
Abstract
The effect of the growth hormone (GH) in promoting linear growth is well known; however, less recognized by practitioners especially pediatric, are its metabolic properties. This may be because the deleterious effects of improperly treated or untreated growth hormone deficiency (GHD) can present beyond the pediatric years. In addition, clinicians may lack familiarity with the potential issues that can arise due to inadequately treated GHD. Considering information from both the basic sciences research and clinical medicine, pediatric practitioners should be cognizant about the metabolic effects of GH. They should also be equipped to provide anticipatory guidance to patients regarding the importance of adherence to therapy in GHD and be prepared to transition patients with permanent GHD from pediatric GH supplementation to adult GH dosing. With a lack of proper transitioning, adverse outcomes may present beyond childhood.
Background
A 17
Her initial hemoglobin A1C (HbA1c) was 9.1%. Traditional basal/bolus insulin therapy was initiated, with conventional dosing requiring rapid escalation to peak total daily insulin dose of 2.9 U/kg/day (∼155 U/day). Comprehensive evaluation for conditions associated with insulin resistance (IR) was negative; however, a diagnosis of GHD was made, based on Arginine/Clonidine stimulation testing showing peak GH level 0.8 (normal ≥10 ng/mL).
GH supplementation was initiated at 0.3 mg daily and titrated based on insulin-like growth factor (IGF)-1 levels. Magnetic resonance imaging (MRI) of the brain and abdomen indicated a small anterior pituitary gland and liver masses, respectively. Liver biopsy showed steatohepatitis with bridging fibrosis. Though her diabetes was not fully reversed with GH, her HbA1c decreased to 5.9% and 5.8% (normal 4.0%–5.6%) at 6 and 19 months, respectively. Insulin therapy requirement decreased to 1.9 U/kg/day at 12 months after diagnosis, and quality of life scores improved. Her liver masses remained stable on GH therapy and her initial transaminits, lipid profile, and blood pressure improved. 1
Although this case is not common, it is instructive that her presentation may be explained by her relative naivety to GH from 7 years old and the fact that she was not supplemented with GH for years when she clearly had GHD.
Introduction
The history of GH administration and the evolution into the GH product administered today are quite interesting. Interesting also are its effects on metabolism, particularly carbohydrates and fat. 2,3
However, before the discovery of its metabolic effects, the growth-promoting properties of GH were recognized. In 1958, an editorial published by Raben in the Journal of Clinical Endocrinology and Metabolism titled “Treatment of a pituitary dwarf with human GH” outlined the merits of GH therapy when used to treat a 17-year-old male with GHD. During treatment with GH, this patient had an annualized growth velocity of 2.6 inches when compared with 0.5 inch before treatment. 4
GH: Issues Impacting the Diagnosis of Pediatric GHD and Therapy
In the 1950s and continuing in the early 1980s, GH was sourced from cadaveric pituitary extracts. However, in 1985, a 22-year-old patient receiving GH therapy developed Creutzfeld-Jacob disease, a “slow virus” encephalopathy. Around that time, a total of three adults in the United States and one in Canada who received therapy with the pituitary-derived extract had a similar fate. 5 Fortuitously, that same year, GH manufactured by DNA technology was approved in the United States and this resulted in an increased supply of a product that was once rationed. 6,7 Today, the dispensing of the product has been driven somewhat by pharmaceutical interests and this has coincided with a change in the cut-off levels, below which GHD is diagnosed overtime (10 ng/mL in pediatrics vs. 5 ng/mL, which was used when GH was derived from pituitary extracts) without much scientific basis to validate this practice variation. 8
The adoption of a cut-off level of 10 ng/mL was based on this being the GH level, just below the mean response elicited on GH stimulation testing. Further, this single cut-off level below which one is seen as having GHD is used, despite the recognition that there is differential stimulation of GH production by different provocative agents. This cut-off level of 10 ng/mL facilitates the treatment of children considered as having partial GHD. The argument for offering these individuals treatment is that GH production should be considered as falling on a continuum from normal production to that of a GH-deficient state. 9,10
In the United States and some European countries except for Australia where auxologic criteria primarily drive the prescribing of GH, provocative testing plays an integral part in the diagnosis of GHD. 11,12 General criteria, which suggests the need for provocation testing during a short stature evaluation, include: a decrease in a patient's height standard deviation score (SDS) not in keeping with an established familial pattern or a change in his/her height below-2 SDS and/or a change in the height velocity pattern. 13
For years, the insulin tolerance test was seen as the gold standard in provocation testing based on its ability to test the integrity of the pituitary gland and, as such, result in GH release; however, it has now become historical in many places. 14,15 This relegation has occurred due to the risks of seizures, hypoglycemia, and even death. 16
Other agents utilized for provocation testing include arginine, glucagon, L-Dopa, and GH-releasing hormone. 16 –18 More recently, macimorelin, a parenterally administered ghrelin mimetic, has been approved for establishing the diagnosis of adult GHD; however, further studies are needed to establish its efficacy in children, adolescents, and obese adults. 19,20 There are, however, a number of issues that can potentially affect these tests, such as the body mass index (BMI) SDS, the inherent lack of test reproducibility possibility due to the intrinsic subject variation at a given time in response to the particular agent that modulates GH release, and the effect of sex steroid priming. 21 –23 Studies have shown an attenuation of the GH response with increasing BMI. In support of this variation of GH levels with BMI, is that with weight loss there is a return to normal GH production. 24 –26
Sex steroid priming arguably prevents the inappropriate treatment of patients with constitutional delay of puberty by improving the diagnostic specificity of stimulation testing. Despite this being a recommendation, it is not routinely followed. 26
Another key issue that impacts clinical decision making and the decision to start GH therapy is the variation in standards affecting GH assays over the years. Historically, radioimmunoassay was the methodology for quantifying GH production; however, newer immunometric assays that have increased specificity are currently being used. Based on varying specificities for different GH isoforms, the issues of discrepancies in test interpretation may arise primarily due to testing antibodies with varying specificities that depend on the GH isoform used. 27 Though the most recent consensus statement and commutability standard recommends that harmonized GH assays use the somatropin standard, International Reference Preparation (IRP) IS 98/574, 22 k recombinant human GH (rhGH) isoform, this is not routinely adhered to worldwide. 28
Based on the various issues affecting the performance of GH provocative tests, specifically their specificity, it is not surprising that many patients are misclassified as having childhood GHD and, as such, qualify to receive GH therapy during the pediatric years. With the increased GH use in this population fueled by increased GH supply that was generated by the Food and Drug Administration's (FDA's) approval of rhGH in 1985, today the long-term complications that could develop in children with untreated GHD are uncommon. Nonetheless, the issues that potentially may arise and could be viewed as being a part of the natural history of untreated GHD provide insight as to GH's importance beyond the growing years.
GH: Metabolic Implications of Deficiency
With the increased GH use after the approval of rhGH, it was apparent that GH supplementation could abrogate certain metabolic issues seen during the natural history of patients with untreated GHD. Before 1985, when the FDA approved the use of rhGH, it was not feasible to conduct trials with GH replacement in adults. This is despite some speculation that a GHD syndrome could develop in patients with true GHD who had not been replaced after their linear growth was complete. Much of this speculation was driven by data showing an increased mortality in patients with hypopituitarism who had received adequate hormonal replacements with the exception of GH supplementation. 29 However, in 1987, the FDA approved the use of rhGH for adults in the United States with GHD either acquired or newly diagnosed, based on diseases affecting the pituitary and hypothalamus. 30 With this approval that facilitated treatment, the emergence of a GHD syndrome was recognized and this includes, reduced psychological well-being, decreased bone mineral density (BMD), accompanied by metabolic and body composition abnormalities. 31,32
It was instructive that early in the era of recombinant GH therapy, a seminal case report outlined the resolution of steatohepatitis with GH administration in a 17 year-old patient treated initially with levothyroxine and hydrocortisone alone for panhypopituitarism. 33
Both animal models and evidence from human studies support the association of GHD with steatohepatitis. To appreciate this association, knowledge of signal transduction involving GH is important. Initially, GH acts by binding to a growth hormone receptor (GHR), which consists of an extracellular N-terminal ligand-binding domain linked to a C-terminal domain located intracellularly. The GHR is a member of the cytokine receptor family involved in signal transduction. 34 –36 When GH binds to its receptor, a homodimer, there is a conformational change that results in signal transduction. 37 –39 Specifically, there is recruitment of Janus kinase 2 (JAK2) with the binding of GH to the GHR, and by a process of phosphorylation its enzymatic activity is promoted. 40 With this initial phosphorylation, there is subsequently phosphorylation of tyrosine residues on the part of the GHR located intracellularly. It is this portion that functions as a docking site for a group of proteins termed collectively as signal transducers and activators of transcriptions (STATs). Please refer to Fig. 1,which illustrates GH signal transduction and certain pathways in the association between GHD and hepatic steatosis. These STAT proteins perform a crucial role in the GH's mediated transcription of the IGF-1 gene. 40 Based on this action, GH is important in improving insulin sensitivity and serum lipid profile and with this, it results in amelioration of steatohepatitis.
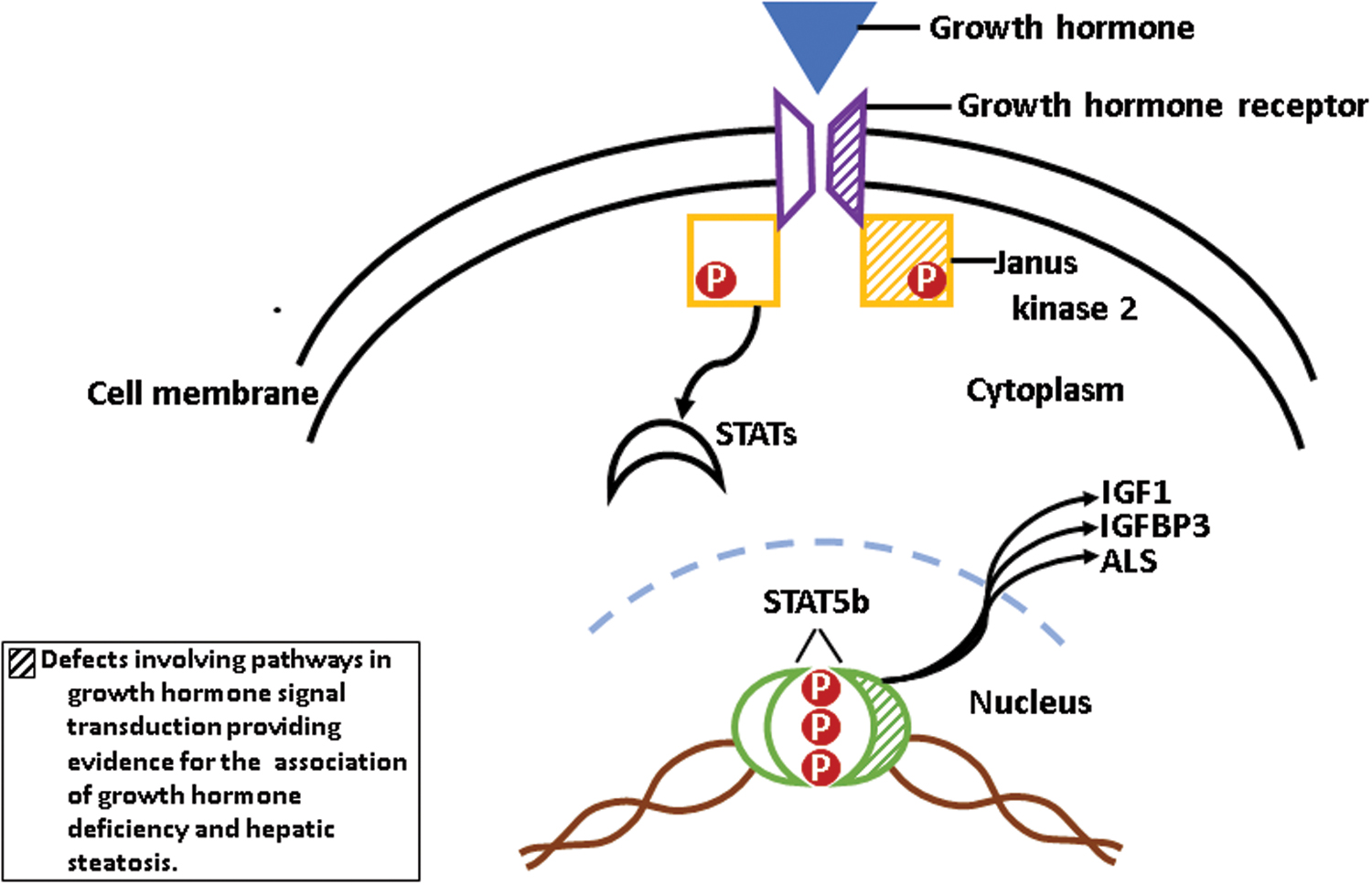
GH signal transduction and certain pathways in the association between GHD and hepatic steatosis. GHD, growth hormone deficiency. Color images are available online.
In the mouse model with liver-specific, near-total deletion of the GHR (GHR-L), hepatic steatosis is seen. With this deletion there is increased IR, glucose intolerance, increased circulating GH levels, and free fatty acids. With the reconstitution of hepatic GHR signaling, there is restoration of triglyceride output to normal levels, illustrating that GH signaling is essential in the regulation of lipid metabolism. 41
In another similar mouse model though IR develops, when there is restoration of the liver's IGF-1 expression by a hepatic transgene that serves to isolate the possible IGF-1 effects on lipid metabolism, both insulin sensitivity and serum lipid profile are improved. However, in this model, hepatic steatosis still occurs. This illustrates the direct action of GH and not IGF-1 on lipogenesis and also lipid uptake. 42
Several mouse models have also corroborated the association of GHD with IR. In mice with global GHR knockout; metabolic syndrome, steatohepatitis, increased inflammation, liver fibrosis, and hepatic tumor develop. 43 Other mouse models have also elucidated the impact of GHD on β cell function. In mice with isolated congenital GHD, β cell function deteriorates, and this deterioration of function is not attributable to a change in their cell mass. 44 In vitro GH not only stimulates β cell proliferation but it can also stimulate both insulin gene expression and glucose-induced insulin release. 45
Since steatohepatitis represents hepatic IR, not surprisingly T2DM, the most extreme state of IR, may also be ameliorated by GH therapy. 46 These findings illustrate the effect of GH on intermediary metabolism, specifically its effects on both carbohydrate and lipid metabolism. For its effects on carbohydrate metabolism, GH has two recognized phases, with the initial being an insulin-like effect and then a later effect. The initial insulin effect results in a decrease in blood glucose and free fatty acids. Its later effects include: gluconeogenesis and fat mobilization, with the potential for the development of impaired glucose tolerance in the process. 2,3 Regarding lipid metabolism, based on the mobilization of free fatty acids from adipose tissue and their subsequent elevation, GH indirectly affects glucose oxidation and causes decreased glucose utilization, which is responsible for hyperglycemia development. 47
Another point that illustrates the impact of GH on intermediary metabolism is that men with hypopituitarism who have been replaced with levothyroxine and hydrocortisone at baseline have a high prevalence of non-alcoholic fatty liver disease (NAFLD) in the absence of GH therapy. When treated with GH, histological improvement has been shown in the liver of these men and this demonstrates that NAFLD is predominantly attributable to GH. 48 Incidentally, NAFLD has emerged as a common cause for pediatric liver transplantation, even in people without GHD. 49 So, decreasing a possible contributor to its occurrence by GH supplementation in patients with GHD may lessen the public health burden, although causing a small decrease. This could also possibly lead to improved health outcomes, which could translate to health care dollars saved.
In addition, clinical reports involving Laron syndrome, primary GH insensitivity involving a molecular defect in human GHR, have documented the development of NAFLD. This point further illustrates the effect of GH on intermediary metabolism and in a few patients based on the severity of IR, T2DM may develop. 50
Though the time frame within which metabolic issues secondary to GHD may arise is currently unknown, the relationship between GH, lipid, and glucose metabolism is becoming clearer. Adams et al. documented a median time of 3 years between the development of NAFLD, elevated blood glucose, and dyslipidemia in patients with pituitary dysfunction (mean age at diagnosis 30 ± 20 years). In this study, of the 18 patients with a long-term follow-up of 66 ± 33 months, 2 required liver transplantation and 2 patients died from liver-related causes. 51
It has also become clear that childhood onset growth hormone deficiency (CO-GHD) represents a distinct entity from GHD starting in adult life based on the gamut of adverse metabolic effects seen. When compared with patients who develop GHD as adults, patients with CO-GHD tend to have lower BMI, waist-to-hip ratio, serum IGF-1, and poorer social outcomes. 52,53 Continued use of GH beyond epiphyseal closure facilitates the normal continued dimorphic development of males versus females in terms of the acquisition of lean body mass and fat mass. So, in addition to the metabolic abnormalities that can develop, untreated CO-GHD may result in a lack of normal sexual dimorphism, a GH-dependent process that targets body composition even beyond the age where treatment with GH supplementation usually ends. 53
In a study to investigate the metabolic effects of GH, adolescents with severe GHD who had discontinued GH for more than 2 years had the accumulation of important cardiovascular risk factors associated with GHD traditionally seen in adults. Johannsson et al. showed that with this discontinuation of GH, total serum and low-density lipoprotein-cholesterol and apolipoprotein B levels were increased, whereas the serum concentration of high-density lipoprotein C was decreased when compared with GH-sufficient individuals. 54
Moreover, in patients with non-idiopathic GHD, there is a relationship between adverse lipid profile and the duration of interruption of GH therapy during childhood and adolescence. It is believed that the longer the period of relative naivety to GH (in patients with severe GHD), the greater the likelihood of developing adverse metabolic consequences such as hyperlipidemia. 55
In addition to the indirect effects of GH on the cardiovascular system, the direct adverse effects of GHD on the cardiovascular system have also been studied. Apart from linear growth, GH also modulates the size of cardiomyocytes. 56,57 Patients with CO-GHD also have decreased cardiac function. 58
GH also impacts skeletal muscle mass and BMD. When compared with controls, patients with GHD have both lower BMD and muscle mass. 54,59 With GH therapy, bone turnover markers and microarchitecture can also be positively impacted. 60,61
Overall, though positive results of GH supplementation have been noted in many patients, there has been an inconsistency with its impact on BMD, metabolic risks, and quality of life. 62
Some studies have shown improved lipid profile after 2 years on GH therapy, whereas other studies have not shown a benefit to supplementation with GH after epiphyseal closure. 63 –66 These differences could be explained by the duration of discontinuation of GH therapy for individual studies. In those with a shorter period of discontinuation (1-month vs. 1–6 years), it is presumed that the short time during which GH may have been discontinued may not have been enough to cause metabolic changes to develop.
Based on the putative benefits of GH previously described, the suitability of each pediatric patient for adult GH therapy is an important topic. To determine the appropriate candidates for therapy, each patient receiving pediatric GH therapy must be evaluated after his/her growth plates have closed for the permanence of GHD. This is since the cause of the majority of patients diagnosed with pediatric GHD is idiopathic and they do not have permanent GHD. 67,68 This may not be surprising considering the limitations of GH provocative testing covered in this article. Patients with multiple hormonal deficiencies and those who have a genetic basis for the etiology of GHD, in addition to patients with a low IGF-1 obtained at least 1 month after the discontinuation of pediatric GH therapy, do not require additional provocative testing. 69
Once the permanence of GHD has been established, the importance of proper transitioning of pediatric patients with GHD cannot be overemphasized, since adolescence may represent a period during which patient compliance wanes and loss to follow-up may occur. Cessation of therapy may also occur due to insurance denial or an individual's lack of coverage. Physician factors, such as a hesitance to start GH therapy based on apprehension about the risk of secondary malignancies, may also affect the resumption of GH therapy in patients with permanent GHD, which could exist beyond the growing years.
At this time, the impact of GH replacement in reversing some of the metabolic effects seen in GHD is not clear and long-term studies are needed to determine whether the metabolic alterations that can be seen in CO-GHD are persistent. 19 Nonetheless, clinicians should individualize their approach to patients with CO-GHD regarding the decision to re-initiate and to continue GH supplementation in adult life. With delayed initiation, it is possible that a total amelioration of the metabolic manifestations seen in GHD may not be possible and there could be an adverse impact on the quality of life.
Conclusion
Considering the adverse metabolic outcome of some individuals with untreated GHD and its possible effects on morbidity and mortality in adulthood, clinicians should be aware of the metabolic consequences of severe GHD in untreated patients. With this awareness also comes the need to ensure that patients with GHD are appropriately transitioned to adult dosing (for which lower GH doses are required) after growth has ceased, since GH can have a crucial metabolic role well beyond the period of linear growth.
Footnotes
Acknowledgments
Author Disclosure Statement
The author declares no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The author received no financial support for the research, authorship, and/or publication of this article.