on volume expansion. 20 Spironolactone may be particularly effective in preventing or treating edema and pleural effusion induced by pioglitazone. Fluid and salt restriction are also necessary. 17
Naranjo Adverse Drug Reaction Probability Scale
Probability category: 0–3 = doubtful; 1–4 = possible; 5–8 = probable; ≥9 = definite.
In conclusion, for patients taking pioglitazone, especially those who use insulin at the same time, all possible side effects should be carefully monitored. When the patient has symptoms of edema and shortness of breath, clinicians should call to mind the possibility of pleural effusion.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This project was supported by Shanghai Municipal Education Commission-Gaofeng Clinical Medicine Grant Support (20181807), National Natural Science Foundation of China (81670728), Shanghai Pujiang Program (2019PJD027), Shanghai Renji Hospital Grant (RJKY17-01), and Shanghai Jiaotong University Grant (CHDI-2019-A-01).