
Abstract
Aims:
The purpose of this study was to investigate the effects of a 12-week aerobic and resistance training program on waist circumference (WC) and carotid intima-media thickness (CIMT) in abdominal obese middle-aged women.
Methods:
Subjects were 40 middle-aged women with abdominal obesity (WC >85 cm) but no specific diseases. Subjects were divided into a combined exercise group (aerobic and resistance exercise) and a control group that did not participate in any lifestyle modification. Carotid variables were measured using B-mode ultrasound. A treadmill exercise test was conducted to directly assess the peak oxygen uptake (VO2peak). Differences in the carotid variables and relative changes between baseline and after 12 weeks were evaluated.
Results:
After 12 weeks, body weight (70.6 ± 7.8 to 65.6 ± 6.3 kg, P < 0.05), WC (88.8 ± 3.6 to 85.6 ± 3.1 cm, P < 0.01), total cholesterol (215.5 ± 38.4 to 188.2 ± 25.8 mmHg, P < 0.05), low-density lipoprotein cholesterol (150.5 ± 30.6 to 131.6 ± 22.3 mmHg, P < 0.05), triglycerides (164.5 ± 82.3 to 119.9 ± 60.6 mmHg, P < 0.01), VO2peak (24.2 ± 6.2 to 28.7 ± 4.4 mL/kg/min, P < 0.01), and CIMT (0.61 ± 0.13 to 0.58 ± 0.12 mm, P < 0.05) were significantly improved in the combined exercise group but not in the control group; changes in CIMT were associated with changes in WC decrease (r = 0.41, P < 0.01) and VO2peak (r = −0.53, P < 0.01).
Conclusions:
Combined exercise training in abdominal obese women decreased CIMT; these changes were also associated with reduced WC and improved V
Introduction
Obesity is directly related to a high risk of atherosclerotic disease and an increased risk of morbidity and mortality from cardiometabolic diseases. 1 –3 In particular, abdominal obesity is strongly associated with insulin resistance, dyslipidemia, and systematic inflammation, resulting in cardiovascular diseases (CVDs). 4 In addition, abdominal obesity is associated with a higher risk of CVD in women than in men. 4,5
Carotid artery parameters, such as carotid intima-media thickness (CIMT) and carotid artery flow velocity, are independent risk factors for CVD. 6,7 CIMT is an independent risk factor for CVD, 7 and an increase in body fat mass is closely associated with an increase in CIMT. 8,9 Furthermore, increased CIMT, as an early sign of CVD, is associated with an increased risk of developing coronary heart disease and stroke. 10 Arterial stiffness or atherosclerosis is one of the most important factors of CVD, as it is a meaningful clinical indicator related to vascular degradation in abdominal obesity. 11
Obesity increases the risk of arteriosclerosis; however, regular exercise is known to effectively decrease obesity; there are numerous efforts to find optimal exercises, such as resistance exercises, that can help to reduce obesity. 12 –14 For this reason, a combination of aerobic and resistance exercises is more effective in reducing body fat and function rather than a single exercise. 15,16
Studies on postmenopausal obese women have shown that combined exercise over 12 weeks improves not only weight and body fat loss but also arterial rigidity, such as brachial-ankle pulse wave velocity. 15,17 However, a systematic review by Roberson et al. examined the association between healthy obesity and subclinical carotid atherosclerosis but found the results to be contradictory. 18 Furthermore, numerous obesity studies have focused mostly on menopausal women, and there are not enough studies on whether regular exercise has a direct effect on improving vascular function in healthy obese women who are not menopausal.
Aim
The aim of this study was to investigate the effects of combined exercise training on CIMT progression in abdominal obese middle-aged women.
Methods
We recruited 62 healthy abdominal obese subjects based on the Korean Society for the Study of Obesity guideline criterion; abdominal obesity, operationally defined as a waist circumference (WC) >85 cm, 19 was determined by participants who had enrolled in a hospital-sponsored health examination program at Samsung Medical Center, Seoul, South Korea, between January 2, 2019 and December 31, 2019, and had their cardiometabolic risk factors, CIMT, and cardiorespiratory fitness (CRF) measured. All participants were free of CVDs, hypertension, and type 2 diabetes. Written informed consent was obtained from all participants before participating in the health screening program. In accordance with the ethical standards of the Declaration of Helsinki, informed consent was obtained from all participants after they were provided with a detailed description.
The exercise group consisted of 32 subjects who enrolled in a lifestyle modification class that included exercise training. The control group consisted of 30 subjects who chose not to participate in the lifestyle intervention program. After the 3-month intervention, all testing procedures were repeated as described earlier.
WC was measured in the horizontal plane midway between the superior iliac crest and the lower margin of the last rib. 20 Blood samples were collected in the morning after a 12-hr overnight fast and analyzed in the hospital clinical laboratory, as previously described.
CRF was directly measured using peak oxygen uptake (VO2peak) during maximal or symptom-limited treadmill exercise testing (Jaeger Oxycon Delta, Wurzburg, Germany). During exercise, heart rate was recorded continuously, and blood pressure (BP) was assessed at the end of each stage and at peak exercise. VO2peak was defined as the highest value for the plateau in oxygen uptake and expressed relative to body weight [mL/(kg·min)].
We evaluated CIMT as a marker of subclinical carotid atherosclerosis. Carotid artery ultrasound imaging was performed using a high-resolution B-mode ultrasound system (Logiq 7; GE Medical System) with a 5–13 MHz linear array transducer. CIMT was measured as the distance between the leading edge of the lumen–intima interface and the leading edge of the media–adventitia interface of the far wall of the carotid artery with the patient in the supine position. CIMT was obtained 10 mm proximal to the carotid bifurcation. The overall maximal CIMT was defined as the mean of the maximal intima-media thickness (IMT) and was averaged for the left and right sides. The prevalence of subclinical atherosclerosis was defined as a mean IMT greater than the 75th percentile. 21 Participants with a maximal IMT >1.2 mm due to atherosclerotic plaque were excluded.
The Exercise Program was designed to be 12 weeks long with a combination of aerobic training (AT) and resistance training (RT). The 12-week combined exercise program intervention consisted of sessions lasting 50–80 min, 5 days per week. Aerobic exercises, such as walking, cycling, and swimming, for 30–50 min per session, were performed at an intensity of 60%–70% of max heart rate or at a rating of perceived exertion of 13–15. Resistance exercises were performed with elastic band exercises (Thera-Band, Ohio) for eight movements (deadlift, squat, shoulder press, reverse flies, sideband, sit-up, push-up, and ankle plantar flexion) with 10–15 repetitions per set, 2–3 sets (1-min rest between sets), and 20–30 min per session for 3 days per week. Every 2 weeks, subjects came back to the hospital to meet with an exercise physiologist to check and update their exercise prescription. Their exercise logs and charts were also checked at this time to ensure that they adhered to the exercise prescription. Diet education was provided initially and then every 2 weeks by a dietitian, with the aim of reducing total energy intake and providing a healthy diet for weight control. The control group received an initial consultation with both an exercise physiologist and a dietician and received written educational materials. There was no contact with the control group after the initial consultation, until the follow-up 3-month later.
The Statistical Package for SPSS version 17.0 (SPSS Inc., Chicago, IL) was used for statistical analysis. A Student's t-test was used to assess differences in baseline variables. Data were presented as mean ± standard deviation and as proportions for categorical variables. The response to the combined exercise program was evaluated using 2 × 2 (group by pre- vs. postintervention) analysis of variance (ANOVA) with repeated measures. If significant interactions were present, a paired sample t-test with Bonferroni correction was performed to identify differences within the group to evaluate the independent contribution of changes in body weight and changes in VO2peak to changes in CIMT. Statistical significance was set at P < 0.05.
Results
Physical characteristics of participants at baseline are shown in Table 1. All participants completed the intervention for 12 weeks. Table 2 presents changes in body composition and WC for 12 weeks. After 12 weeks of exercise training, the groups showed a significant reduction in body weight (7%, P < 0.01), body mass index (6%, P < 0.01), percent fat (7%, P < 0.05), and WC (4%, P < 0.01). There was no change in these variables in the control group.
Subjects of the Exercise and Control Groups at Baseline
Data are expressed as mean ± SD.
BMI, body mass index; SD, standard deviation; WC, waist circumference.
Change in Obesity Index
Values are mean ± SD.
P < 0.05, ** P < 0.01, change within groups.
P < 0.05, ## P < 0.01, group × time interaction.
Table 3 presents changes in BP, serum lipids, and CRF (VO2peak). In the exercise group, there were significant reductions in systolic BP (3%, P < 0.05), total cholesterol (12%, P < 0.05), low-density lipoprotein cholesterol (LDL-C) (12%, P < 0.05), and triglycerides (TGs) (27%, P < 0.01) and a significant increase in VO2peak from 24.2 ± 6.2 to 28.7 ± 4.4 mL/(kg·min) (18%, P < 0.01). There was no change in these variables in the control group.
Changes in Blood Pressure, Serum Lipid Levels, and Peak Oxygen Uptake
Values are mean ± SD.
P < 0.05, ** P < 0.01, change within groups.
P < 0.05, ## P < 0.01, group × time interaction.
DBP, diastolic blood pressure; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; TC, total cholesterol; TG, triglyceride; VO2peak, peak oxygen uptake.
Figure 1 shows the comparison of the mean CIMT values between the groups after 12 weeks of exercise. In the ANOVA analysis results, CIMT (P < 0.05) showed significant group × time interactions (P < 0.05), In the paired t-test results for the exercise group, CIMT significantly decreased, from 0.61 ± 0.13 to 0.58 ± 0.12 mm (3%, P < 0.05). However, the control group showed no change in CIMT or carotid artery parameters.
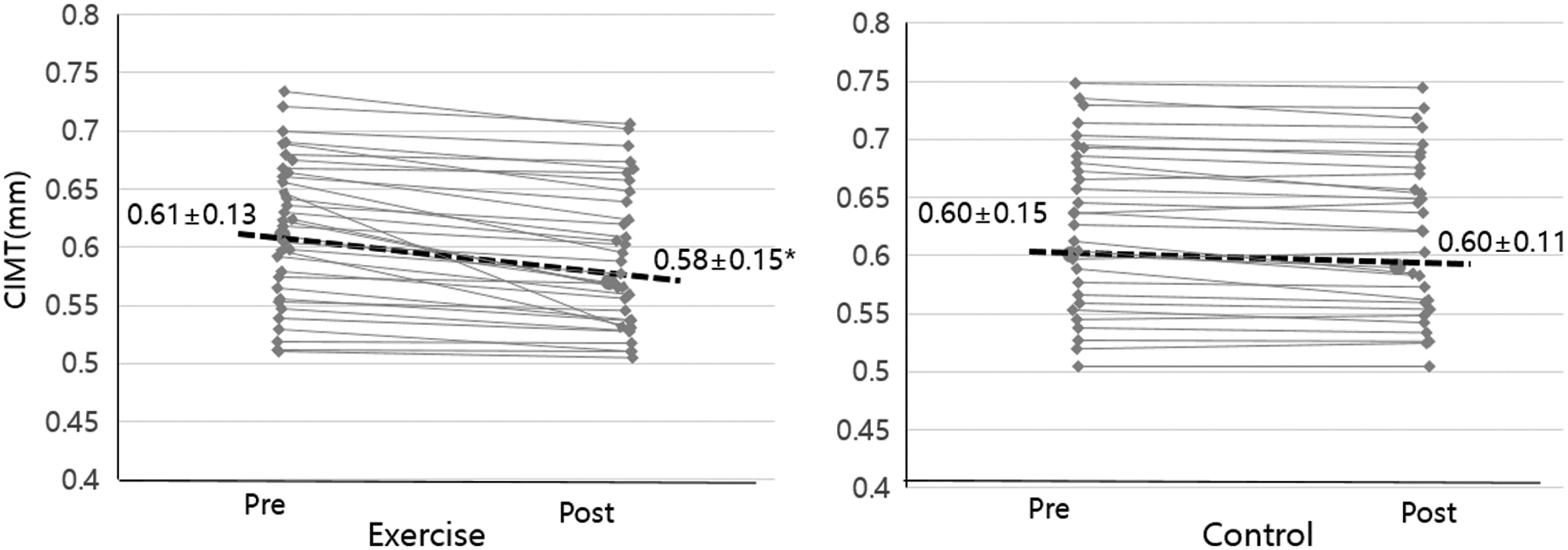
Changes in intima-media thickness in the carotid artery. *P < 0.05, change within groups.
Factors that influenced CIMT according to change in variables after exercise training are shown in Table 4. Changes in body weight and WC were associated with changes in CIMT (separately, r = 0.41, P < 0.01, r = 0.40, P < 0.01). Changes in VO2peak were also associated with changes in CIMT (r = −0.53, P < 0.01), and these changes were still significant after adjustment for changes in weight loss (r = −0.35, P < 0.05).
Correlation of Change in Parameters and Carotid Intima-Media Thickness After Exercise Training
P < 0.05, ** P < 0.01.
Δ, difference between pre- and postvalue; CIMT, carotid intima-media thickness.
Discussion
Twelve weeks of combined exercise training in abdominal obese middle-aged women resulted in weight loss and improvements in blood lipid levels and cardiopulmonary fitness. Moreover, CIMT was significantly decreased. This study demonstrated that key benefits could be achieved in healthy obese women after as little as 12 weeks of a training program.
Obesity, especially abdominal obesity, is an independent risk factor for CVDs. 5,13,22 Abdominal obesity in women elevates the risk of CVD more than that in men. 4 Exercise is a well-known and effective method to lose weight and reduce visceral fat in the abdominal cavity. 13 Various studies have attempted to find an exercise suitable for effective weight loss. A study by Willis et al. compared the effects of AT, RT, and combined training (AT/RT), and found that body weight and body fat were decreased in both the AT and AT/RT groups but not in the RT group. 23 This demonstrates that AT is essential to reduce body fat. Moreover, body fat percentage and WC were significantly decreased in the AT/RT group that performed both AT and RT.
In our study, because only AT/RT was performed, it was not possible to compare our results to other types of exercise. However, abdominal circumference was decreased by an average of 3 cm after 12 weeks of exercise. This reduction in WC is especially important as it is considered to be an independent cardiovascular risk factor. 22 In the exercise group, TG and LDL-C were also significantly decreased, and combined exercise training showed a positive effect on serum lipid levels, which improved the risk index of metabolic diseases. Numerous previous studies have demonstrated that regular exercise, similar to our study, helps to improve serum lipid levels. 24 In obese people, if not accompanied by weight loss, the improvement of serum lipid levels is only temporary. 19,25 Therefore, it is critical for obese people to supplement positive changes in serum lipid levels with weight control.
Obese people have increased CIMT, which is a potential risk factor for myocardial infarction and stroke. 6,7 The intima and media of the carotid artery are composed of endothelial cells, connective tissue, and smooth muscle, and fat tends to accumulate in this region. CIMT is ∼0.25–1.5 mm in healthy subjects, and clinically, a CIMT >1.0 mm is reported to increase the risk of diseases. 26 Although the mechanism by which abdominal visceral fat can affect the carotid artery is unclear, visceral fat causes hyperglycemia and hyperinsulinemia, which increases free fatty acid secretion. Elevated levels of free fatty acids increase vascular tone and adrenergic responsiveness to arterial stiffness. 27 Therefore, weight loss and abdominal fat loss may have a positive effect on carotid artery improvement; a previous meta-analysis of obese people reported a high correlation between weight loss and CIMT. 28 Recently, Byrkjeland et al. showed that a combination of aerobic and RT in people with type 2 diabetes and coronary artery disease led to a significant decrease in CIMT. 29 In our study, subjects were healthy obese people with a CIMT mostly in a normal range, and improvements in CIMT were observed after 12 weeks of training.
Moreover, training improved cardiopulmonary fitness by 18% for middle-aged women, which is another health benefit. As demonstrated in previous studies, improvement of cardiopulmonary fitness is a crucial factor for reducing the prevalence of metabolic syndrome and mortality in obese people. 18,30,31 In this study, training for as little as 12 weeks resulted in decreased CIMT, which confirms that this decrease is closely related to the improvement of cardiopulmonary fitness.
A limitation of this study was it is difficult to generalize this study result for all women because our study had limited to middle-aged women in subjects. The menopause and menstrual cycles of women were not considered in this study due to unpredictable physiological phenomenon. Furthermore, because we did not have dietary information to evaluate the specific influence of diet, including alcohol intake, we could not determine how specific diet alterations influenced CIMT.
Conclusions
This study revealed that 12 weeks of combined exercise training significantly reduced CIMT and WC. It also effectively improved CRF in abdominal obese middle-aged women. Therefore, we suggest that regular combined exercise contributes to a lower risk of CVD in abdominal obese individuals.
Footnotes
Acknowledgments
We thank the Samsung Medical Center physicians and technicians for collecting the baseline data.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this work.