
Abstract
Introduction:
Handgrip strength (HGS), a simple, convenient, and economic measurement of muscle strength, is known to be related to metabolic syndrome (MetS) in adults. This relationship in adolescents, however, has not been widely examined. this study investigated the relationship of MetS (as defined by the International Diabetes Federation [IDF]'s criteria) to HGS in Korean adolescents.
Materials and Methods:
This cross-sectional study analyzed data on 2802 adolescents 10–18 years of age from the Korean National Health and Nutrition Examination Survey (KNHANES) 2014–18, which had measured and recorded HGS, body mass index, and other parameters relevant to MetS. Normalized HGS was defined as the sum of the maximum HGS from both hands normalized per weight. Complex sample multivariate logistic regression analyses were performed to investigate the relationship between HGS and MetS.
Results:
The risk of MetS decreased with increasing sex-specific quartile of normalized HGS in both boys and girls after adjustment for age (Ptrend < 0.001). Higher HGS was associated with lower odds of having MetS, such that for every 5% increase of normalized HGS, the odds were decreased by factors of 0.79 (0.73–0.85) and 0.67 (0.59–0.77) for boys and girls, respectively, after age adjustment.
Conclusions:
This population-based, nationally representative study suggests that higher HGS is associated with lower risk of MetS in Korean adolescents regardless of sex.
Introduction
Metabolic syndrome (MetS), a cluster of metabolic risks, including abdominal obesity, high blood pressure (BP), high triglyceride (TG), high fasting plasma glucose (FPG), and low high-density lipoprotein cholesterol (HDL-C), is known to be related to cardiovascular disease and diabetes in adults. 1 MetS also is observed in children and adolescents, and tends to persist from childhood into adulthood. 2 –4 MetS incidence in children and adolescents is now increasing due to the obesity epidemic and sedentary life styles, 5 and could be an even more serious public health problem in the future.
Handgrip strength (HGS), a simple, convenient, and economic measurement of muscle strength, is reported to be associated with MetS, type 2 diabetes, frailty, and overall mortality in adults. 6 –12 When performed in a standing position, absolute HGS also captures lower body and core muscle strength, which are used in balance and exertion of force. 13 By contrast, when performed in a seated position, it targets relatively smaller muscle groups and is more localized to the upper body. 13 Several previous studies investigating the relationship between HGS and MetS in adults and the elderly 6,7,14 –16 have shown inverse relationship between HGS and MetS; such relationship, however, has not been widely studied in adolescents. 17 –21 Recently, Kang et al. 22 showed that HGS is reduced in Korean adolescents with MetS relative to those without MetS. However, there is still no study on any dose–response relationship of HGS with MetS or components of MetS in Korean adolescents. Therefore, this study investigated the dose–response relationship between HGS and MetS in Korean adolescents 10–18 years of age.
Materials and Methods
Study subjects
This study was conducted using data obtained from the 2014–2018 Korean National Health and Nutrition Examination Survey (KNHANES), which is a nationwide cross-sectional survey of the general population performed by the Korea Centers for Disease Control and Prevention for noninstitutionalized South Koreans that employs a rolling sampling design entailing complex, stratified, and multistage probability clustering.
Among the 39,199 participants in the KNHANES, 3689 adolescents 10–18 years of age were selected for this analysis. The following individuals were excluded from the study: those without complete data on HGS (n = 392); those with less than 8 hr of fasting (n = 155), and those without complete data on MetS (n = 340). After these individuals were excluded, a total of 2802 participants remained eligible for this study (Fig. 1).
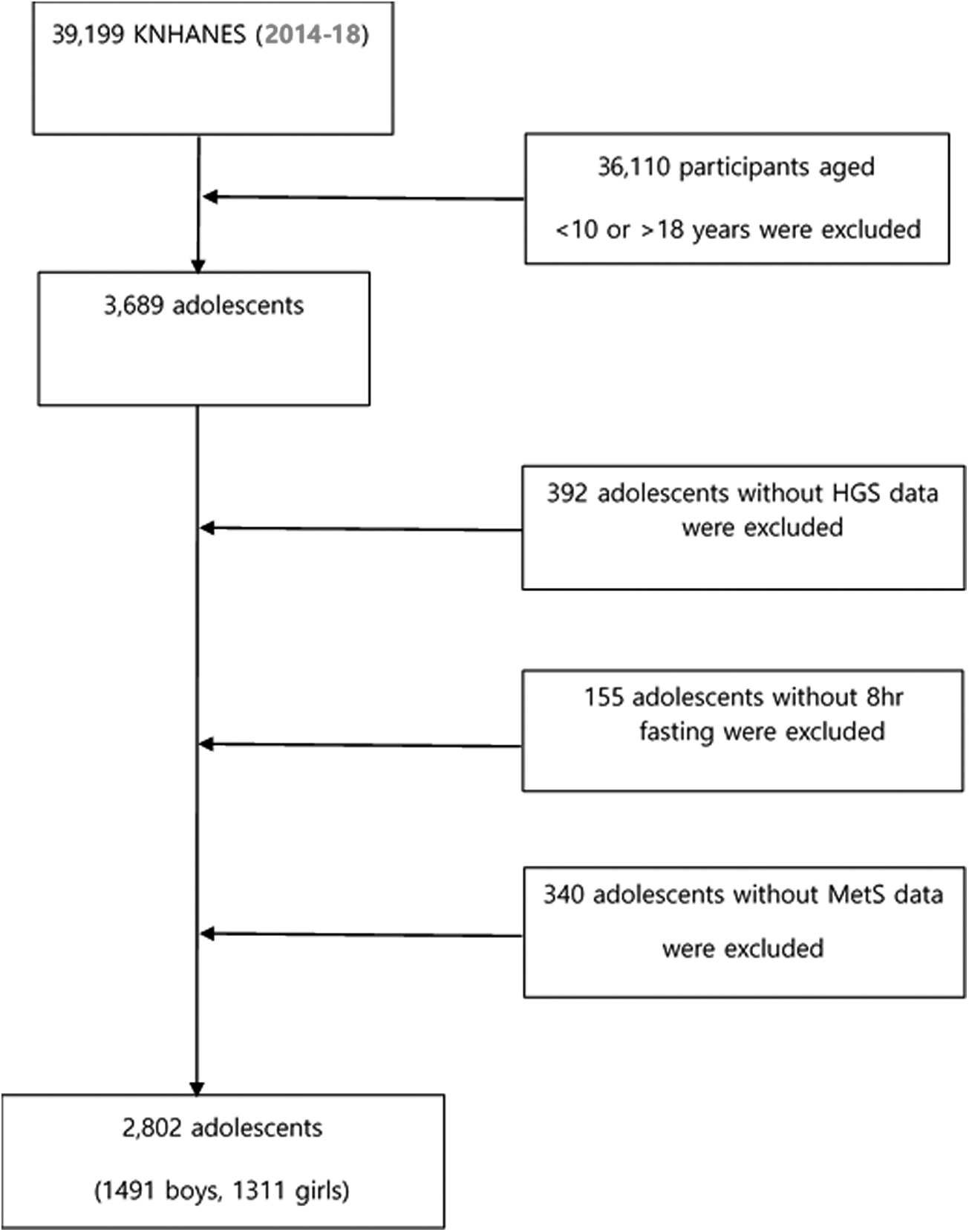
Flow diagram of study participant selection. HGS, handgrip strength; KNHANES, Korean National Health and Nutrition Examination Survey; MetS, metabolic syndrome.
All of the participants in the KNHANES had provided written informed consent for their data to be used in the study. This study and the original KNHANES study were classified under the ethical-review-exemption category by the Bioethics and Safety Act.
Clinical and laboratory measurements
HGS was evaluated thrice in each hand using a TKK 5401 digital grip-strength dynamometer (Takei Scientific Instruments Co., Ltd., Tokyo, Japan). All the subjects stood with their hands at their sides. Then, each grasped the dynamometer with one hand, whereupon each of the three trials was conducted as described below. The same procedure was then repeated using the other hand. The subjects squeezed the dynamometer with maximum effort for ∼3 sec. The maximum value of the three trials was used as the determinant of grip strength in each hand. Those with a history of wrist surgery within 3 months or any wrist discomfort were excluded from HGS measurement. Absolute HGS was defined as the sum of the maximum HGS from both hands, and normalized HGS was defined as the absolute HGS divided by body weight.
Weight and height were measured with the subjects wearing light clothing without shoes. Body mass index (BMI) was calculated by dividing the weight (kg) by the squared height (m). Waist circumference (WC) was measured at a level midway between the lowest lateral border of the ribs and the uppermost lateral iliac crest in the standing position. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) measured in the sitting position were each recorded twice at 5-min intervals and averaged for the purposes of the analysis. After at least 8 hr of fasting, blood was collected and analyzed within 24 hr. FPG, HDL-C, and TG were measured using the enzymatic method (Hitachi 7600 Automated Analyzer; Hitachi, Tokyo, Japan).
Definition of MetS
According to the International Diabetes Federation (IDF)'s criteria for children and adolescents, the subjects were classified as having MetS if they had a high WC and two or more of the indicated metabolic risk factors. 23 A high WC was defined according to the IDF criteria (age- and sex-specific WC ≥90th percentile for adolescents 10–15 years of age based on the same growth chart, 90 cm for boys 16–18 years of age, and 80 cm for girls 16–18 years of age). The criteria for the metabolic risk factors were defined as follows: blood pressure ≥130/85 mmHg, fasting glucose ≥100 mg/dL, high-density lipoprotein (HDL) <40 mg/dL for children 10–15 years of age and boys 16–18 years of age, HDL <50 mg/dL for girls 16–18 years of age, and TG ≥150 mg/dL.
Statistical analyses
The complex sample analyses were conducted with SPSS software (version 25.0; IBM, Inc., Armonk, NY, USA), using sampling weights from the KNHANES to acquire nationally representative estimates. To prevent biased results, excluded subjects were considered subgroups. The data for boys and girls were separated for further analysis owing to the sex difference in HGS. The participants were divided into four groups according to the sex-specific quartiles of normalized HGS: first (0.35–0.82), second (0.82–0.98), third (0.98–1.16), and fourth (1.16–1.76) in boys and first (0.27–0.71), second (0.71–0.82), third (0.82–0.93), and fourth (0.93–2.37) in girls. According to these quartiles, complex sample multivariate logistic regression and linear regression analyses were conducted to identify the linear relationships for categorical variables and continuous variables. The prevalence of MetS and its components in each quartile was compared, and logistic regression analysis was performed to investigate the association between the sex-specific quartiles of normalized HGS and MetS or its components, which consisted of the unadjusted and age-adjusted model.
Results
The study population included 1491 (53.21%) boys and 1311 (46.79%) girls 10–18 years of age. The average age of the study population was 14.31 (±0.07) years for boys and 14.35 (±0.08) years for girls. Table 1 provides the demographic and MetS characteristics of the study participants according to the sex-specific quartiles of normalized HGS. Participants in higher quartiles were more likely to be older than those in lower quartiles, among both boys and girls. They were also more likely to be taller among boys, and to have lower body weight among girls, compared with those in lower quartiles. The prevalence of MetS was 2.6 (±0.5%) and 2.3 (±0.5%) in boys and girls, respectively; among both boys and girls, it was found to have a significant inverse association with sex-specific quartile of normalized HGS. More than 10% of the study participants had high WC and low HDL-C, among both boys and girls, and 14.1 (±1.0%) of boys had high FPG. The prevalence of high WC, high FPG, high TG, and low HDL-C was found to have a significant inverse association with sex-specific quartile of normalized HGS among both boys and girls (Ptrend < 0.05) (Table 1).
Characteristics of Study Population According to Sex-Specific Quartiles of Normalized Handgrip Strength Among Korean Boys and Girls 10–18 Years of Age
Values are represented as weighted means or weighted proportions with standard error for continuous or categorical variables.
BMI, body mass index; DBP, diastolic blood pressure; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; HGS, handgrip strength; SBP, systolic blood pressure; TG, triglyceride; WC, waist circumference.
Tables 2 and 3 show the crude and age-adjusted OR of MetS and its individual components according to the sex-specific quartiles of normalized HGS in boys and girls, respectively. After age adjustment, the participants in the highest quartile of normalized HGS had 95% and 97% lower odds of having MetS among boys and girls, respectively, compared with those in the lowest quartile. Participants with higher normalized HGS (per 5% increase of normalized HGS) had significantly lower odds of having MetS (OR 0.79; 95% confidence interval [CI] 0.73–0.85 for boys, OR 0.67; 95% CI 0.59–0.77 for girls), again after adjustment for age. Boys with higher normalized HGS had significantly lower odds (per 5% increase of normalized HGS) of having any of the components of MetS, including high WC (OR 0.68; 95% CI 0.64–0.73), high BP (OR 0.90; 95% CI 0.85–0.96), high TG (OR 0.90; 95% CI 0.86–0.95), and/or low HDL-C (OR 0.91; 95% CI 0.87–0.95), after adjustment for age. Girls showed the same trend, but for the MetS components, including high WC (OR 0.69; 95% CI 0.64–0.74), high FPG (OR 0.92; 95% CI 0.85–0.99), high TG (OR 0.86; 95% CI 0.80–0.92), and/or low HDL-C (OR 0.91; 95% CI 0.86–0.96), after adjustment for age.
Odds Ratio (95% Confidence Interval) of Metabolic Syndrome and Its Components According to Sex-Specific Normalized Handgrip Strength Quartiles in Korean Boys 10–18 Years of Age
Analyzed by (multivariate) logistic regression analysis.
Age adjusted.
MetS, metabolic syndrome.
Odds Ratio (95% Confidence Interval) of Metabolic Syndrome and Its Components According to Sex-Specific Normalized Handgrip Strength Quartiles in Korean Girls 10–18 Years of Age
Analyzed by (multivariate) logistic regression analysis.
Age adjusted.
Discussion
This study investigated the dose–response relationship between HGS and MetS in Korean adolescents 10–18 years of age. An inverse association of MetS and its components with sex-specific quartile of normalized HGS was found in both boys and girls. The risk of MetS decreased with increasing sex-specific quartile of normalized HGS in both boys and girls after adjustment for age. Higher HGS was associated with lower odds of having MetS, such that for every 5% increase of normalized HGS, the odds were decreased by factors of 0.79 (0.73–0.85) and 0.67 (0.59–0.77) for boys and girls, respectively, after age adjustment.
In this study, the prevalence of MetS was 2.6 (0.5%) and 2.3 (0.4%) in boys and girls, respectively. These results were similar to those of a study analyzing data from KNHANES 2007–2008, in which the prevalence of IDF-defined MetS was 2.7% and 2.1% in boys and girls 10–19 years of age, respectively. 24 This result was lower compared with a US study on adolescents 12–19 years of age based on NHANES 2011–2014 data: 6.04% and 2.28% for boys and girls, respectively. 25
This study found that higher normalized HGS was associated with lower prevalence of MetS. This finding agrees with previous studies conducted in other countries. The HELENA study conducted with 709 adolescents 12.5–17.5 years of age from 10 European cities reported that muscular fitness using HGS and the standing long jump was negatively associated with clustered metabolic risk, independent of cardiorespiratory fitness. 26 The OR for having a high clustered risk was 5.3 in the least-fit quartile compared with the most-fit quartile for muscular fitness. In a study on 1421 sixth-grade US students, normalized HGS was independently associated with lower cardiometabolic risk in both boys and girls. 17 Another study, this one on 1326 US sixth graders, also showed that for each 5% decrease in muscle strength, boys and girls were 1.48 and 1.45 times more likely, respectively, to have a deleterious cardiometabolic risk phenotype independent of cardiorespiratory fitness and physical activity. 18 Furthermore, in a prospective 2-year follow-up study, adolescents with low normalized HGS had a significantly greater prevalence of health decline or poor health persistence compared with those who were strong, and those who were strong were more likely to maintain and improve health. 27 Another prospective study of 737 children followed up for 20 years also showed high muscle strength to be associated with decreased risk of developing adult MetS independent of cardiorespiratory fitness. 28 These results suggest that early strength acquisition prevents development of MetS in children and adolescents.
In this study, HGS, to restate, was negatively associated with MetS in both boys and girls, which agrees with most of the relevant previous studies. 17,18,26,27 However, in a study on 1376 Canadian children and youth 6–19 years of age, HGS was negatively associated with cardiometabolic z-score only in girls, and not in boys. 21 It remains unclear as to why such an association would be observed only in girls. Differences in study design, population, sample size, confounders, and measurement of HGS might have been contributing factors.
This study has some limitations: (1) The cross-sectional nature of the study design precluded any causal inference. (2) Even though age was adjusted for as a confounding factor, unmeasured factors that are known to be related with MetS such as short duration of sleep, excessive screen time, specific dietary factors, low physical activity, and tobacco smoke exposure might have contributed to the inverse associations observed. 29 (3) This study was conducted with a population of exclusively Korean adolescents, which could limit the generalizability of the results to other populations. This study's strengths include the following: (1) consideration of a nationally representative sample of Korean adolescents with sampling weights and (2) objective measurement of HGS and components of MetS, respectively.
In a nationally representative sample of Korean adolescents, those with greater levels of normalized HGS were found to be less likely to have MetS or most of its components. These results suggest that HGS in a clinical setting could be used in screening and early detection procedures, particularly in adolescents at risk for MetS. Further research is needed to define normative data and cut points for the low muscle strength to increase its utilization in medicine beyond cardiometabolic biomarkers.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this work.