
Abstract
Background:
Lifestyle intervention programs comprise the first-choice therapy to reduce the cardiovascular risk factors in metabolic syndrome (MetS). Our aim was to compare the effects of three lifestyle modification programs on the number of diagnostic criteria and clinical parameters of MetS.
Methods:
Twelve-week clinical trial, including 125 adults who presented at least three of the criteria defined by the revised NCEP ATP III (National Cholesterol Education Program Adult Panel III) for MetS. Individuals were randomized into three multidisciplinary intervention groups: Standard Intervention (SI), Group Intervention (GI) and Individual Intervention (II).
Results:
Seventy-one individuals, aged 34–59 years, concluded the study: SI: 20, GI: 25, and II: 26. The GI and II groups presented a significant decrease of body mass index, abdominal circumference, diastolic and systolic arterial pressure after intervention. The number of diagnostic criteria for MetS decreased significantly. Within the GI and II groups, 16.0% and 15.4% of the individuals, respectively, did not meet the criteria for the clinical condition studied at the end of the interventions. In the II group, the percentage of individuals with five criteria reduced 83.5%. In the GI group, the percentage of individuals with five criteria remained the same, but the number of individuals with four criteria presented a 50.0% reduction.
Conclusions:
Results reinforce that nonpharmacological strategies for changing lifestyle affect the reduction of cardiovascular risk factors existing in MetS. They are also able to remove the population from this clinical condition by decreasing the diagnostic criteria. II or GI lead to a successful treatment of MetS, especially when conducted by multidisciplinary team.
Brazilian Registry of Clinical Trials-ReBEC number: RBR-9wz5fc
Introduction
Metabolic Syndrome (MetS), a complex set of cardiovascular risk factors related to abdominal fat and resistance to insulin, is strongly associated with high cardiovascular morbimortality. 1 –3 In the United States, the prevalence of MetS, when adjusted for age, is 22.5%. 4 The estimated global prevalence is one quarter of the world population, meaning that more than a billion people are affected by MetS. 5
The diagnostic components' criteria of MetS are primarily attributed to an unhealthy lifestyle, which is a modifiable risk factor. The first-choice therapy for prevention and treatment of MetS comprised lifestyle modifications through a multifactor approach based on healthy diet, physical exercise, and pharmacological strategies. 6 Programs of lifestyle change including supervised physical exercise and nutritional education were able to achieve the proposed goals for the treatment of MetS. 7,8 Researchers have been exploring various strategies including lifestyle modification programs to demonstrate robust scientific evidence of the effectiveness on progression of MetS diagnostic criteria, but the best intervention model remain inconclusive. 9
The hypothesis tested in the present study is that there is a variation in the diagnostic criteria and clinical parameters involved in MetS, when comparing different interventions on lifestyles. Thus, the aim of this study was to test three different programs with a multidisciplinary approach to lifestyle change to answer if there is a difference on the number of diagnostic criteria and clinical aspects of MetS.
Methods
Study participants
The study participants were recruited from the Rehabilitation Center of the Pontifical Catholic University of Rio Grande do Sul (PUCRS), Brazil, in 2012. The trial included 125 adults of both sexes, selected through dissemination in the media. Volunteers to participate in the study attended a screening session and those who met the following inclusion criteria were included: aged 30–59 years, present at least a 5-year education background, diagnosis of MetS, and no previous cardiovascular events. Exclusion criteria: contraindication for physical activity, pregnancy, severe psychiatric disorders, and severe cognitive impairment assessed by the Mini-Mental State Examination (score <24). 10 Groups showed similar distributions in terms of general characteristics, as well as MetS components, not presenting statistically significant differences at baseline.
Individuals recruited through media advertising in the newspapers, radio, or websites were informed about the objectives and the inclusion and exclusion criteria of the study at the screening session. After identifying the participants who were able to join the study, they were consecutively randomized into the three kinds of intervention for lifestyle change, by simple randomization 1:1:1. This procedure occurred successively in four waves till the sample size was reached.
The study was approved by the Ethical Committee of PUCRS (10/05153), registered in Brazilian Registry of Clinical Trials-ReBEC (RBR-9wz5fc), and subjects provided an informed consent.
For α = 0.05, 90% power and estimating a difference between abdominal circumference (AC) averages of 0.9 U of standard deviation, 27 volunteers in each of the 3 groups, and considering maximum loss of 20%, the estimated sample size was 34 participants per group.
Measurements
The following information was collected during candidates' screening session: anthropometric measurements, blood pressure (BP), and current medications.
AC measurement was collected through a millimeter nonextensible tape at the end of a normal expiration and at the abdomen's maximum extension. 11,12 Individuals were barefoot and lightly dressed having body weight measured through the use of a properly calibrated 160 kg Cauduro® scale. The Sunny® vertical anthropometer was used for height measurement. Body mass index (BMI) was calculated according to the following formula where weight is measured in kilograms (kg) and height in meters (m2). 13
Three consecutive BP measurements were assessed using a mercury sphygmomanometer, with participants in a seated position and after a 10-min period of rest, in accordance with the VI Brazilian Guidelines on Hypertension. 14 The mean of three measures was considered.
The biochemical tests were performed using blood samples collected via venipuncture after 12-hr fasting. Plasma glucose, total cholesterol (TC), serum triglyceride, and serum high-density lipoprotein cholesterol (HDL-C) levels were determined through enzymatic methods performed in a fully automated analyzer (VITROS 950 dry-chemistry system; Johnson & Johnson, Rochester, NY).
The week before the interventions, sociodemographic data (name, age, ethnicity, education level, marital status), health data, medications, and lifestyle behaviors were assessed. The alcohol consumption was assessed with the Alcohol Use Disorders Identification Test (AUDIT) instrument. 15 Participants who exercised at least once a week were considered physically active compared with those who did not exercise at all (sedentary).
Individuals who presented at least three criteria defined by the revised National Cholesterol Education Program Adult Panel III (NCEP ATP III; 2005) 1 were diagnosed with MetS: AC ≥102 cm for men and ≥ 88 cm for women (mandatory) 16 ; systolic blood pressure (SBP) and diastolic blood pressure (DBP) ≥130 and ≥85 mmHg, respectively, or using antihypertensive drugs; triglycerides (TG) ≥150 mg/dL or using antihypertriglyceridemia drugs; fasting glucose ≥100 mg/dL or with a diabetes diagnosis; HDL-C <40 mg/dL for men and <50 mg/dL for women or being in pharmacological treatment.
To assess the improvement of metabolic parameters, all groups were assessed at the end of interventions (3 months), using the same measurements previously described. The biochemical tests were collected individually and all on day 1. The other measurements were collected on a second appointment.
Of 125 individuals enrolled in the study, a total of 71 concluded the study, of whom 20 were from the Standard Intervention (SI) group, 25 from the Group Intervention (GI) group, and 26 from Individual Intervention (II) group (Fig. 1).
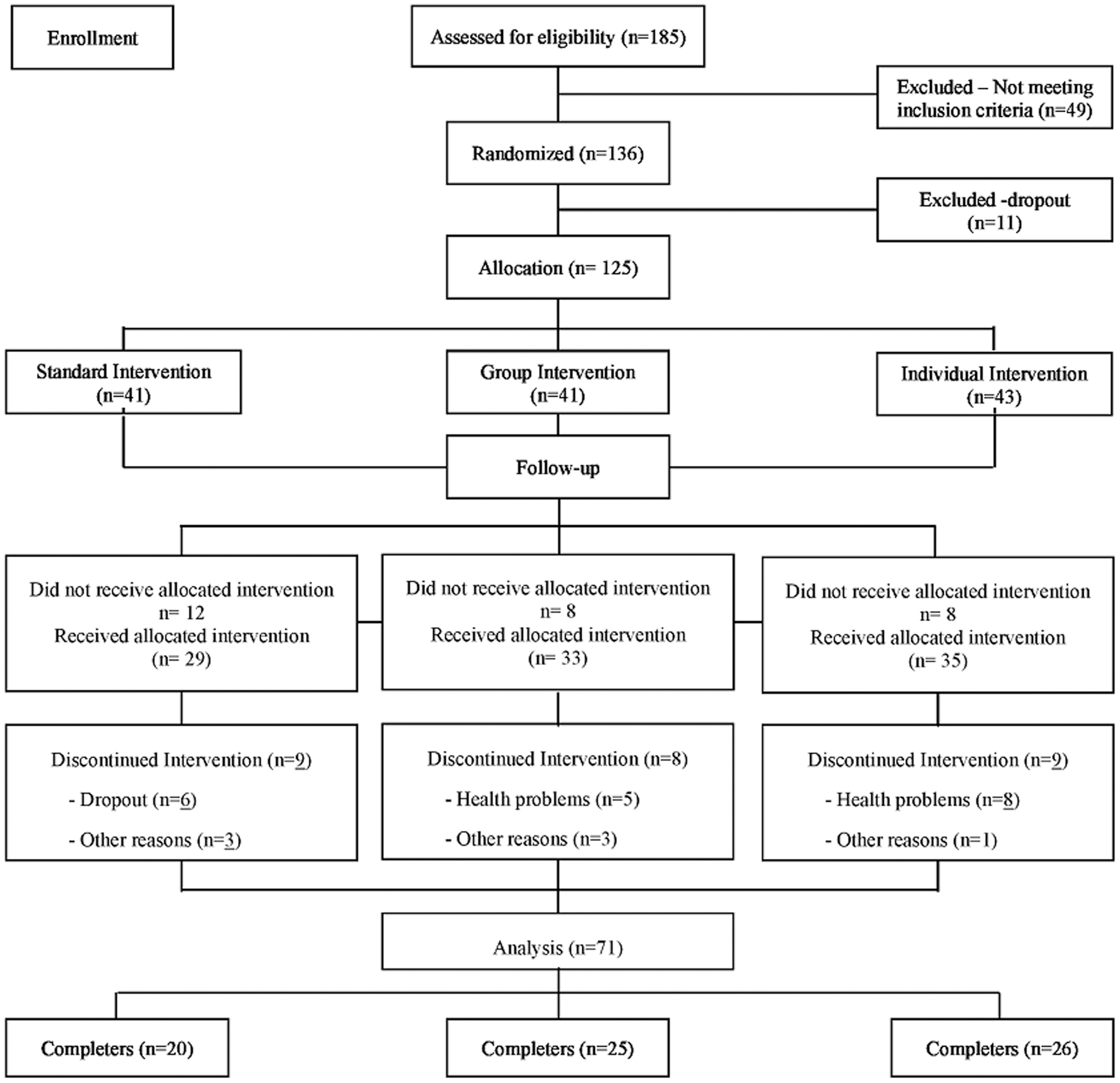
Flowchart of study participants.
Interventions
The volunteers were submitted to simple randomization and consecutively allocated in one of the following groups: SI, GI, and II.
SI group (control): nonpharmacological intervention recommended by the guidelines for clinical management of MetS. The volunteers had two individual consultations with the nursing staff. One at baseline, for standard guidance on exercising and diet, according to the healthy diet model of the Brazil's Ministry of Health, 17 and self-care focused on the administration of medications in use and general health care. After 3 months, the second consultation consisted of discussing facilities and difficulties to follow recommendations.
GI group: lifestyle change implemented weekly for 3 months (12 meetings) by a multidisciplinary team of a psychologist, a nurse, a physical therapist, and a nutritionist. The approach used for GI was discussions of themes regarding health education focused on the main cardiovascular risk factors associated with MetS, which are considered changeable, as well as motivation for changing target behaviors, based on the transtheoretical model of change, 18 during a 1 hr 45 min session. In the first 45 min, volunteers discussed a health topic proposed by the multidisciplinary team. Subsequently, they discussed and tested strategies for changing eating habits and maintaining regular exercises, which were possible to be included in the volunteers' routine, according to the group's motivation.
II group: individual appointments twice a week—one with the nutritionist and the other with the psychologist, during a 3-month period (a total of 12 appointments with each area). The nutritional intervention proposed was according to the needs of each participant, and in each weekly appointment, body weight was measured and adhesion to the diet program was assessed through a 24-hr recall. 19 Finally, during this period, three times per week, participants met with the psysiotherapist to practice exercise, consisting of walking on a treadmill. The sessions were scheduled in such a way that the participant met with the treatment group three times per week. The intensity of exercise was adjusted for each participant to achieve target heart rates ranging between 75% and 85% of maximum heart rate 20 as recommended by the I Brazilian Guidelines on diagnosis and treatment of MetS. 3 During the exercise, BP and heart rate were monitored, including signs and symptoms of cardiovascular disorders. The speed and inclination of the treadmill were continuously adjusted to maintain the target heart rate. Each one of these sessions lasted 60 min.
Statistical analyses
Statistical analyses was carried out using Statistical Package to Social Sciences—SPSS 21.0. Descriptive statistical analyses are presented as absolute and relative frequency distribution, mean, standard deviations, and symmetry investigated by the Kolmogorov–Smirnov test. Data comparisons between the groups were performed using analysis of variance (ANOVA), paired sample t test, Pearson's chi-squared, linear chi-square association, and Fisher's exact tests. The comparison between groups and time was performed by generalized estimating equations (GEE), adjusted for sex and post hoc least significant difference. P values <0.05 were considered statistically significant.
Results
Most of the individuals studied were aged between 34 and 59 years, were female (56.3%), white (90.1%), married (70.4%), sedentary (63.4%), nonsmoking (94.4%), presented high levels of education (88.7%), and of BMI (33.7 ± 3.6 kg/m2). In all the groups, participants presented measures above the recommended for AC, SBP, DBP, TG, and glucose (Table 1).
Baseline Characteristics of the Participants (N = 71)
Analysis of variance.
Pearson's chi-squared test.
Fisher's exact test.
As the main effect, BMI, AC, SBP, and DBP presented reduction, after 3 months, in both the II and GI groups (P < 0.001). After intervention, when comparing the studied groups, the BMI mean value of the II group was lower than that of the GI group (P < 0.001). In relation to the baseline, AC measures in the II group presented the lowest value compared with the SI and GI groups (P = 0.013). In the II group, there was a reduction in TG values, showing different behavior over time, in comparison with the SI and GI groups (P = 0.004). Different from other groups, HDL-C in the GI group showed an increase (P = 0.018). Fast glucose did not present statistically significant modification neither in the main effects nor in the interaction effects (Table 2 and Fig. 2). In the graphical representation, it is possible to visualize the main and interaction effects described above (Fig. 2).
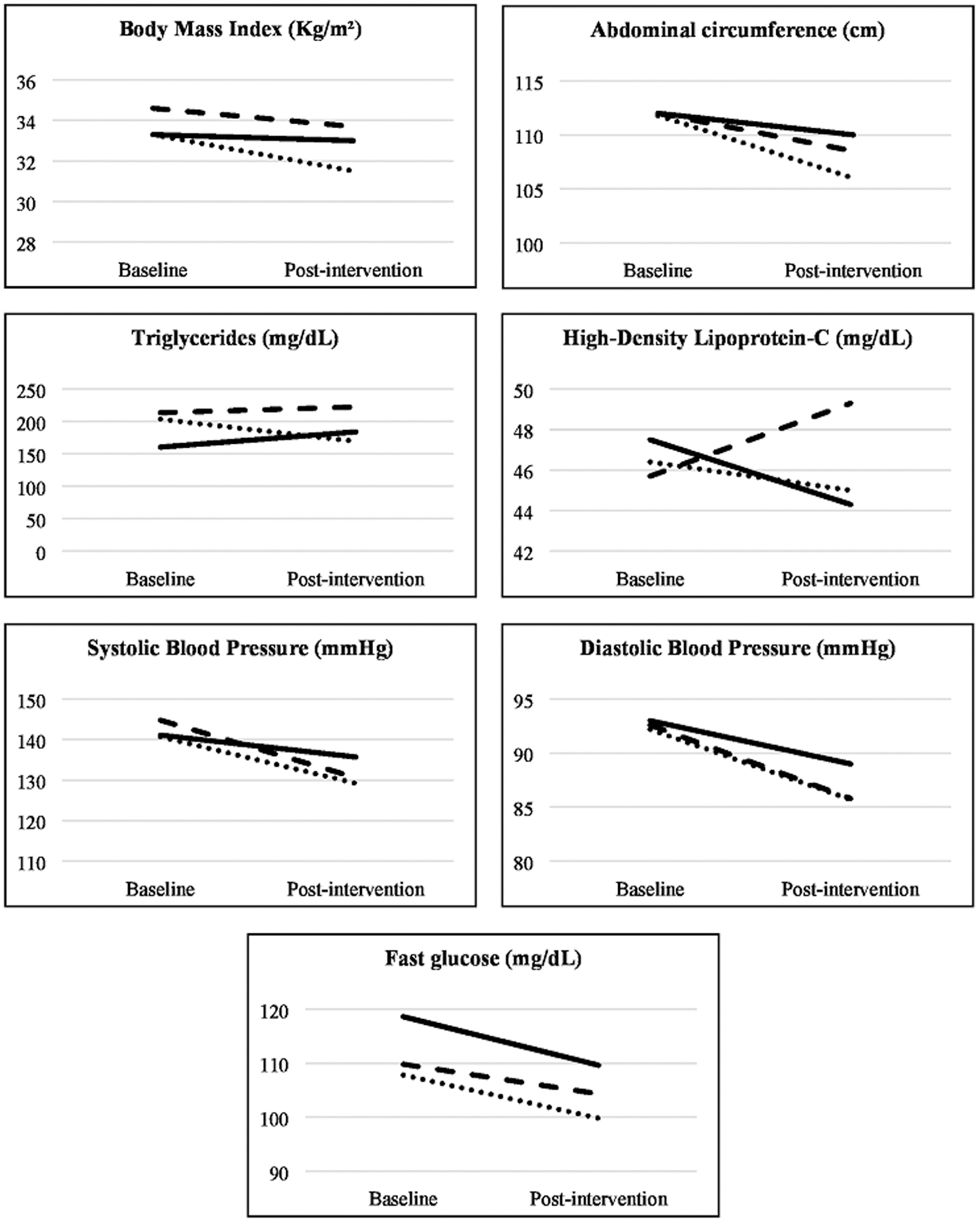
Graphical representation of behavior from the groups over time, for each metabolic parameter (N = 71).
Comparisons Between the Three Groups at Baseline and Postintervention in Metabolic Parameters (N = 71)
P values in bold show significant statistical difference.
Generalized estimating equations adjusted for sex and post hoc least significant difference (LSD).
Different lowercase letters = difference between baseline and postintervention (main effects); different capital letters = difference between the groups over time (interaction effects).
On the baseline, except for increased AC, which is a mandatory parameter, the most frequent criterion for diagnosing MetS was systemic arterial hypertension (SAH) (97.2%). The least common criterion was low HDL-C (50.7%). After intervention, increased AC (93.0%) and SAH (84.5%) remained the most frequent criteria. The least frequent criterion was increased fasting glucose (45.1%) (Fig. 3).
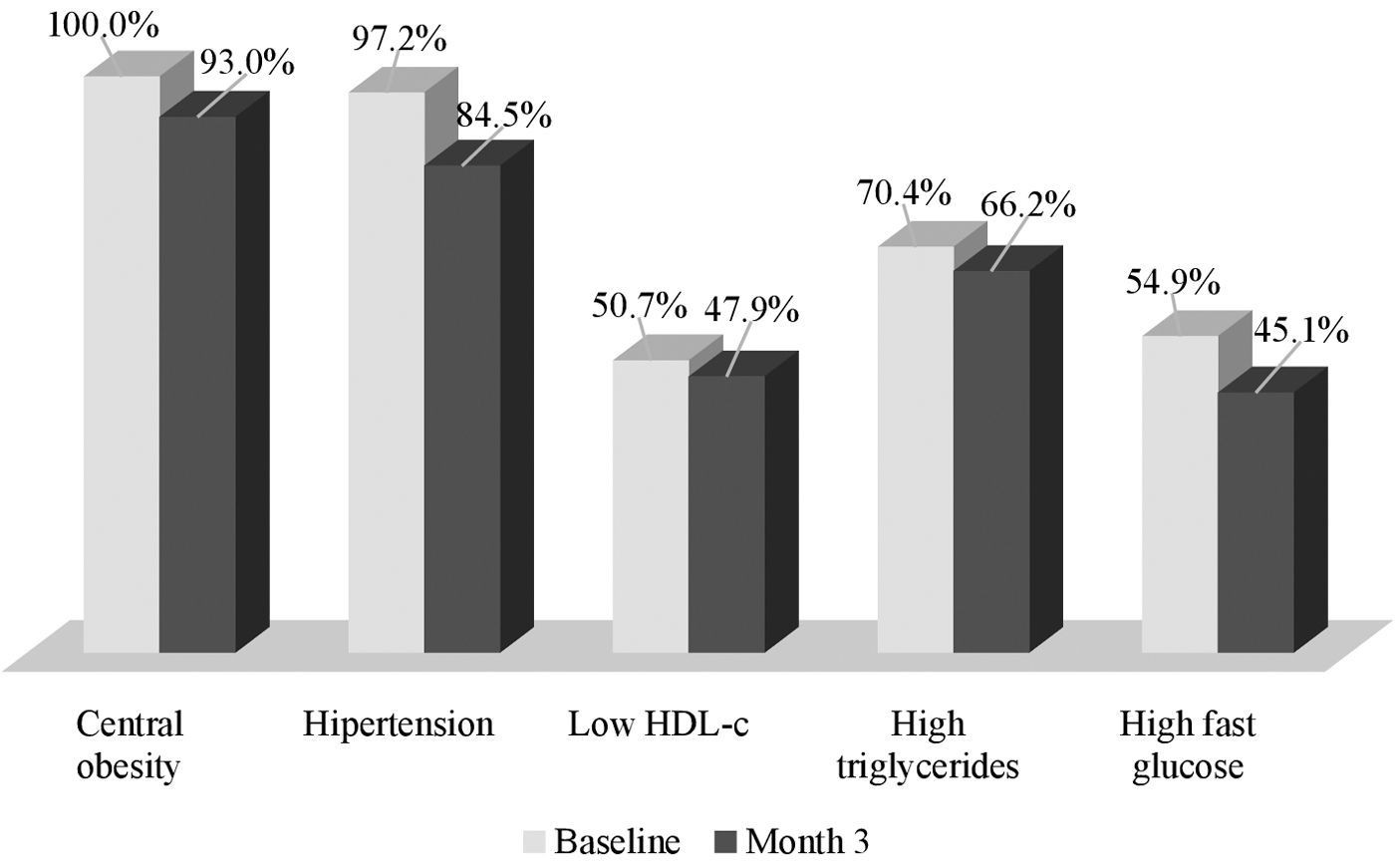
Comparison of the frequency of metabolic syndrome components at baseline and after 3 months (N = 71).
In the total sample, the number of criteria most prevalent for MetS diagnosis was three (n = 32; 45.1%), followed by four (n = 26; 36.6%). Only, 18.3% presented five criteria at baseline. After intervention, three criteria continued to be the most frequent (n = 30; 42.3%); 15.5% and 1.4% of the sample showed two and one criteria, respectively. The mean of the number of criteria decreased significantly (paired sample t test: P = 0.002).
The percentage of individuals in each diagnostic criteria for MetS changed significantly (linear chi-square association: P < 0.001). At the end of the interventions, 16.9% of the individuals did not meet the number of criteria required for the clinical condition (Fig. 4).

Frequency of the number of criteria of metabolic syndrome diagnosis in total sample (N = 71).
There were no differences between the groups at baseline and between the groups over time regarding the number of criteria (GEE: P = 0.849 and P = 0.420, respectively). In relation to time, the GI and II groups presented statistically significant overall change after 3 months (GEE: P = 0.002). Within the GI group, 16.0% of the individuals presented less than three criteria and in the II group, 15.4% after intervention (Fig. 5).
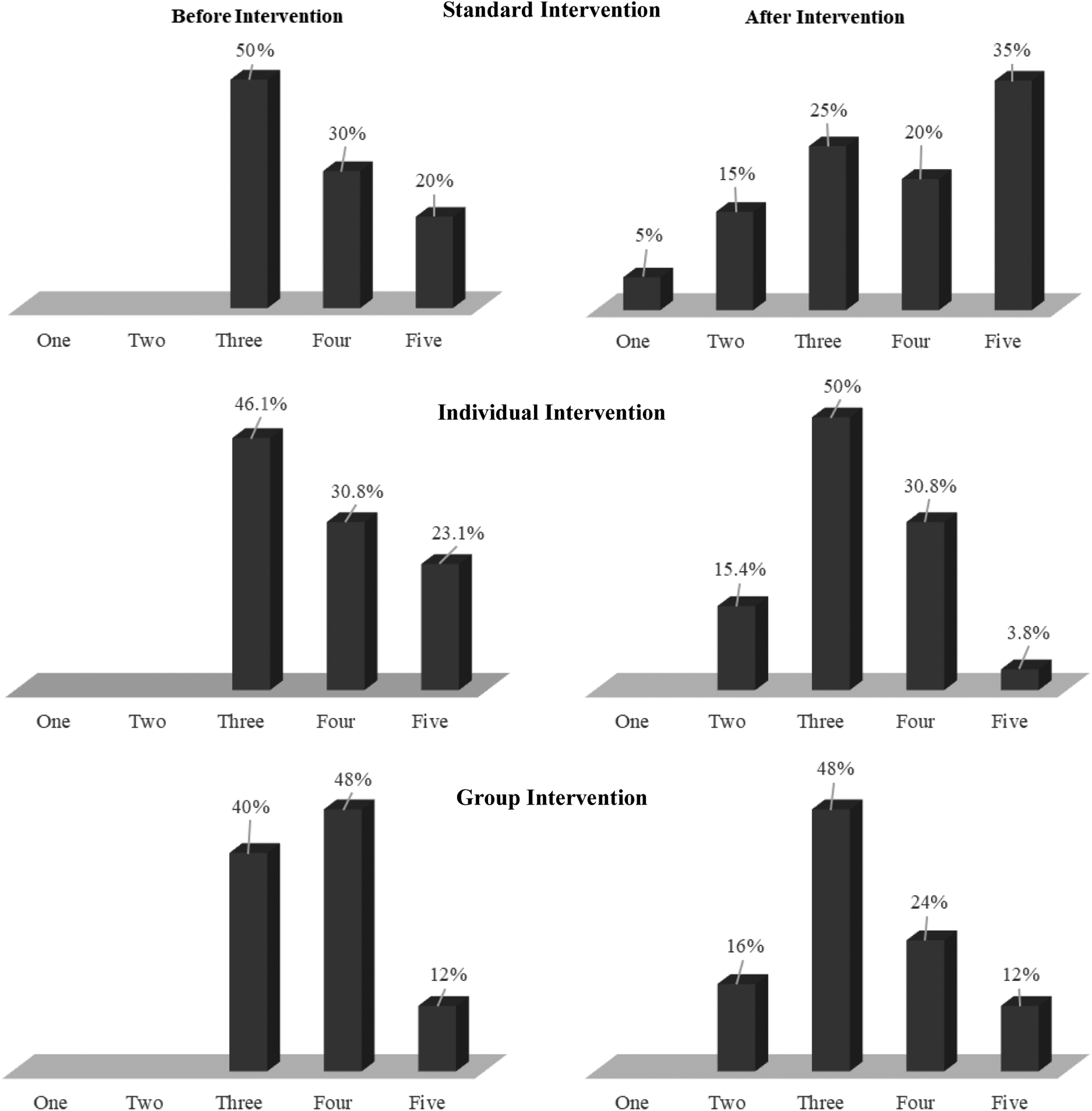
Number of criteria of metabolic syndrome diagnosis in the different intervention groups (N = 71).
Discussion
This study tested three types of intervention for changing lifestyle in individuals with MetS, followed during 3 months, to determine their effects on the number of diagnostic criteria and clinical parameters of MetS.
Results suggest that GI and II were associated with significant BMI, AC, SBP, and DBP reduction, in accordance with Kataria et al., 21 who pointed out that regular physical activity, along with improved diet, has the ability to attenuate the syndrome and bring benefits to its combat, if performed methodically. They also emphasized the importance of personalizing treatment strategies and early interventions. Additionally, Gleeson et al., 6 corroborating our findings, demonstrated that lifestyle intervention (diet and physical activity) may lower BMI and disease risk and/or have therapeutic value in treating disease.
In general, diet and physical activity behavioral interventions with changes in BMI and AC result in short-term consistent benefits across important health outcomes, such as BP, HDL-C, and TC levels and into long-term reduction in coronary artery disease (CVD)-related events. 22,23
The average of AC reduction in the II group was similar to the one found in individuals who had underwent an intensive lifestyle intervention program. 24 Furthermore, II and GI demonstrated to be effective once they promoted a reduction of 6.1 and 3.5 cm, respectively. Considering the fact that reducing AC by ≥3 cm is already a significant improvement to reduce cardiometabolic risk factors, 25 these results present a high clinical relevance. In an intensive behavioral management intervention program, greater relative decrease in AC was associated with greater improvements in MetS components. 26
With regard to BP, previous data have shown that regular aerobic exercise can reduce BP by 06–10 mmHg, in previously sedentary both men and women. 27 Regular exercise can also help to control BP, in cases of risk of hypertension, and reduce the mortality rate of physically fit hypertensive individuals, when compared with their normotensive counterparts. 28
Other studies showed that the maintenance of good physical fitness acts favorably on the cardiovascular risk factors that comprise the diagnostic criteria of MetS because it improves insulin sensitivity and thus reduces the risk of developing type II diabetes mellitus and CVD. 29 –31
As the main effects related to the mean HDL-C, TG, and glucose levels, there were no differences found from baseline to postintervention evaluations. In the past years, the classical epidemiology stated that low levels of HDL-C are a part of the atherogenic dyslipidemia complex, which has triggered an intense interest in increasing HDL-C levels for the therapeutic intervention of CVD. 32,33 However, recent studies of genetic epidemiology are not supporting this causal relationship. Evidence suggests that the association between HDL-C levels and CVD may be indirect or more complicated than previously recognized. 34 A current study in the field of human genetic demonstrates that genetically altered HDL-C levels do not necessarily translate to an altered risk of CVD. 32 As in our research, a systematic review of the impact of lifestyle modification programs on metabolic risks in adults with MetS did not reveal a significant effect on HDL-C and fasting blood glucose. 35
Although studies suggest that lifestyle intervention is beneficial for glycemic control, this does not seem to occur in patients with impaired glucose tolerance and it depends on the type of lifestyle intervention. 36
In a study with syndromic adults, it was observed that on the first 15 days, AC, SBP, DBP, and serum glucose were not modified. Interestingly, after 2 months of intervention, AC, BMI, SBP, and DBP decreased, and there was no change in TG and glucose levels, as in our study, suggesting that the intervention time can modify the results. 37 Although our study did not find significance for this marker, efforts to reduce TG are important because strong evidence suggests that elevated triglyceride-rich lipoproteins represent causal risk factors for low-grade inflammation, atherosclerotic cardiovascular disease, and all-cause mortality. 38
When evaluated over time, HDL-C showed, as interaction effect, a different behavior among the groups. While there was a decreasing tendency in the SI and II groups, the HDL-C levels increased significantly in the GI group. However, over the time, as interaction effect, there was an increasing tendency in TG levels in the SI and GI groups, as oppose to a significant decrease in the II group. A prospective, randomized, parallel-group assessor-blind study with 543 individuals with diagnosed MetS, in accordance with the American Heart Association/National Heart, Lung, and Blood Institute criteria, conduct a lifestyle intervention. After 6-month exercise-focused intervention using telemonitoring systems, all components of MetS showed a significant between-group difference with the exception of HDL-C, favoring the exercise group. 39
Regarding changes in the frequency of the number of criteria for MetS, ∼16.9% of subjects did not present a MetS diagnosis at the end of the intervention, which indicates that lifestyle modification contributes to the reduction of the cardiovascular risk. In the II group, the percentage of individuals with five criteria reduced 83.5%; in the GI group, the number of individuals with five criteria remained the same and the number with four criteria had a reduction of 50.0%. It is important to consider that unhealthy diet, physical inactivity, and genetic predisposition are among the main factors contributing to the emergence of MetS, 40,41 and these first two factors can be modified through interventions such as that proposed by this study.
Results reinforce that both the lifestyle modification program that combines weekly nutritional counseling with regular exercise and the program that implemented lifestyle change weekly by a multidisciplinary team produced beneficial effects on metabolic parameters, especially on BMI, AC, SBP, and DBP, and decreased the number of diagnostic criteria for MetS by reducing cardiometabolic risk.
As reported by previous studies, 20,24,42 these findings indicate that lifestyle modification can produce beneficial effects on the management of MetS, even in a relatively short period.
Even though other studies presented similar dropout rate, we believe that this was a limiting factor of our study. 43,44 Still, it is important to highlight that the dropout rate was similar between the GI and II groups.
The study proposal contemplated eating habits and physical activity, which are two main arguments in the first-choice therapy for the improvement of modifiable risk factors for cardiovascular disease. Therefore, intervention programs promoting changes in lifestyle should be encouraged.
In conclusion, the interventions proposed by this study reinforced that nonpharmacological strategies for changing lifestyle affect the reduction of cardiovascular risk factors involved in MetS. All interventions produced beneficial effect on reduction of cardiovascular risk factors of MetS. They were also able to remove the population from this clinical condition by decreasing the diagnostic criteria. Thus, the results suggest that, in the clinical practice, both II and GI, especially when conducted by a multidisciplinary team, may be successful alternatives to the treatment of MetS.
Footnotes
Acknowledgment
The authors thank the colleagues of the MERC research group for their collaboration.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was financially supported by a grant from the Brazilian National Council of Scientific and Technological Development (CNPq), number 481279/2009. Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES).