
Abstract
Background:
Metabolic syndrome (MetS), one of the most researched topics in recent years, is a metabolic disorder that presents with increased inactivity and has increasing prevalence in the developing world where many ready-made foods are consumed. This research aimed to investigate the protective effect of exercise and quercetin administration in a rat model of MetS induced by fructose.
Methods:
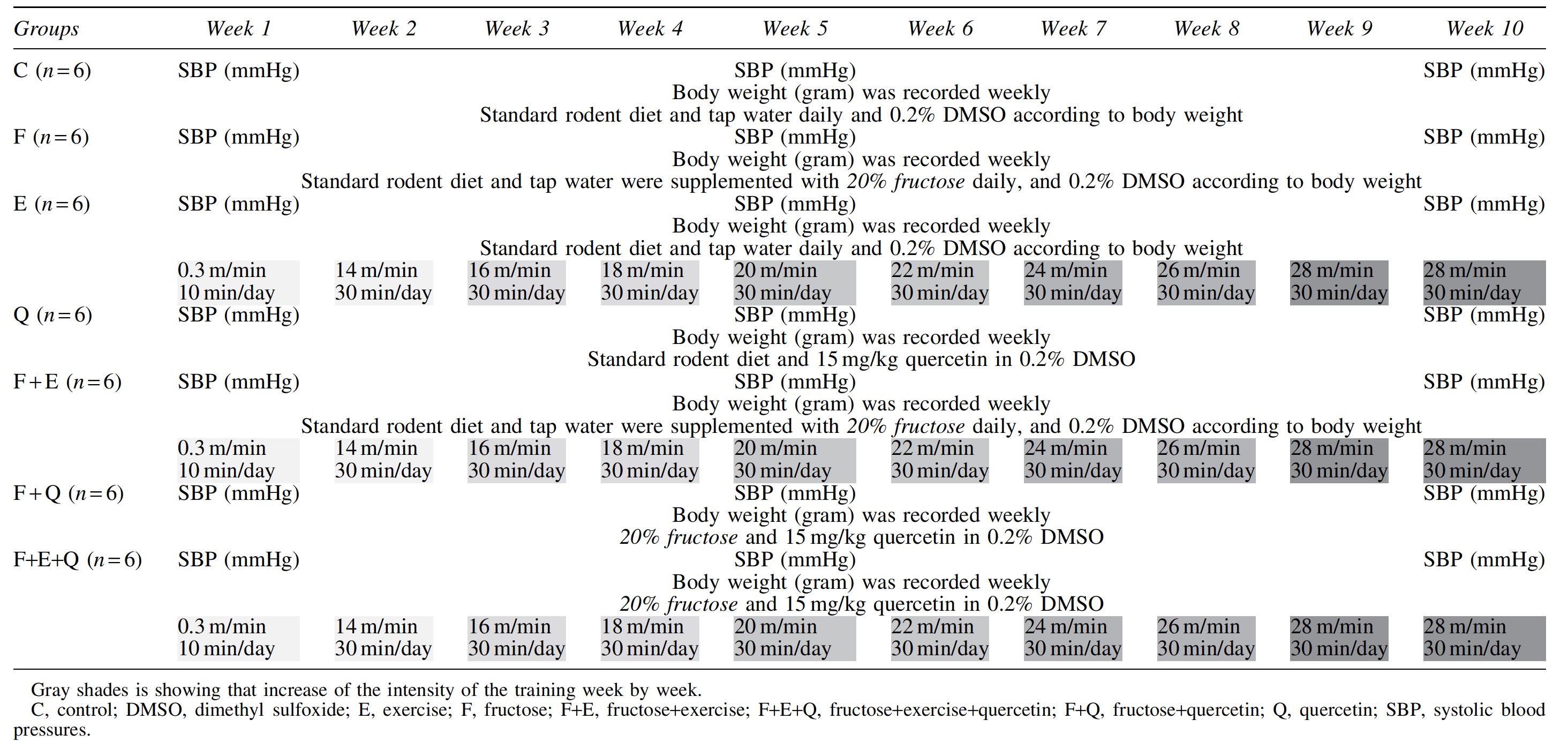
Forty-two male rats were divided into seven groups (n = 6): control (C), fructose (F), exercise (E), quercetin (Q), fructose+exercise (F+E), fructose+quercetin (F+Q), and fructose+quercetin+exercise (F+Q+E). Fructose was given as 20% solution in drinking water, and quercetin (15 mg/kg/day) was administered by oral gavage. Treadmill running exercises were applied 30 min a day for 5 days a week. After the experiments, biochemical assays, Lee index, and body fat mass analyses were measured.
Result:
Fructose administration caused a statistically significant increase in systolic blood pressures (SBP), triglycerides (TG), VLDL–cholesterol, glucose, insulin, and homeostasis model assessment of insulin resistance (HOMA-IR) compared with the control group, and the MetS model was successfully demonstrated (P < 0.05). It was determined that SBP, serum TG, serum insulin, HOMA-IR, and Lee indexes, and body fat mass, were decreased in the F + E group (P < 0.05). In addition, it was found that the MetS-related parameters improved, except lipid profile in the F + Q group (P < 0.05).
Conclusion:
These results show that high fructose consumption leads to elevated SBP, TG, cholesterol, body fat mass, glucose, insulin, and HOMA-IR levels, and aerobic exercise training treatment has beneficial effects on these biochemical parameters in rats. Although quercetin has positive effects on SBP and insulin levels, it was observed to cause a significant increase especially in TG and body fat mass. Therefore, more detailed dose studies and pathways of quercetin are needed to elucidate its mechanism of action in body fat mass.
Introduction
Metabolic syndrome (MetS) is a disease characterized by hypertension, dyslipidemia, hyperinsulinemia, and insulin resistance, and it is a severe risk factor for cardiovascular disorders, type 2 diabetics, and obesity. 1,2 The frequency of MetS is increasing all over the world, especially in developed countries. In addition to genetic factors, a sedentary lifestyle and the rapid increase in the consumption of ready-made foods, especially those that are carbohydrate based, are the main reasons for this increased prevalence. 3
Recent studies reveal that fructose included in the diet is an important factor in the development of MetS. The main source of fructose is in the form of corn syrup used as a sweetener in the production of ready-made foods. 4 Increases in insulin resistance, weight gain, glucose intolerance, hypertension, and triglycerides (TG) have been observed in animals that have been fed a fructose-rich diet. 5
Today, in line with technological developments, people's lifestyles are changing, making them less mobile. Lifestyle modifications, such as regular aerobic exercise and healthy diet, are often recommended as nondrug treatment options for MetS. 3 Researchers have confirmed that exercise is a good method to prevent MetS since it increases muscle mass, decreases body fat and body weight, controls diabetes, reduces blood pressure, and decreases general cardiovascular risk factors. 6,7 There are also various therapeutic tools, such as pharmacological agents and natural compounds, used to control MetS and obesity. 8 Studies have shown that a variety of flavonoid-containing foods, for example, many fruits, vegetables, grains, herbs, and beverages, are beneficial for the treatment and prevention of obesity and MetS. 9 Quercetin, a flavonoid found in many fruits and vegetables, is an important antioxidant. Studies have reported that quercetin lowers blood pressure, inhibits lipid peroxidation, reduces cancer risk, and accelerates metabolism. In addition, quercetin has been proven to treat various diseases and conditions, such as heart diseases, atherosclerosis, and liver fibrosis. 10,11
Some recent meta-analyses have reported the beneficial influences of quercetin administration on blood pressure. 12 A research by Mahmoud et al., as cited in Ostadmohammadi et al., in diabetic rats showed that quercetin intake reduced hyperinsulinemia, insulin resistance, inflammatory factors, blood pressure, and hyperlipidemia. 13
Cost-free lifestyle changes, such as exercise and a healthy diet, gain importance day by day in the prevention and treatment of MetS, which is rapidly increasing and considered to become an economic burden and a serious health problem in the future. The literature contains several studies examining the effects of exercise and quercetin on human health separately. 6,10,14 However, to our knowledge, there is no comprehensive similar study examining the effects of both applications on MetS components and obesity parameters. The functions of flavonoids and exercise models in MetS remain controversial, and studies investigating the functions of flavonoid subclasses modifying MetS provided inconclusive results. 15 In this study, the effects of aerobic exercise and administration of quercetin, a flavonoid, on MetS were evaluated in rats in which MetS was induced by fructose.
Materials and Methods
Chemicals
Quercetin (95%) and fructose (99%) were purchased from Sigma-Aldrich (St. Louis, MO). All the other chemicals of the highest analytical grade were purchased from Merck or Sigma-Aldrich.
Animals and experimental design
Forty-two adult male Sprague–Dawley rats weighing 225 ± 10 grams were housed at 20–24°C with a 12-hr light/12-hr dark cycle and provided with standard rat chow and tap water that were freely available. Forty-two rats were randomly divided into seven groups (n = 6) as follows:
Control (C): The rats were fed a standard rodent diet and tap water.
Fructose (F): The rats were fed a standard rodent diet, and tap water was supplemented with 20% fructose. 16
Exercise (E): The rats were fed a standard rodent diet and tap water, and treadmill running exercises were applied for 30 min every day at the same hour 5 days a week for an experimental period of 10 weeks. 17
Fructose+Exercise (F+E): Both fructose and treadmill running exercises were applied.
Quercetin (Q): The rats were fed a standard rodent diet and tap water, and quercetin was administered at a dose of 15 mg/kg body weight in 0.2% dimethyl sulfoxide (DMSO) per day by oral gavage. 18 Quercetin solution was prepared freshly every day.
Fructose+Quercetin (F+Q): Both fructose and quercetin were applied.
Fructose+Exercise+Quercetin (F+E+Q): The rats were fed a standard rodent diet and fructose was given. Treadmill exercises were applied as in the exercise group, and the rats were also administered quercetin.
Since dimethyl sulfoxide was used as a vehicle for quercetin, the control and fructose groups received 0.2% DMSO, proportional to their body weight (Table 1). The experiment was carried out for 10 weeks, after which, the rats were sacrificed under anesthesia induced with ketamine (30 mg/kg body weight) and xylazine (6 mg/kg body weight). Blood samples for laboratory assays were drawn intracardiacally, and the sera were separated by centrifugation and stored at −80°C until analysis.
Animals and Experimental Design
Exercise training protocols
The rats were trained on a treadmill for 30 min/day for 5 days a week for 10 weeks. The speed was started at 14 m/min and increased by 2 m/min every minute, until a maximum speed of 28 m/min was reached. The exercise protocol was prepared by modifying Sebaı et al.'s treadmill exercise protocol. 17 We used the maximal exercise test (∼60% to 85%). This protocol received approval from the University of Gazi Animal Use and Care Committee. The rats were exercised in a temperature- and humidity-controlled (22°C and 55%, respectively) room using an EGAL Instruments (RT-02) treadmill.
Measurement of systolic blood pressures and body weight
Body weights were recorded weekly and systolic blood pressures (SBP) were measured with the tail-cuff method at the beginning of the study, at the end of week 5, and at the end of week 10. All animals were preconditioned for blood pressure measurements 1 week before each experiment. At least seven measurements were undertaken in every session, and the mean of the lowest three values within 5 mmHg was recorded as the SBP value. All SBP measurements were made between 10 a.m. and 1 p.m. 4
Biochemical assays
Serum glucose, TG, total cholesterol (total-c), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and very low-density lipoprotein cholesterol (VLDL-C) cholesterol levels were measured by enzymatic methods using autoanalyzers. The serum insulin level was estimated with a commercially available ELISA kit (Millipore, Billerica, MA). The homeostasis model assessment of insulin resistance (HOMA-IR) index was calculated using the following formula: [insulin (mU/L) glucose (mmol/L)]/22.5. 4
Lee index analysis
Lee's obesity index was calculated as follows: body mass1/3(gram)/nasal-anal length (cm) × 10. The rats with a value equal to or lower than 30 grams/cm was classified as having normal weight, and those with a value higher than 30 grams/cm were classified as obese. 19
Body fat mass analyses
Abdominal subcutaneous fat mass (SFM), visceral fat mass (VFM) (mesenteric, epididymal, and retroperitoneal), and hind limb skeletal-muscle mass (H.L.S.M-gastrocnemius, soleus, plantaris, and extensor digitorum longus) were removed from each animal. 20 The tissues were weighed after dissection and separation from vessels and other connective tissues.
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics v. 24 (SPSS, Inc., Chicago, IL). The Kolmogorov–Smirnov test was used to determine whether the distributions of continuous variables were normal. Since the study groups did not show a normal distribution according to the Kruskal–Wallis test, the comparisons between the groups were undertaken using the Mann–Whitney U test. More than two measurements in a single group, the Friedman test was used to determine change over time. Probability values of less 0.05 were accepted as significant.
Results
Summary of the effects of exercise and quercetin administration on metabolic syndrome were shown in Fig. 1.

Summary of the effects of exercise and quercetin administration on metabolic syndrome.
The body weights and SBP of the rats are shown in Table 2. The body weights and SBP values of the F group were higher compared with the C group (P < 0.05, P = 0.035; P = 0.006). In comparison with the F group, E and Q administration significantly reduced SBP in the F + E and F + Q groups (P < 0.05, P = 0.006).
Body Weights and Systolic Blood Pressures
All results are expressed as mean ± SD.
P < 0.05. Compared with the control group.
P < 0.05. Compared with the fructose group.
P < 0.05. Compared with the exercise group.
P < 0.05. Compared with the quercetin group.
P < 0.05. Compared with the fructose plus exercise group.
P < 0.05. Compared with the fructose plus quercetin group.
P < 0.05. Compared with the initial values.
P < 0.05. Systolic blood pressure compared with fourth week values.
SD, standard deviation.
The Lee index values of the groups are shown in Fig. 2. The higher Lee index of the F group was significantly reduced by E and Q treatment (P < 0.05, P = 0.016; P = 0.047). The values of the F + E and F + Q groups were found to be significantly lower than those of the Q group (P < 0.05, P = 0.006; P = 0.010).
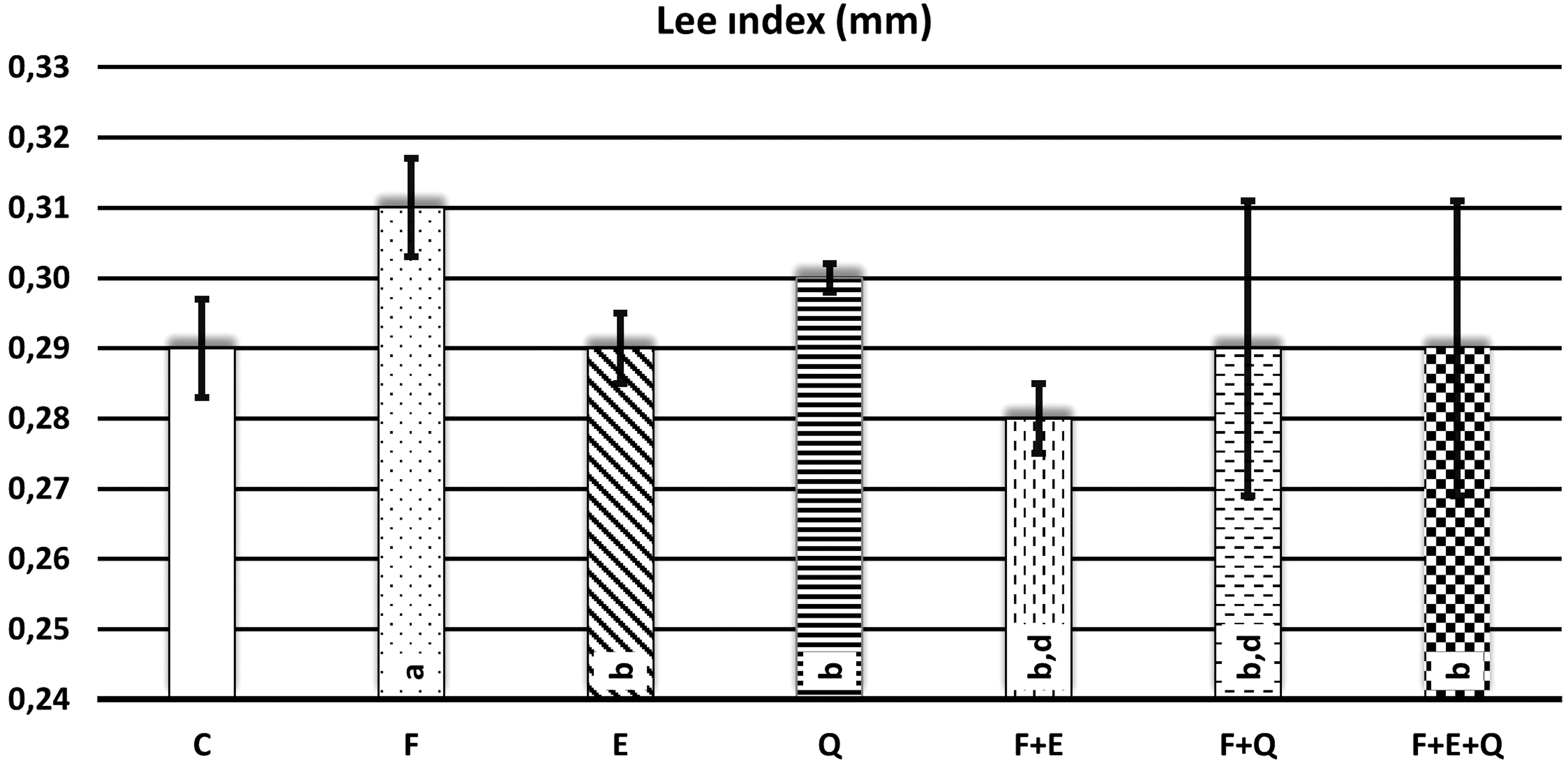
Lee index profile. Data represented as mean ± SD. Forty-two male rats, each group included six rats. *P < 0.05. (a P < 0.05. Compared with the control group, b P < 0.05. Compared with the fructose group, c P < 0.05. Compared with the exercise group, d P < 0.05. Compared with the quercetin group, e P < 0.05. Compared with the fructose plus exercise group, f P < 0.05. Compared with the fructose plus quercetin group). C, control; E, exercise; F, fructose; F+E, fructose+exercise; F+E+Q, fructose+exercise+quercetin; F+Q, fructose+quercetin; Q, quercetin.
Abdominal SFM and VFM were also significantly greater in the F group compared with the C group (P = 0.006). The VFM of the F + E group was lower compared with the F group (P = 0.006); however, it did not significantly differ between the F + Q and the F groups (P = 0.361). Furthermore, the VFM of the F + Q group was higher compared with the F + E group (P = 0.016) (Fig. 3).

Body fat masses. Data represented as mean ± SD. Forty-two male rats, each group included six rats. *P < 0.05. (a P < 0.05. Compared with the control group, b P < 0.05. Compared with the fructose group, c P < 0.05. Compared with the exercise group, d P < 0.05. Compared with the quercetin group, e P < 0.05. Compared with the fructose plus exercise group, f P < 0.05. Compared with the fructose plus quercetin group).
Muscle weights, a combination of gastrocnemius, soleus, plantaris, and extensor digitorum longus muscles of the hind limb, are shown in Fig. 4. The muscle weights (sum of gastrocnemius, soleus, plantaris, extensor digitorum longus) of the F and E groups were higher compared with the C group (P < 0.05, P = 0.045; P = 0.011), while the hind limb muscle weight was higher in the E group than in the Q and F + Q groups (P < 0.05, P = 0.009; P = 0.01). Furthermore, the muscle weight of the E group was higher compared with the F group; however, this was not statistically significant (P > 0.05, P = 0.347)

Skeletal muscle masses. Data represented as mean ± SD. Forty-two male rats, each group included six rats. *P < 0.05. (a P < 0.05. Compared with the control group, b P < 0.05. Compared with the fructose group, c P < 0.05. Compared with the exercise group, d P < 0.05. Compared with the quercetin group, e P < 0.05. Compared with the fructose plus exercise group, f P < 0.05. Compared with the fructose plus quercetin group).
Table 3 shows the serum lipid profiles of the groups. Compared with the C group, the F group showed a significant increase in serum TG and VLDL-C levels (P < 0.05). The serum TG, TC, LDL-C, and VLDL-C levels of the F + E group were lower than that of the F group (P < 0.05 P = 0.009; P = 0.018; P = 0.017; P = 0.017), and the HDL-C level of the F + E group was higher than that of the F group (P < 0.05 P = 0.006). When the F group and F + Q were compared, quercetin administration reduced total and LDL-C to control levels in the F + Q group. The TG and VLDL cholesterol levels of the F+E+Q groups were significantly elevated compared with the F group (P < 0.05, P = 0.009)
Serum Lipid Profile
All results are expressed as mean ± SD.
P < 0.05. Compared with the control group.
P < 0.05. Compared with the fructose group.
P < 0.05. Compared with the exercise group.
P < 0.05. Compared with the quercetin group.
P < 0.05. Compared with the fructose plus exercise group.
P < 0.05. Compared with the fructose plus quercetin group.
HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TG, triglyceride; total-c, total cholesterol; VLDL-C, very low-density lipoprotein cholesterol.
As shown in Table 4, the serum glucose and insulin levels and HOMA-IR indexes of the F group were significantly higher compared with the C group (P < 0.05, P = 0.006). Compared with the F group, the serum glucose and insulin levels and HOMA-IR indexes were significantly lower in the F + E group (P < 0.05, P = 0.006). The serum insulin levels of the F + Q and F+E+Q groups were lower than the fructose group (P < 0.05, P = 0.006; P = 0.009).
Serum Glucose, Insulin Levels, and Homeostasis Model Assessment of Insulin Resistance Levels
All results are expressed as mean ± SD.
P < 0.05. Compared with the control group.
P < 0.05. Compared with the fructose group.
P < 0.05. Compared with the exercise group.
P < 0.05. Compared with the quercetin group.
P < 0.05. Compared with the fructose plus exercise group.
P < 0.05. Compared with the fructose plus quercetin group.
HOMA-IR, homeostasis model assessment of insulin resistance.
Discussion
In the present study, 20% fructose was added to the drinking water of the rats for 10 weeks and the MetS criteria were evaluated. At the end of the study, fructose induced hypertension, hyperinsulinemia, insulin resistance, and hypertriglyceridemia in which MetS criteria were observed compared with the C group (P < 0.05). Our findings are in agreement with those reported by Kantar et al., Zhang et al., Dupas et al., and Mamikutty et al., who all reported that 20% fructose-fed rats had significantly increased SBP, plasma TG, plasma glucose, and plasma insulin levels and an elevated HOMA-IR index. 4,5,8,21
Studies highlight the importance of nutritional regulation and increased physical activity in the treatment and prevention of MetS. 3 –20 For this purpose, we investigated the preventive role of aerobic exercise and quercetin administration on MetS after creating an MetS model and evaluating it with its criteria.
In our study, similar to the literature, fructose administration was found to cause a significant increase in the body weight of the animals (P < 0.05). 2 –15 It was observed that exercise accompanied by fructose administration reduced this increase in body weight, while quercetin did not affect body weight and even had similar activity to fructose, resulting in increased body weight; however, these moderations did not reach statistical significance. In experimental and clinical studies, researchers have examined the effect of regular exercise on metabolic diseases, obesity, diabetes, and cardiovascular diseases, and noted that fructose administration causes an increase in body weight and different exercise practices significantly reduce body weight and improve body composition. 7,20,22 On the contrary, in our study, similar to the literature, 11 quercetin did not have a significant effect on body weight, which can be attributed to the low dose used. In this respect, there is a need for further comparative studies investigating the effect of different doses.
Our study and other experimental animal models demonstrated an association between fructose consumption and hypertension. 4,5,23 In our study, exercise and quercetin administration reduced hypertension, but it was observed that this effect was higher in the long-term aerobic exercise application than quercetin (P < 0.05). Exercise is an effective treatment method for the prevention and control of hypertension. 24,25 Researchers have reported that regular exercise lowers blood pressure by increasing baroreflex sensitivity, and similarly triggers angiogenesis, dilating the capillary network and preventing cardiac hypertrophy. 26 Similarly, studies consistent with our results suggest that quercetin administration reduces hypertension and this antihypertensive effect is positively associated with the activity of quercetin in endothelial disorders. 10,11
Obesity, notably abdominal obesity, is the most important factor increasing MetS and cardiovascular risks. 27 In our study, the Lee index, SFM, and VFM, which are frequently used in the diagnosis and evaluation of obesity, were examined and the values of F group were higher than the C group (P < 0.05). Other studies also reported that the Lee index, SFM, and VFM were increased in rats given a high-fructose and high-fat diet. 10,14,16,21,28 We also observed that exercise application accompanied by fructose decreased the Lee index, SFM, and VFM values, while quercetin administration in the presence of fructose significantly decreased the Lee index value only, with SFM and VFM being slightly affected at a nonsignificant level. The Lee index, SFM, and VFM values of the F+E+Q group were statistically significantly decreased compared with the F group, which can be attributed to the effect of exercise. This change can be explained by exercise increasing the lipid oxidative capacity of skeletal muscles, resulting in an improvement in the whole-body fat oxidation rate. 29 Similar to the results of our study, previous researchers have reported the positive effects of physical activity on lipid parameters and noted that the Lee index, fat mass percentage, fat mass, VFM, and SFM values were effectively reduced by exercise. 14,19,20 However, studies examining the effect of quercetin on body weight and fat mass present conflicting results. On the one hand, there are researchers showing that quercetin administration decreases the Lee index values and epididymal, retroperitoneal, and perirenal adipose tissue of mice, 30,31 which is consistent with our findings; on the other hand, a human study found no changes in adipose tissue-associated inflammatory markers. 32 In another study similar to ours, there was no significant reduction in the body weight and adipose tissue size of animals as a result of the administration of 15 mg/kg quercetin. 33 These conflicting data on quercetin may be related to the differences in the dose used, route of administration, and duration of supplementation. 32,34 In our study, it was observed that Lee index parameters in the F + E and F + Q groups were found to be significantly lower than those of the Q group (P < 0.05). Researchers found that quercetin reduced liver fat, but there was no significant difference in body mass parameter. Similar to our results, they found the body mass of the quercetin group to be higher than the high-fructose, high-cholesterol diet, with or without quercetin; however, this was not statistically significant. 35 There is a need for studies in the literature on the interaction of fructose and quercetin and their effects on metabolism. In our study, the reason why quercetin administration did not affect body fat mass like exercise may be associated with the activation of fat metabolism by this flavonoid. More detailed dose studies and pathways or cell culture analyses of quercetin are needed to elucidate its mechanism of action in body fat mass.
In individuals with MetS, lipid accumulation in skeletal muscles accompanying body fat mass reveals serious impairments in lipid metabolism. 20 As stated in the Materials and Methods section, when measuring the absolute level of body fat mass values of the animals, we also removed and weighed the H.L.S.M. The values of the F and E groups were higher than those of the C group, and the values of the Q and F + Q groups were found to be statistically significantly lower compared with the exercise group (P < 0.05). The increase in hind limb muscle mass with the effect of fructose can be explained by the decrease in glucose oxidation, glucose uptake, and glycogen synthesis in muscles mediated by insulin resistance, as well as the increase in muscle fat accumulation as a result of inhibition of carbohydrate-fat conversion. 36 In our study, it was observed that quercetin administered together with fructose reduced the muscle mass increasing effect of the latter due to inflammation. In another study consistent with our results, it was reported that a fructose diet caused inflammation in the skeletal muscles and increased muscle mass and muscle fiber size with macrophage accumulation, while quercetin administration inhibited this process by reducing inflammation, increasing muscle oxygenation, and reducing fat accumulation. 37 This is in line with our study, in which muscle mass development was mostly observed in the exercise group, which can be explained by exercise increasing the ability of muscle tissue to take up and oxidize unesterified fatty acids as the oxidative capacity of the muscle increases, that is, growth of lean tissue in the muscle (hypertrophy). 28 This idea is supported by a study of Herbert et al., who investigated the atrophic response and associated adaptations of the soleus and medial gastrocnemius muscles to an exercise program and reported that exercising the hind limb muscles was effective in reducing atrophy. 38
Unlike glucose, in fructose metabolism, due to the phosphofructokinase enzyme, fructose directly enters the glycolytic pathway without glycolysis and cannot be regulated by insulin. Since fructose cannot be regulated at this stage, it causes glycolysis products to be produced in excess, thus increasing the synthesis of fatty acids. Increased fatty acid synthesis can increase circulating fatty acids and stored fat. 36 In our study, in the fructose-mediated MetS model, the amount of TG increased with the effect of fructose, which is consistent with the results of Mamikutty et al. and Abo-Youssef. 9 –21 Researchers have reported that exercise improves lipid metabolism by increasing the lipid oxidation capacity in skeletal muscles. 29 Our study and other experimental animal models demonstrated an association between exercise and TG levels. 7,22,26 It is reported that treatment with exercise administration significantly lowers TG levels. However, in our study, we determined that quercetin administration increased the TG level acting like fructose, with the TG values of the F+E+Q group being considerably higher compared with all the remaining groups. This serious increase in the TG level can be considered a synergistic increase due to fructose and quercetin and is not related to exercise. We suggest that quercetin increases the lipid level more strongly than exercise through the pathways in which the lipid synthesis is activated, without the strong oxidization of lipid particles emerging through fructose. Thus, exercise may be unable to inhibit lipid synthesis or break down lipids caused by fructose and quercetin. Parallel to our study, other researchers have reported that quercetin use did not lead to a decrease in body weight, blood lipids, and lipid indices. 10,39
Hyperlipidemia and hypercholesterolemia have been reported as major risk factors for the cardiovascular complications of atherosclerosis and myocardial infarction. 40 We attempted to further support our results by measuring the amount of total-c, HDL-C, LDL-C and VLDL-C, which are not included in the MetS diagnostic criteria but constitute an important lipid profile.
In our fructose-mediated MetS model, only VLDL-C was significantly increased among the cholesterol parameters, and similar to other experimental animal models, 4,15 we demonstrated an association between fructose consumption and high plasma VLDL-C levels. In addition, we determined that exercise application reduced total-c, LDL-C, and VLDL-C, and increased HDL-C, which is in agreement with the results of Ha et al. and Coll-Risco et al. 6,7 This has been previously explained by exercise increasing the consumption of fatty acids and lipoprotein lipase enzyme activity in muscle tissue. 41 On the contrary, we observed that quercetin administration reduced total-c and LDL-C, but had no effect on HDL-C and VLDL-C. As in the case of TG, a significant increase was detected in the VLDL-C value of the fructose+exercise+quercetin group, and there was also a statistically significant increase in the HDL-C of this group. The literature contains no study examining the effect of quercetin administration on total-c, HDL-C, LDL-C, and VLDL-C at a dose and for a duration similar to our study. We consider that this effect of quercetin may be due to its synergistic effect with fructose and its role in increasing general lipid synthesis. 10,39,40
In our study, it was observed that the blood insulin, glucose, and insulin resistance (HOMA-IR) parameters were increased in the fructose-mediated MetS model (P < 0.05). These parameters are among the important criteria of MetS and have been reported to significantly change in similar models in the literature. 5,16,23,33 In the model we created, we determined that exercise reduced blood glucose and insulin levels and had a positive effect on insulin resistance. In studies conducted to date, researchers have reported that acute and chronic physical activity applied in the prevention and treatment of MetS improves insulin resistance, and this has been explained by the increase in glucose uptake into the cell in the skeletal muscles due to the increase in insulin signals in response to muscle contraction with exercise. 28,41 Exercise also increases insulin sensitivity while stimulating GLUT-4 receptors on the cell surface, which is not dependent on insulin, increasing glucose permeability of the membrane and decreasing insulin resistance. 33,41 That is, exercise improves glycemic control, particularly in patients with type 2 diabetes as muscle contraction acts like insulin in glucose transfer from plasma to cell. 25 Quercetin supplementation downregulates gluconeogenesis enzymes via an insulin-dependent pathway and may result in decreased glucose production and thus exhibit antidiabetic properties. However, in the literature, studies on the effect of quercetin on glucose, insulin, and HOMA also have conflicting results. 9,13,18,42 These conflicting data on quercetin may be related to the differences in the study design of quercetin, differences in the dose used, and type of quercetin used as only quercetin or combined quercetin with other nutrients. 13 In our study, although not statistically significant, quercetin administration further increased the glucose level, which was already elevated due to the effect of fructose, leading to the reduction of the amount of insulin and insulin resistance This increase in the blood glucose level may be due to the quercetin-induced rise in liver gluconeogenic enzyme activities and increased expiration. We can also explain the positive effect of quercetin on the insulin amount and insulin resistance with its activity in increasing glucose influenza in muscle and adipose tissue, resulting in elevated insulin-mediated lipid synthesis. 43
Conclusion
As a result, we induced MetS in rats with 20% fructose supplementation via drinking water for 10 weeks, which led to an increase in SBP, serum TG, serum insulin, and insulin resistance, and investigated the effect of exercise and quercetin. Both aerobic exercise training and quercetin administration can be used in the treatment for MetS prevention. Both aerobic exercise training and quercetin application can be used as a treatment method for the prevention of MetS parameters. Although quercetin has partial positive effects on MetS, it was observed to cause a significant increase especially in TG and body fat mass. Therefore, it is considered that aerobic exercise alone is a preventive method for MetS and can be applied as a beneficial treatment. In addition, aerobic exercise training has been proven to be very beneficial for individuals with MetS by improving the Lee index, blood TG, and HDL-C. Considering cell damage caused by MetS and the mechanism of action of this syndrome, there is a need for further comprehensive and large-scale studies taking into account the dose-dependent effects of antioxidant molecules, such as quercetin along with exercise applications.
Ethical Approval
This study was conducted in accordance with regulations of the Animal Experimentation Ethics Committee of Gazi University (G.Ü.ET-13.012).
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
The study was supported by the Scientific Research and Project unit of Gazi University, coded 20/2015-01.