
Abstract
Background:
Several studies showed that lipid accumulation in the pancreas (NAFPD: nonalcoholic fatty pancreas disease) may lead to different pancreatic disorders, including beta-cell dysfunction. The role of genetic and environmental factors in pancreatic lipid accumulation is unclear. We evaluated the magnitude of genetic and environmental impact on pancreatic lipid content within a cohort of adult twin pairs.
Patients and Methods:
We investigated 136 twin subjects [monozygotic (MZ, n = 86) and dizygotic (DZ, n = 50) same-gender twins (age 57.7 ± 9.1 years; body mass index [BMI] 28.0 ± 4.4 kg/m2; females 64.7%)] with a 256-slice computed tomography (CT)-scanner. Using nonenhanced CT images, we calculated the average value of pancreatic attenuation expressed in Hounsfield unit (HU) suggesting pancreatic lipid content. Crude data were adjusted to age, sex, BMI, and hemoglobinA1c values. Intrapair correlations were established, and structural equation models were used for quantifying the contribution of additive genetic (A), common environmental (C), and unique environmental (E) components to the investigated phenotype.
Results:
The study cohort represented a moderately overweight, middle-aged Caucasian population. Average pancreatic attenuation was 48.9 ± 11.9 HU in MZ and 49.0 ± 13.0 HU in DZ twins (P = 0.934). The intrapair correlation between HU values was stronger in MZ compared to DZ twins (rMZ = 0.536, P < 0.001; rDZ = 0.115, P = 0.580). Using the structural equation model, a greater unique environmental influence [E: 54%, 95% confidence interval (CI) 19%–66%] and a moderate additive genetic dependence (A: 46%, 95% CI 34%–81%) were found.
Conclusions:
The results of our classical twin study indicate that environmental (lifestyle) influences slightly outweigh genetic effects on the phenotypic appearance of pancreatic lipid accumulation known as NAFPD.
Introduction
Although the first human autopsy investigation about the association between pancreatic fat and obesity was published as early as 1933, the clinical consequences of lipid accumulation in the pancreas remained unrevealed for a long period of time. 1 Nevertheless, fat deposition in the pancreas (fatty pancreas), termed nonalcoholic fatty pancreas disease (NAFPD), has gained much attention in the last years. 2 –9 It was due, at least in part, to the development of imaging techniques enabling to perform clinical investigations to characterize the clinical significance of pancreatic lipid accumulation. There is a consensus that NAFPD is associated with increasing age, body mass index (BMI), and other factors of the metabolic syndrome. 3,9 –12 Furthermore, lipid accumulation in pancreas may promote the development of chronic pancreatitis and exacerbate the clinical picture of acute pancreatitis. 13 –15 It was also suggested that pancreatic steatosis promotes dissemination and worsens prognosis of pancreatic cancer. 16
The potential relationship of pancreatic lipid accumulation with β cell dysfunction is debated. 17 A study with Korean subjects documented with computed tomography (CT) that pancreatic volume and fat deposition might be associated with the development and progression of Type 2 diabetes. 18 Namely, the authors investigated four groups of patients from normal glucose tolerance to overt Type 2 diabetes with different duration and found that decreasing pancreatic volume and increasing lipid accumulation were associated with increasing duration of diabetes. 18 Another clinical investigation documented that pancreatic fat is negatively correlated with insulin secretion in subjects with prediabetes. 19 Nevertheless, others found in a cross-sectional clamp study that pancreatic fat content increased in individuals with prediabetes (compared to subjects with normal glucose tolerance) but without a direct relation with beta-cell function. 20 Notably, NAFPD can frequently be observed; the prevalence rate may vary between 16% and 35% depending on the method used and population investigated. 10,21,22
The reliable measurement of pancreatic fat accumulation is challenging in the clinical practice. Abdominal ultrasonography, CT, and magnetic resonance imaging techniques were used in different clinical studies; however, these measurement methodologies differ in availability, cost, radiation dose, and reproducibility, which should be considered both in research and clinical settings. 23 A recent clinical study documented that CT attenuation indices can be used to quantify pancreatic fat volume; the results were validated by histological measurements. 24
Lipid accumulation in different organs may be triggered by genetic and environmental factors. In general, anthropometric parameters such as weight, height, and, consequently, BMI have relatively strong genetic dependence. 25 Importantly, heritability of different adipose tissue compartments and that of ectopic fats may vary. 26 Classical twin studies allow determining the effect of genetics and environmental factors on a certain phenotype. Comparing data of monozygotic (MZ) versus dizygotic (DZ) same-gender subjects, the contribution of genetics and environment to the investigated phenotype (in this case: CT density representing pancreatic lipid content) may be quantified. We could identify in the literature only a small study with eight healthy MZ twin pairs where effects of physical activity on hepatic and pancreatic fat contents were investigated. 27
The role of genetic and environmental factors in the development of NAFPD is unclear. Therefore, the aim of our study was to evaluate the magnitude of genetic and environmental impact on pancreatic lipid content within a cohort of healthy adult twin pairs using standardized measurements of nonenhanced CT imaging.
Subjects and Methods
Study population
This study was a prospective, single-center classical twin study involving MZ and DZ same-gender twin subjects of self-reported Caucasian ethnicity. The investigation was conducted under the name of BUDAPEST-GLOBAL (Burden of atherosclerotic plaques study in twins—Genetic Loci and the Burden of Atherosclerotic Lesions) clinical study; the participants had been co-enrolled with the large, international, multicenter GLOBAL clinical study (
In the current study we included 68 twin pairs (136 twin subjects; 86 women, 50 men); 33 twin pairs from the original cohort were excluded due to inadequate image quality as imaging was tailored for cardiac CT acquisition. We assessed zygosity using a multiple self-reported questionnaire 31 and, accordingly, our study population consisted of 43 MZ and 25 DZ same-gender twin pairs. For evaluating genetic and environmental influences on pancreas lipid accumulation, we investigated CT attenuation of the pancreas to quantitate pancreatic lipid accumulation. This method was earlier validated by histologic assessment and has been accepted for assessing NAFPD in clinical settings. 18,24
CT scanning protocol
For the original study a noncontrast enhanced CT scan of the heart was performed with a larger coverage to visualize the upper part of the abdomen. 29 Importantly, the native CT image acquisition resulted in a small (<1 mSv) radiation dose.
Measurements of pancreatic CT attenuation were performed in a blinded manner, that is, researchers who performed CT measurements were blinded to zygosity of twin subjects. Pancreatic CT attenuation was assessed in three regions of interests (ROIs), which were placed in the head, body, and tail and were at least 1.5 cm2. Special attention was taken not to include the peripheral margin of the pancreas or any vasculature structures. For further analysis we used the mean values of CT attenuation measured in three ROIs of the pancreas (Fig. 1). Pancreatic attenuation was measured by two radiologists (Á.L.J., A.P., both with 5 years of experience with CT) in consensus. CT attenuation was expressed in Hounsfield unit (HU).
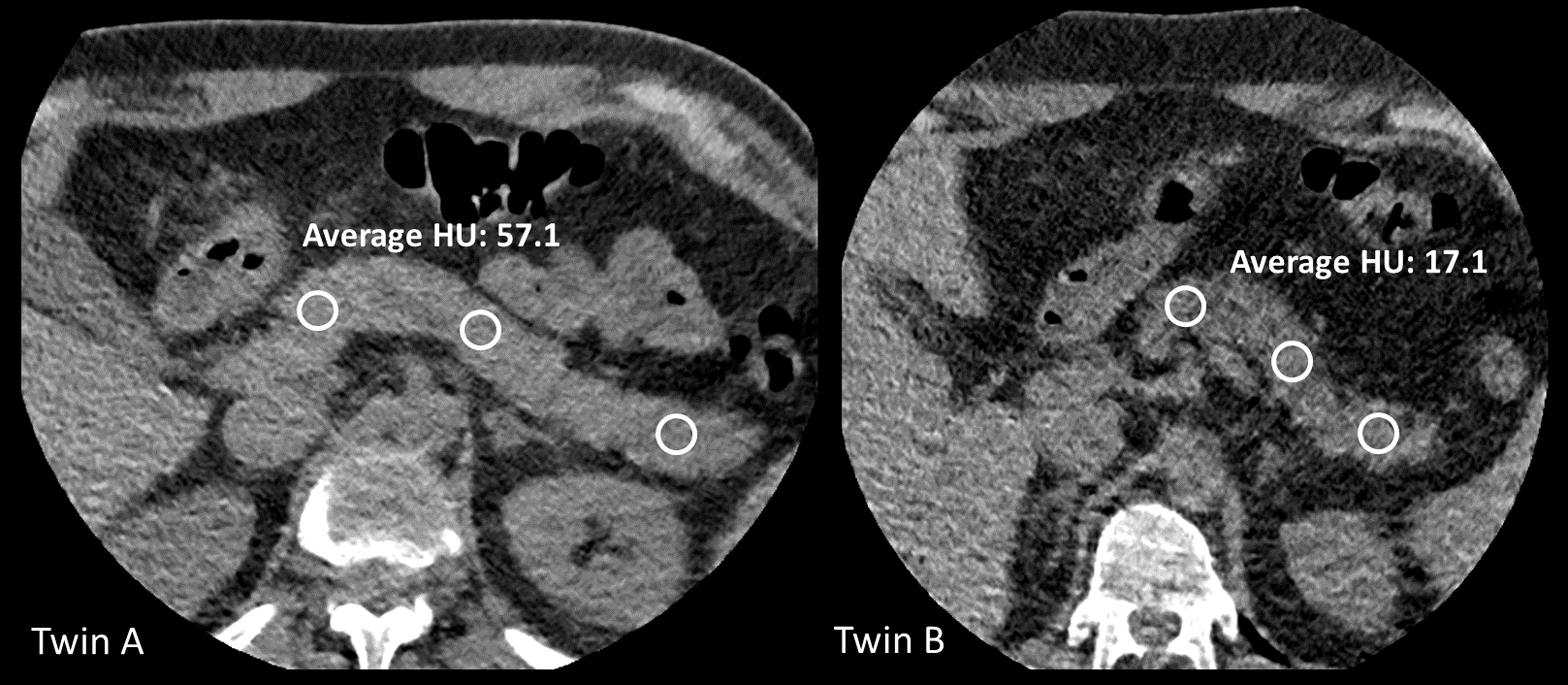
Evaluation of pancreatic attenuation in a dizygotic twin pair. Measurements were performed in the head, body, and tail of the pancreas with at least 150 mm2 sized regions of interests (white circles), and average values of the three measurements were used for analysis. HU, Hounsfield unit.
Anthropometric data, medical history, and laboratory analysis
We recorded basic anthropometric parameters (weight, height, waist circumference). Brachial blood pressure was measured before the CT examination. Questionnaires regarding past medical history and current lifestyle, smoking, and dietary habits were recorded for every participant. Fasting peripheral blood draw was performed before the CT examination.
Laboratory parameters were investigated using standard methods in certified laboratory.
Statistical analysis
Continuous variables are expressed as mean ± standard deviation, whereas categorical variables are expressed as numbers and percentages. MZ and DZ twins were compared using Student's t-tests (continuous variables) or chi-squared tests (categorical variables). Correlations were calculated using Pearson correlation coefficients. Descriptive statistics, correlations, and reproducibility measurements were calculated using IBM SPSS Statistics version 23 (IBM, Armonk, NY). The level of significance was set at P < 0.05.
For evaluating genetic and environmental influences on NAFPD, first we assessed co-twin correlations of HU in MZ and DZ pairs separately, and then we evaluated the heritability using structural equation models often called ACE models. In the ACE model, the best fit model substantiates the quantification of genetic or environmental effects on phenotype investigated (in our study: pancreas lipid accumulation assessed by CT attenuation, expressed in HU). All models were corrected for age, sex, BMI, and hemoglobinA1c (HbA1c) values. Log likelihood-based 95% confidence intervals (CIs) were calculated for all estimated parameters. All calculations were performed using R version 3.6.0. 32 Twin modeling was performed using OpenMx version 2.12.2. 33 Using the structural equation model, the effect of genetic and environmental influences on a given phenotype can be partitioned into additive genetic effects (A), common (or shared) environmental (C), and unshared (or unique) environmental (E) factors, which drive the variance in the phenotype for each twin. Additive genetic effect (A) is perfectly (r = 1.0) correlated across MZ twins and less (r = 0.5) correlated across DZ twins. Environmental components are grouped as common factors (C), which equally affect the siblings, and unique factors (E), which cause differences within families. Both MZ and DZ twins shared 100% of their C factors and none of their E factors. Since measurement error in the phenotype is also uncorrelated across measurements, it appears as part of the unique environmental component.
Results
Our study cohort (68 twin pairs, 136 twin subjects) represented a middle-aged, moderately overweight Caucasian population with a slight female predominance (age: 57.7 ± 9.1 years, 64.7% females, BMI: 28.0 ± 4.4 kg/m2, waist circumference 97.3 ± 11.5 cm). Overweight (BMI 25.0–29.9 kg/m2) and obesity (BMI ≥30.0 kg/m2) were more frequently observed among males (44.4% and 37.5%) than in females (36.9% and 26.9%), respectively (P = 0.024). However, males and females did not differ significantly regarding prevalence of increased waist circumference (males: >94 cm, 86.9%; females >80 cm, 76.4%, P = 0.056). In the total cohort, mean values of laboratory parameters indicating glucose and lipid metabolism, as well as those of renal and hepatic function, were in normal or near-normal ranges; homeostasis model assessment of insulin resistance value (2.17 ± 3.22) was slightly elevated (Table 1).
Demographic Characteristics, Medical History, and Clinical Laboratory Data of Twin Subjects
Continuous variables are presented as mean ± SD, while categorical as n (%). MZ and DZ twins were compared using Student's t-tests and chi-squared tests, as appropriate. P values represent two-sided P values for independent t-tests (continuous variables) or chi-squared tests (categorical variables) done between the MZ and DZ twin groups.
HDL-cholesterin in males: 72.3 ± 13.3 mg/dL, in females: 63.6 ± 14.3 mg/dL (P < 0.001).
ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; DZ, dizygotic; GGT, γ-glutamyl transpeptidase; HbA1c, hemoglobinA1c; HDL, high-density lipoprotein; HOMA, homeostasis model assessment of insulin resistance; hsCRP, high sensitivity C-reactive protein; LDL, low-density lipoprotein; MZ, monozygotic; SD, standard deviation.
There was no significant difference between MZ and DZ twin subjects regarding pancreatic CT attenuation (48.9 ± 11.9 HU and 49.0 ± 13.0 HU, P = 0.934, respectively).
Age-, sex-, BMI-, and HbA1c-adjusted co-twin correlations between the siblings showed that MZ twins have stronger correlation of HU values than DZ twins (rMZ = 0.536, P < 0.001; rDZ = 0.115, P = 0.580, respectively).
Using the structural equation model, a greater unique environmental influence (E: 54%, 95% CI 19%–66%) and a moderate additive genetic dependence (A: 46%, 95% CI 34%–81%) were found. Common environmental influence was not identified (C: 0%) (Table 2).
Detailed Model Information Regarding Single Trait Classical Twin Model of Computed Tomography-Based Pancreas Attenuation
A: additive genetic factor, C: common environmental factor, E: unique environmental factor.
AIC, Akaike information criterion; BIC, Bayesian information criterion; CI, confidence interval; HU, Hounsfield unit; LL, log-likelihood; Bold, best fit model.
Discussion and Conclusion
We found a moderate additive genetic and a greater unique environmental dependence of pancreatic lipid accumulation in our twin cohort indicating that development of NAFPD is mainly driven by environmental factors (lifestyle characteristics).
Importantly, we have enrolled adult twin pairs with the mean age of 57.7 ± 9.1 years. The female predominance (64.7% in our study) has been described in previous twin studies, as female twin subjects are more willing to participate in such clinical studies than males. 34
We used nonenhanced CT images for measuring pancreatic lipid accumulation; this method was also popular among other researchers in clinical settings. 18,24 Undoubtedly, visualization of pancreas is often challenging due to inadequate coverage or image quality. In our study, we excluded some twin subjects (and their siblings) from the analysis simply due to poor pancreas image quality.
It is noteworthy that there are no consensus criteria for the CT diagnosis of pancreatic lipid accumulation. Although absolute number of attenuations was proposed for diagnosis, 23 other authors preferred to use ratio of pancreatic to splenic attenuation or difference between pancreatic and splenic attenuation. 18,24 In our study we refrained from using derived ratios or differences as we aimed to assess genetic and environmental dependence of pancreatic lipid accumulation, and crude but not derived numbers should be considered more appropriate for assessing the phenotype in statistical analysis of a classical twin study.
Although pancreatic lipid accumulation was mainly driven by environmental factors in our study, a moderate genetic effect on pancreatic fat was also documented. This observation can be based on the results of structural equation model, although co-twin correlations (rMZ > rDZ) already suggested that genetic dependence should not be considered negligible. To our best knowledge, this is the first systematic clinical observation with twin pairs documenting slightly dissimilar impact of environmental and genetic influence on development of NAFPD.
The greater environmental and a moderate genetic effect on developing NAFPD can translate to clinical practice. As pancreatic lipid accumulation was documented even in children and adolescents with overweight, 35 early and intensive preventive efforts should be implemented to reduce or at least to halt this pathological process. All modifiable lifestyle characteristics should be appropriately treated with medical nutrition therapy, regular physical activity, or behavioral interventions. Clearly, lifestyle changes and weight management should be considered as key element for preventing or decreasing pancreatic lipid accumulation. For example, bariatric surgery resulted in a significant decrease of pancreatic fat within 12 months in obese subjects. 36 In contrast, active lifestyle resulted in a beneficial effect only on hepatic but not on pancreatic lipid contents in a Finnish twin study. 27 In a recent small study, metformin therapy for 4 months did not result in any change of pancreatic CT attenuation among patients with newly diagnosed Type 2 diabetes. 37
Our results have to be interpreted within the context of their limitations. The sample size (136 twin subjects) is limited but comparable to other classical twin studies. 34 Lipid accumulation in the pancreas was assumed by CT attenuation without any histological validation. Nevertheless, this method is widely accepted, and histopathological correlations have been already published by others. 24 In our study, the zygosity was classified according to validated questionnaires, but this method is widely accepted in clinical studies. 31 The age of DZ pairs was somewhat higher compared to MZ pairs, but all models were corrected for age, sex, BMI, and HbA1c values in our study. Our results were derived from an adult twin Caucasian population; therefore, the generalizability of our findings is limited.
In conclusion, our classical twin study documented that unique environmental influences slightly outweighed additive genetic effects on the phenotypic appearance of pancreatic lipid accumulation known as NAFPD.
Footnotes
Author Disclosure Statement
S.V. is a shareholder in Global Genomics Group, LLC, and receives salary from Global Genomics Group, LLC. The authors have no other financial relationships or conflicts of interest to disclose.
Funding Information
The study was supported by a New Horizons Grant from the EASD (European Association from the Study of Diabetes) to G.J.