
Abstract
Background:
Glucagon-like peptide-1 agonists (GLP-1) reportedly lower HbA1c and promote weight reduction and improve cardiovascular outcomes. The primary objective of this study was to evaluate the use of GLP-1 agents in patients and changes in HbA1c, weight loss, blood pressure, and lipoid profiles.
Methods:
Patient information was extracted from a regional Veteran Affairs data mart. Patients were included if they had prescriptions for at least 90 days of a GLP-1 between April 1, 2005, and December 1, 2016, and HbA1Cs and weights at both baseline and within first 15 months of therapy. Blood pressure and lipids were also measured. Pearson's correlation and multiple regression analysis were used.
Results:
Three hundred twenty-two patients met inclusion criteria. Average HbA1c decreased by 0.81% and weight by 4.4 kg. At 1 year, 160 patients had both weight and HbA1c measured, and of those, 92 (58%) patients had HbA1c reduction of at least 0.5% and 94 (59%) patients had <−2 kg change in weight. Fifty-seven (36%) patients met both of those outcomes. Veterans who met both weight and HbA1c outcomes were slightly, but significantly, older than those who did not meet both. No correlation was found between weight and HbA1c change at each quarter (P > 0.05); however, weight change was correlated with systolic blood pressure change (P = 0.03). Multiple regression for meeting weight and HbA1c target outcomes, and changes at quarters 1–3, all correlated to success at 1 year (P < 0.05).
Conclusions:
Weight change was independent of HbA1c changes in patients receiving GLP-1s for diabetes control. Weight loss was associated with decreases in systolic BP.
Purpose
The primary purpose of this retrospective, observational study was to examine whether weight changes should be considered when determining appropriateness of glucagon-like peptide-1 agonist (GLP-1) therapy. Secondary objectives were to assess weight changes, HbA1c changes, and their effect on cardiovascular health markers, as well as examining provider adherence to current GLP-1 criteria.
Background
Diabetes and obesity are major health problems in the United States, and the prevalence continues to increase. 1 In 2011, the CDC estimated 70.7% of the U.S. population were either overweight or obese, and ∼8%, around 26 million people, had diabetes. By 2014 estimates, the number of people with diabetes had grown to 9.1%, around 29 million people. In contrast, the U.S. Department of Veteran Affairs (VA) estimates 24% of veterans have diabetes, a much higher prevalence than the general population. 2,3
GLP-1, also known as incretin mimetics, are newer antidiabetic agents that are quickly gaining favor not only for their effects in lowering HbA1c but also in reducing weight. In addition, they have evidence of improving the cardiovascular profile as related to blood pressure reduction and improved lipid profile as well as reduced risk of cardiovascular events in certain populations. 4 –7 The 2015 American Association of Clinical Endocrinologists and American College of Endocrinology (AACE/ACE) diabetes guidelines now recommend GLP-1 analogs as second-line agents after metformin, along with sodium-glucose transport protein 2 (SLGT2) inhibitors, dipeptidyl peptidase-4 (DPP4) inhibitors, and alpha-glucosidase inhibitors. 5
In general, GLP-1 agonists appear to reduce weight and lower HbA1c in a dose-dependent manner, but that is not universally true: literature demonstrates liraglutide 1.8 mg increased HbA1c, while reducing weight, and there is no clear connection between weight and HbA1c reduction. 8 –10
Weight loss alone can decrease HbA1c, but very few studies have examined the relationship between weight and HbA1c reduction. Available studies that have examined the relationship have yielded variable results. One small cohort study with 120 patients examined the average weight loss to achieve a reduction in HbA1c. 6 They found that participants who were more obese at baseline had to lose a greater percentage of body weight to achieve the same HbA1c reduction. GLP-1 agonists may improve hyperglycemia by weight loss, but some meta-analyses of certain GLP-1 agonist trials were only able to find tenuous associations between weight loss and HbA1c reduction. In addition, there are few trials examining the effect of body mass index (BMI) and metabolic factors on how well people respond to GLP-1 and whether weight change may affect cardiovascular markers.
The VA recently relaxed the criteria for use of GLP-1s in 2016 which may result in an increase in utilization. 11 VA patients are now eligible for GLP-1s if they have type 2 diabetes and inadequate glycemic control on two medications, one of which should be metformin unless contraindicated or not tolerated. Once started, there is little guidance on when to evaluate benefits of therapy and consideration of alternate agents or discontinuation. GLP-1 use criteria from a non-VA health care institution as well as NICE guidance on diabetes management provide more specific guidance and evaluate both weight changes and glycemic control. 12,13 To continue a GLP-1 agent, patients need to have both a HbA1c reduction of ≥0.5% and a weight reduction of ≥2kg (4.4 lbs.).
GLP-1s are costly medications with limited data on their effectiveness in the veteran population. Some veterans may not receive full benefit from GLP-1s, and would receive similar benefits with DPP4 inhibitors or other more cost-effective antidiabetic medications.
Methodology
Research plan
This retrospective, observational study examined the information of patients receiving GLP-1 from the five VA stations in the Veterans Integrated Service Network 21 (VISN 21). In addition to the VA Northern California Health Care System (VANCHCS), VISN 21 includes the Palo Alto, San Francisco, Sierra Nevada, and Pacific Islands Health Care Systems. We analyzed the information from these patients to see whether patients were meeting the specific criteria from the non-VA guidance on average. The information was also examined to assess weight changes and if those were correlated to HbA1c changes, as well as whether changes in earlier quarters were correlated to achieving glycemic target outcomes as well as both glycemic and weight outcomes. This will help clarify when to assess HbA1c changes and whether to consider weight changes when looking at GLP-1 therapy for diabetes. Changes in HbA1c and weight, as well as blood pressure and lipid values were also correlated to see whether benefits in either may be potentially contributing to cardiovascular outcome improvements.
Data collection
Structured query language (Microsoft, Redmond, WA) was used to extract data from the VISN 21 data mart, including demographic data such as age, sex, ethnicity (self-described), weight, BMI, and medications, including GLP-1s, all diabetes medications, lipid medications, blood pressure medications, and antipsychotics. HbA1c, weight, blood pressure, and lipids were also extracted. Lipids included total cholesterol, low-density lipoprotein (LDL), high-density lipoprotein (HDL), and triglycerides (TG). Medication fill dates and quantities were extracted; the day supply and days between fills were compared to calculate the medication possession ratio for adherence.
Data analysis (statistical analysis)
Descriptive statistics was used to report demographic data and to summarize key findings. Average changes and number of patients that met target outcomes taken from non-VA criteria: HbA1c reduction of ≥0.5% and a weight reduction of ≥2 kg (4.4 lbs.). Pearson correlation was used to assess relationship between weight changes and HbA1c changes, as well as changes in blood pressure and lipids. Multiple regression analysis was used to assess relationship of changes in weight at quarters 1–3 and quarter 4, the final evaluation point. The Mann–Whitney rank sum test was used to assess differences in the groups who achieved target outcomes as above, and the groups who did not. BMI, age, baseline HbA1c, sex, insulin use, and exenatide versus liraglutide were also assessed
Study period
Data regarding GLP-1 use, laboratory, and other measures were extracted from the regional data warehouse, from patients who were on GLP-1 from April 2005 to December 2016. The final analysis was completed in May 2017.
Subject Population
Adult patients (≥18 years) were included in this retrospective observational study, and both male and female patients were included. No ethnic groups were excluded. All adults who met inclusion criteria were included, a final of 322 patients were examined. These criteria included the following: age ≥18 years; received at least 90-day supply of GLP-1 from the following VA stations: Northern California, Sierra Nevada, Palo Alto, San Francisco, and Pacific Islands; adherence ≥80% based on medication possession ratio; baseline weight and HbA1c within 6 months before starting GLP-1; and at least one weight and HbA1c in the same quarter within 455 days (1 year +90 days). Patients were excluded if any of the following conditions was met: age <18 years and did not meet above inclusion criteria. Vulnerable research subject criteria were considered not applicable, since we conducted a retrospective analysis. Ethnicity was extracted from the VA database; Veterans self-identified as non-Hispanic White, Native Hawaiian/other Pacific Islander, Asian, Hispanic White, declined to state, Black, Unknown, American Indian/Alaska Native, or Null.
Results
Three hundred twenty-two patients who met criteria as above were included in this retrospective, observational analysis. Thirty-two patients trialed greater than one GLP agonist. Each course of therapy was analyzed separately. Table 1 summarizes key demographic parameters of the patients.
Patient Demographics
GLP-1, glucagon-like peptide-1 agonists.
The majority of patients included were older male adults, average BMI was in obese range, many were on multiple diabetes medications, including insulin, and most were already on antihypertensives and lipid-lowering medications. Most patients were on liraglutide or exenatide, the GLP-1 agents that have been on the market the longest.
Review of dosing data for baseline hypoglycemic medications (primarily metformin and the sulfonylureas glyburide and glipizide) showed that 19 patients were able to reduce metformin doses, 20 were able to reduce sulfonylurea doses, 2 reduced both classes, but 12 had to increase metformin dose and 11 sulfonylurea dose. The average metformin dose decrease was 759 mg daily, but the average increase was 731; for glipizide, 11.75 mg decrease and 9.8 mg increase; and for glyburide, 11.6 mg drop, but a 10 mg increase. Overall, the average daily dose of metformin before GLP agonist therapy was 1877.7 ± 480 mg, and 1848 ± 465 mg after; for glipizide, 19.4 ± 10 mg pre-GLP and 19.2 ± 12.5 post-GLP, and for glyburide, 17.1 mg ±4.8 pre-GLP and 16.3 ± 5.4 mg post-GLP. These changes were not significant.
Ethnicity data were tabulated and revealed 55.1% non-Hispanic White, 12.7% Native Hawaiian/Other Pacific Islander, 11.2% Asian, 8.1% declined to state, 4.3% Black, 3.1% Hispanic White, 3.4% Unknown, 1.2% American Indian/Alaska Native, and 0.6% Null.
Changes in glycemic control, weight, and cardiovascular indicators
Table 2 summarizes the baseline and changes in measures after 1 year of GLP-1 therapy. At 1 year, the average change in weight and HbA1c was −4.4 kg and −0.81%, respectively, which meets the non-VA criteria to continue GLP-1s. The changes in blood pressure and lipid measures were small. The systolic blood pressure decreased by 0.44 mmHg on average, the diastolic blood pressure increased by 0.49 mmHg, the total cholesterol decreased by 0.56 mg/dL, LDL decreased by 2.2 mg/dL, HDL decreased by 0.7 mg/dL, and TG decreased by 8.0 mg/dL. All changes had large standard deviations when compared to actual changes. Changes in HbA1c and cholesterol were statistically significant, while changes in weight and TG approached significance.
Baseline and Changes in Measures
HDL, high-density lipoprotein; LDL, low-density lipoprotein; SD, standard deviation.
Patients meeting one or both target outcomes after 1 year of GLP-1 therapy
Table 3 displays the number of patients meeting each target outcome and the number meeting both. Figure 1 shows the proportion of patients who met each target and the patients who met both outcomes separately. In more than half of the treatment courses analyzed, patients met the weight target of ≥2 kg weight reduction (59%), and a similar portion met the glycemic control target of ≥0.5% HbA1c reduction. Patients who met both targets were less common (36%), and 19% patients using GLP-1 had did not meet either. Eighty-four patients did not have the required labs.
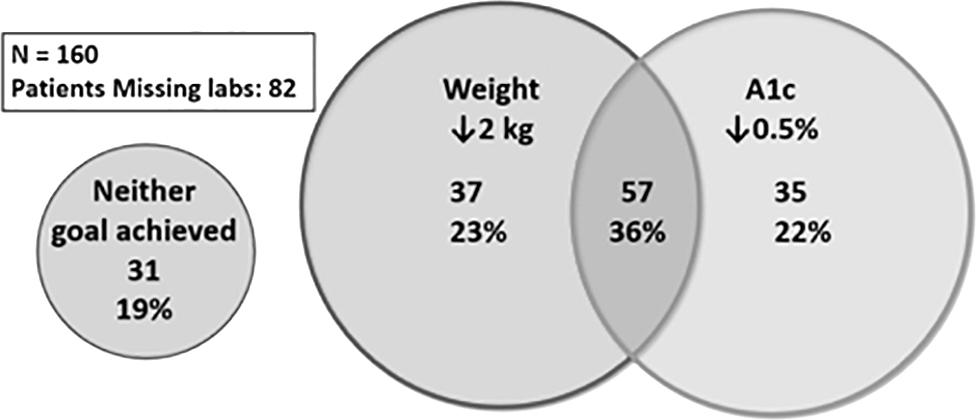
Outcome after 1 year on GLP-1 receptor agonists. Data are shown for 160 patients for whom weight and HbA1c data were available before and after 1 year of continuous therapy. Data are shown for those who achieved neither weight nor HbA1c goals, both, or one or the other. GLP-1, glucagon-like peptide-1 agonists.
Number of Patients with Decrease in Weight and/or A1c
Correlation of weight change and glycemic control
The change in weight and HbA1c was assessed with Pearson correlation, the results summarized in Table 4. There was no significant correlation between weight change and HbA1c change at any of the quarters assessed. Figure 2 shows weight and HbA1c at each quarter of treatment. HbA1c dropped dramatically early, while weight was relatively constant over the time course for the pooled population.

Weight and HbA1c data are shown at each quarter of continuous therapy with GLP-1 receptor agonists.
Correlation Between HbA1c and Weight Change
Impact of other medications that could impact glycemic control
By definition, all patients in the study cohort were on other diabetes medications at the onset. The majority were on metformin (78%) or sulfonylurea (44%). While it is difficult to track each prescription, or use patterns (since patients sometimes modify dosing without it being reflected in the medication order), it appears that doses of these oral hypoglycemics were unchanged. Insulin titration was also not assessed. Other medications known to impact glycemic control, such as statins, or certain hypertension medications, were not tracked in this analysis.
Correlation with cardiovascular markers after 1 year of GLP-1 therapy
Weight change as well as HbA1c change and changes in cardiovascular markers (blood pressure and lipids) were assessed with Pearson correlation, as summarized in Table 5. Most indices did not meet statistical significance, but weight changes and systolic blood pressure were correlated (P = 0.03).
Correlation of Weight or HbA1c Change and Cardiovascular Markers
Logistic regression analysis of earlier quarters on success after 1 year of GLP-1 therapy
Whether changes at quarters 1–3 were correlated to meeting either both weight and HbA1c target outcomes or the HbA1c outcome was assessed using logistic regression analysis, and results are summarized in Table 6. Changes at all quarters were important in determining success (meeting criteria) after 1 year of GLP-1 therapy. Both HbA1c and weight changes were correlated to meeting both targets (P ≤ 0.05), while only HbA1c changes were correlated to meeting the HbA1c targets.
changes at Quarters 1–3 Correlated to Meeting Target Outcomes
Differences between patients who met both target outcomes versus patients who did not
Patients who met both the weight and glycemic targets were compared to those who did not using Mann–Whitney rank sum test since the data were not normally distributed. These results are shown in Table 7. The only statistically significant finding was a difference in age (P = 0.045). The mean age of patient who did meet both target outcomes was 69 and mean age of those who did not was 68.
Differences Between Groups: Patients Meeting both Target Outcomes Versus Patients Not Meeting Both Targets
Discussion
Our observational retrospective study suggests that while GLP-1 agents are effective for both weight loss and glycemic control, they do not benefit everyone equally. The number of patients meeting the threshold of weight loss recommended by non-VA criteria was similar to the number for HbA1c reduction, but there was only a 61%–62% overlap in people who met both target outcomes. This distribution is very close to the expected distribution if these two measures were independent (58%–59%), suggesting that weight loss and glycemic control are independent processes. Other data that support this are that at each quarter, the weight change and HbA1c change were not correlated, and that weight change does not contribute to success in decreasing HbA1c by at least 0.5%. 10 Umpierrez et al. examined the data from six clinical trials of dulaglutide at the relationship between weight change and glycemic control in patients on dulaglutide; weight loss and HbA1c reductions were found to be dose dependent, but have very weak correlation, and appeared to be independent. 10 This conclusion is similar to the one reached by Blonde et al., who examined eight trials using exenatide once weekly. 14
Some studies have explored the notion that ethnicity may impact the response to GLP-1 agonists, particularly for East Asian patients. 15 –17 For example, Blundell et al. have proposed that Japanese participants would lose less body mass overall than a heavier and/or obese cohort, as ∼80% of weight lost with semaglutide treatment is fat mass. 15 This would be further influenced by the Japanese diet.
These efficacy results might also be considered in the context that, in East Asia, t2dm is characterized by significant β-cell dysfunction with less adiposity and less insulin resistance than in Western populations. Consequently, incretin-based drugs may show more efficacy in Asian populations, mostly because of amelioration of β-cell dysfunction. 16,17
While our population showed a substantial portion of patients who identified as Asian or Native Hawaiian/Other Pacific Islander in keeping with the Western United States location of our VISN, we do not know how many of those patients live on the mainland or consume a western or traditional diet. Thus, while it is tempting to speculate that some of our results may reflect ethnic differences, we do not have sufficient data to explore those relationships further. On the other hand, some investigators do not believe there is much ethnic or racial impact on the efficacy of these medications. 18
The “business rules” in effect at the time we started the study mandated we add GLP-1 agents to existing glucose-lowering therapy. The available data suggest that overall, while there were no significant changes in doses of other hypoglycemic medications, it is difficult to assess impact of medication changes in an individual patient. Our data do not allow us to analyze the glucose-lowering contribution of lipid-lowering or antihypertensive medication to the outcomes we measured. This is a limitation of our study.
Weight changes while on GLP-1 were found to be correlated to systolic blood pressure in our study, but the other markers of cardiovascular health did not include diastolic blood pressure and lipids. Blonde et al. 14 examined whether weight loss contributed importantly to cardiovascular risk markers, including blood pressure, lipids, liver enzymes, and heart rate. They found that patients with larger weight loss experienced greater improvements to all cardiovascular risk markers other than diastolic blood pressure. Weight loss alone can contribute to improvements in cardiovascular markers as well as improved cardiovascular outcomes, and it is unclear what additional benefits GLP-1 agonists confer. In large cardiovascular outcomes trials, liraglutide is shown to improve cardiovascular outcomes in the LEADER trial, but lixisenatide had a neutral effect on cardiovascular outcomes. 19,20 Liraglutide is one of the GLP-1 with the highest weight loss, while lixisenatide has a more modest effect. Further study is necessary to elucidate the relationship between GLP-1, weight loss, and cardiovascular outcomes.
We conclude that weight changes minimally affect glycemic control and when GLP-1 agents are used for diabetes control, assessments of any change to weight are unnecessary. If patients are overweight and receiving weight benefits without glycemic benefits, consideration should be made to adjust the GLP-1 dose to that for weight loss, and help the patient modify other lifestyle factors like diet and activity to receive maximal benefit of losing weight.
While weight loss is often a key component of nutritional therapy for diabetes, it has been recognized for some time that weight loss is not always associated with improved glycemic control, and dietary interventions focusing on HbA1c lowering may be more effective than those focusing on weight loss. 21
Some investigators have pointed out that outcome differences between different GLP-1 agents could be due to their derivation. Some, such as exenatide, are derivatives of exendin-4, while others, such as liraglutide, are considered derivatives of native human GLP-1. These differences may impact half-life, and potentially other clinically significant outcomes. 22,23 The agents primarily used in our population were liraglutide and exenatide, and our data do not allow us to distinguish if the outcomes might be related to their proposed differences of origin.
GLP-1 agents impact glucose homeostasis by affecting insulin and glucagon secretion, satiety, and gut motility. 24 Bear in mind that glucose homeostasis reflects the interaction of glucose absorption, de novo hepatic production, insulin secretion, and insulin action at liver, fat, and muscle. While these effects are relatively well understood, the effect on weight loss is less clear and may be multifactorial. Recall that weight homeostasis involves appetite, food digestion and absorption, as well as energy expenditure at rest, in response to eating, and with activity. For example, GLP-1 agonists impact the brain-adipocyte axis in humans and rodents, affecting both caloric intake and energy expenditure. 25 –27 The melanocortin-4 receptor, present in the hypothalamus, is involved in appetite regulation; liraglutide has been shown to both upregulate the pertinent gene in mice 28 as well as be active in obese humans who lack the melanocortin-4 receptor pathway. 29 The hepatic expression of adenylate cyclase 3 is regulated, in mice, by liraglutide. 30 In addition, liraglutide has been demonstrated to modulate gut microbiota in obese and obese diabetic rats. 31 It is also likely that while different mechanisms of weight loss have been proposed, there is no reason to anticipate they would not act in parallel in any individual.
These novel agents appear to have significant cardiovascular benefits as well, which appear to be distinct from their effects on glycemic control and weight. 32,33 Nonglycemic effects of these drugs have been summarized elsewhere. 34
It would thus be naive to imagine that the weight loss and glycemic effects of GLP-1 agents would be similar in magnitude and would co-exist in individual patients. Our findings are consistent with this reality, as is the developing use of these GLP-1 agents for either diabetes control or weight loss, or both. While clinicians and patients may see improved outcomes, pharmacy benefits managers will have ongoing challenges in evaluating the proper use of these agents.
Footnotes
Disclaimer
The contents do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This material is the result of work supported with resources and the use of facilities at VA Northern California Health Care System.