
Abstract
Background:
Obesity is a chronic disease with several co-morbidities that increase morbidity and mortality and decrease quality of life. Psychopathologies are an important group of co-morbidities. In this study, it was aimed to search for the presence of depression and sexual dysfunction in patients with obesity, examine impact of obesity on marital adjustment, and highlight those important problems that are usually overlooked.
Methods:
Fifty patients who were seen in the obesity outpatient clinic in a random month as case group and gender-matched 50 healthy individuals as control group were included in the study. The inclusion criteria were body mass index (BMI) ≥30 kg/m2 and having a sexual partner. The exclusion criteria were having psychiatric/mental or any other chronic illness, using medication that would affect sexual functions, and alcohol/substance abuse. After recording the sociodemographic data, patients were asked to take three internationally validated questionnaires: The Arizona Sexual Experience Scale (ASEX), Dyadic Adjustment Scale (DAS), and Beck Depression Inventory (BDI). Results were analyzed using SPSS.
Results:
Fifty patients with obesity as case group and 50 normal weight healthy persons as control group were included in the study. BMI and BDI score were significantly higher in the case group than in the control group. DAS score was lower in the case group for consensus and affectional expression than the control group but there was no difference for satisfaction, cohesion, or total score between the groups. ASEX score was higher in the case group than in the control group.
Conclusion:
Patients with obesity have dyadic consensus problems with their partners. Their excessive weight causes distress and difficulty in expressing their feelings and usually results in marital problems and depression. Evaluation of the patient with a multidisciplinary approach in obesity centers will allow patients to be analyzed in every aspect of obesity including these issues and contribute to the success of the treatment.
Introduction
Obesity is defined as abnormal or excessive fat accumulation that presents a risk to health by the World Health Organization (WHO). The ratio of fat mass to lean body mass is increased to cause weight to exceed the limits determined according to the height. 1
Obesity is classified using body mass index (BMI). It is now accepted as a disease beyond being a cosmetic problem. Thus, obesity-related pathologies are a matter of concern. 2 Although physical co-morbidities of obesity are well established, its association with psychopathologies is less explored and needs to be addressed better. 3
Anxiety, depression, and sexual dysfunction usually accompany obesity and decrease quality of life seriously. 4,5 Sexual health is an important part of human life in both men and women, but expression of sexual problems or diagnosis of these pathologies is not as easy as physical pathologies. Dyadic consensus, dyadic satisfaction, dyadic cohesion, and affectional expression are terms to describe the quality of marriage. Despite present researches about obesity and sexual dysfunction, obesity and marital quality are still unexplored.
In this study, it was aimed to search for the presence of depression and sexual dysfunction in patients with obesity, examine impact of obesity on marital adjustment, and highlight those important problems that are usually overlooked.
Materials and Methods
Fifty patients who were seen in the obesity outpatient clinic in a random month as case group and gender-matched 50 healthy individuals as control group were included in the study.
The inclusion criteria were BMI ≥30 kg/m2, having a sexual partner, and positive informed consent.
The exclusion criteria were BMI ≤30 kg/m2, having psychiatric/mental or any other chronic illness, using medication that would affect sexual functions, and alcohol/substance abuse.
After recording the sociodemographic data, the patients were asked to take three internationally validated questionnaires that were The Arizona Sexual Experience Scale (ASEX), Dyadic Adjustment Scale (DAS), and Beck Depression Inventory (BDI).
The ASEX: this is a five-item self-rating scale that quantifies sex drive, arousal, vaginal lubrication/penile erection, ability to reach orgasm, and satisfaction from orgasm. Each question is scored between 1 and 6 and total score would be 5–30. This test has national validity and reliability approval in our country. According to this test, the patient has sexual dysfunction if a total score of ≥19 or any one item with a score of ≥5 or any three items with a score of ≥4 is found. 6
DAS: the test is developed by Spanier. The scale's Turkish validity and reliability study was conducted by Fışıloğlu and Demir. 7 The test evaluates marital quality testing dyadic satisfaction, dyadic consensus, dyadic cohesion, and dyadic affectional expression. 8 Total score is the sum of all scores gained from answers from each part of the questionnaire and it is between 0 and 151. Higher scores indicate better marital quality.
BDI: BDI is an objective self-rated scale that evaluates the level of somatic, emotional, motivational, and cognitive symptoms seen in depression. 9 It contains 21 items on a 4-point scale from 0 (symptom absent) to 3 (severe symptoms). The total score is achieved by adding the highest ratings for all items and it is between 0 and 63. Higher scores indicate greater symptom severity. The national adaptation of the test is made by Hisli. 10
Statistical method: statistical analysis was performed using SPSS 22.0 for Windows program. Descriptive statistics were reported as mean, standard deviation, median, minimum, maximum, frequency, and percentage values. Distribution of variables was tested with Kolmogorov Simirnov test. Quantitative independent data analysis was made with Mann–Whitney U test. Qualitative independent data analysis was made with chi-square test. The statistical significance level was regarded as P < 0.05.
This study was approved by the Ethics Committee of Istanbul Training and Research Hospital (1879/2019). All participants provided written informed consent. All procedures performed in the study were in accordance with the 1964 Helsinki Declaration.
Results
The mean age was 42.6 ± 9.7 years for the case group and 33.9 ± 9.1 years for the control group. Mean age was higher in the case group than in the control group (P < 0.05), but there was no significant difference for gender, marital status, or number of children between case and control groups (P > 0.05). Level of education was lower in the case group than in the control group (P < 0.05). Employment rate was higher in the case group than in the control group (P < 0.05). The duration of marriage was longer in the case group than in the control group (P < 0.05) (Table 1).
Results of Case and Control Group
Mann–Whitney U test.
t test.
Chi-square test.
SD, standard deviation.
The significant values are written in bold italics.
BDI score was higher in the case group than in the control group (P < 0.05). DAS score was lower in the case group for consensus and affectional expression than in the control group (P < 0.05), but there was no difference for satisfaction, cohesion, or total score (P > 0.05) between the groups. ASEX score was higher in the case group than in the control group (P < 0.05) (Table 1, Figs. 1 and 2).

DAS score results of case and control groups. DAS, Dyadic Adjustment Scale.
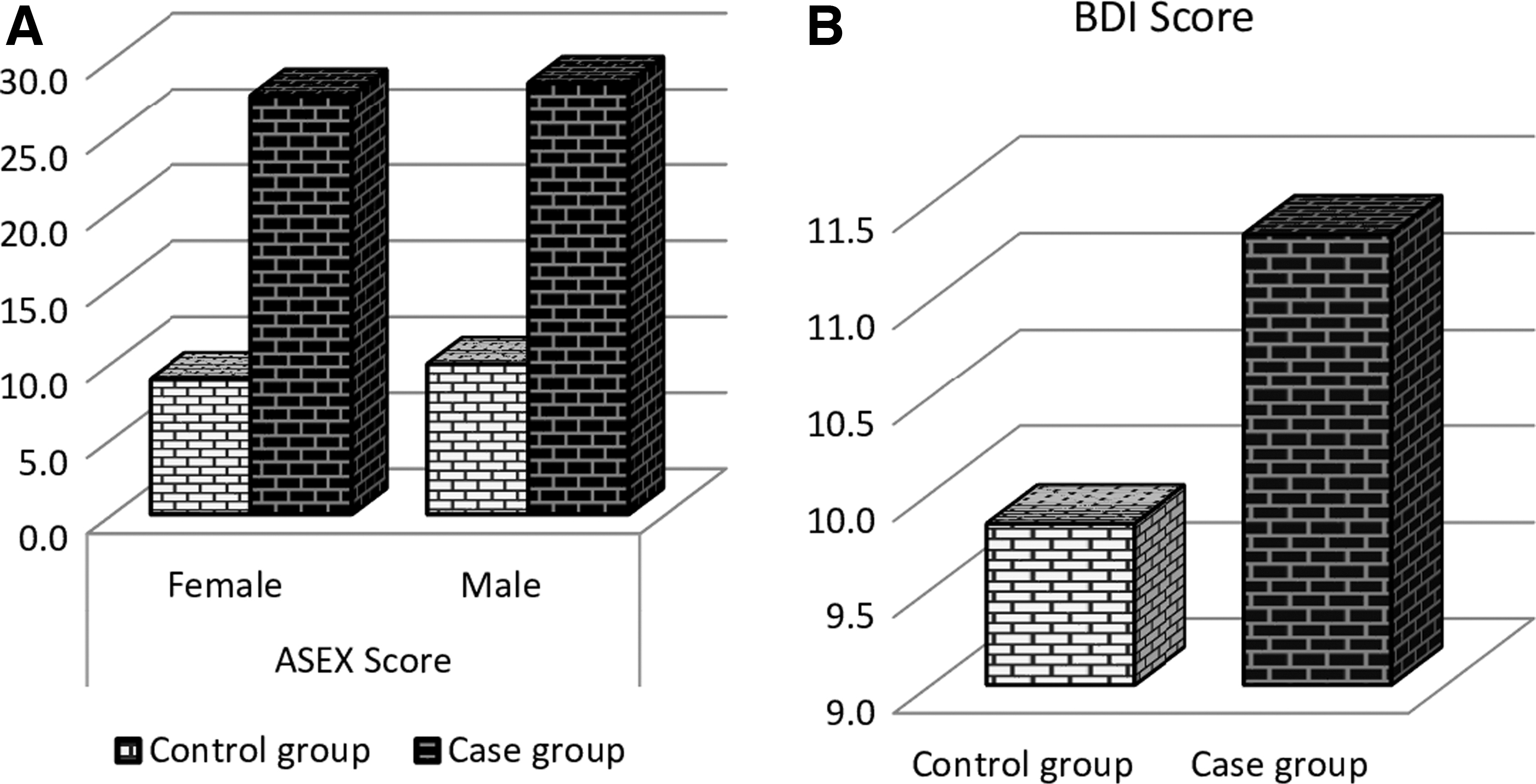
ASEX score and BDI results of case and control groups. ASEX, Arizona Sexual Experience Scale; BDI, Beck Depression Inventory.
Discussion
Obesity is a globally increasing chronic disease that has negative impact not only on physical health of the individual but also on psychological health and quality of life. 11 Despite the social pressure put on people to lose weight and the increased availability of weight loss tools, it has reached to epidemic proportions at both national and international levels. 12
There are many diseases and complications related to obesity, but the physical complications are the target of attention most of the time, and psychological effects on life of the individual with obesity and his/her family are either ignored or remain in the background. 13
WHO accepts obesity as a “social and environmental disease.” 14 Stigmatization and discrimination toward people with obesity often result in depression, low self-esteem, and sexual and marital problems. 15,16
There are several studies showing a strong link between obesity and depression and it is known that people with obesity experience depression and anxiety much more than people with normal weight. Loneliness and stigmatization nourish this situation. 17,18 The fat mass is a causal risk factor for depression 19 in both women and men with obesity, but the nonphysical consequences of obesity in the men could sometimes be ignored. 20 The results of our study support that persons with obesity have the idea that they have impaired performance in life that results in high rates of depression.
Sexual health is an important determinant of quality of life and body weight/image is one of the main components affecting sexual life. 21 Kaneshiro et al. showed that increasing obesity levels negatively affected sexual life in women in their study with 6690 women with obesity living in United States. 22 Our study also showed that obesity caused sexual problems between partners when compared with people with normal weight. Kolotkin et al. conducted a series of studies to find that obesity was a risk factor for the degree of dysfunction in sexual life. However, in obesity, sexual dysfunction could also be related to other psychiatric problems, including low self-esteem and low self-body image instead of being only directly related to obesity. 23 High rates of depression concomitantly with sexual dysfunction found in our study in persons with obesity support this idea. In the literature, it is emphasized that sexual dysfunction in women is more related to low self-body image than BMI. Studies defend that women with obesity avoid sexual intercourse because they think their body is not attractive for their partners. Thus, the source of the problem is “avoiding” sexuality rather than sexual dysfunction. 24
Sexual activity is decreased in men with obesity. Erectile dysfunction and other sexual abnormalities such as decreased sexual desire or sexual intercourse satisfaction seen in men with obesity benefit from weight loss. 25,26 Body weight seems to be the most important part of body image and it is important to analyze the impact of obesity on sexual functions in both men and women while evaluating a patient with obesity.
Obesity affects relationship quality with partners and causes marital problems. 27 Although we did not find a significant difference in total DAS score in case and control groups, subgroup DAS score for consensus and affectional expression was lower in the case group than in the control group, predicting that people with obesity could not express their feelings well and had difficulty to agree on subjects with their partners. There are several studies about sexual dysfunction in obesity, but the data are limited about dyadic consensus. 28 –30 Thus, this study is one of the few studies highlighting the importance of the subject. Increasing BMI causes not only sexual problems but also increases depression rates in married couples, 31 and marriage quality is improved in different aspects with weight loss. 32 As obesity causes marital problems, marital problems can increase the risk for obesity and create an unavoidable circle. 33
In contrast, dyadic consensus benefits weight loss. It was found that in women with type 2 diabetes, dyadic consensus scores at the beginning of treatment predicted changes in BMI over time, with better problem solving and higher relationship satisfaction at baseline related to steeper decreases in BMI across treatment. 34 Along with obesity, dyadic consensus scores are decreased in many other situations such as urinary incontinence, 35 receiving infertility treatment, 36 cancer, especially breast cancer, 37,38 depression and other psychiatric disorders, 39,40 and many other life-limiting illnesses. 41 A dyadic reintegration model is suggested to support dyads facing life-limiting illness. This model includes three adaptation processes of comprehension, creative adaptation, and reintegration for couples to achieve a better communication and relationship. 41
Conclusion
Obesity is one of the major causes of depression, sexual function impairment, and diminished marital quality. Thus, health care providers should include questions about these subjects using motivational interview techniques and prevent those problems to remain overlooked. Psychosocial support should be a part of obesity treatment. The partner of the patient should be included in the treatment and counseling of couples should be applied when necessary. Treatment of obesity does not only intend improvement in physical health but also psychological health and quality of life. Obesity centers with multidisciplinary approach seem to provide the best solution to all aspects of health care to patients with obesity.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.