
Abstract
Background:
The effect of diabetic polyneuropathy (DPN) and autonomic neuropathy (AN) on bone turnover in type 2 diabetes mellitus (DM) is uncertain due to the lack of data. In this study, we tried to determine the effect of DPN and AN on bone metabolism.
Materials and Methods:
The study included patients with type 2 DM (aged 18–80 years) and age-matched healthy individuals who presented to the Departments of Metabolism and Diabetes, Geriatrics, and General Internal Medicine, Cerrahpaşa Medical School, Istanbul University. The patients were examined to find out whether they had AN, and neuropathy scores were recorded by exploring peripheral neuropathy. Bone mineral density was measured by dual-energy X-ray (DXA). Demographic characteristics, the presence of microvascular complications, and biochemical data were obtained from patients' files. Serum cross-linked C-telopeptide (Ctx), osteocalcin, and bone-specific alkaline phosphatase (B-ALP) were analyzed.
Results:
The study comprised a total of 64 patients: 23 had type 2 DM and osteoporosis (OP) (duration of diabetes 10.1 ± 7 years; mean age 63 ± 9.1 years; female/male 18/5; Group 1), 41 had type 2 DM and non-OP (duration of diabetes 10.3 ± 7.6 years; mean age 58 ± 7.4 years; female/male 30/11; Group 2), and 26 healthy volunteers made up the control group (mean age 62 ± 11.9 years; female/male 14/12; Group 3). The bone turnover parameters were lower in type 2 DM individuals. The levels of osteocalcin (13.3 ± 5.2 ng/mL) and B-ALP (44.7 ± 10.9 IU/L) in patients with type 2 DM were lower than those of healthy subjects: osteocalcin (20.6 ± 10 ng/mL) and B-ALP (111 ± 31.4 IU/L; P = 0.001 and P = 0.000, respectively). Ctx levels (193.5 ± 49.3; 207.6 ± 40 ng/mL) were recorded to be similar (P = 0.2). AN was also noted as a risk factor for OP. For patients without AN, the likelihood of developing OP (odds ratio) was 0.7. The corresponding ratio for patients with AN was 9.3.
Conclusions:
Among the independent variables, the neuropathy score was determined to have an impact on bone turnover. AN was identified to be a significant risk factor for OP.
Introduction
Diabetic polyneuropathy (DPN) is one of the most commonly encountered microvascular complications of diabetes. 1 –7 The prevalence of DPN seen in 10%–15% of patients at the time of diagnosis shows an increase that parallels the patient's age at onset of type 2 diabetes mellitus (DM) and his or her level of glycemic control. 8 –14 The role of DPN in bone pathology and fracture risk has not yet been clearly examined. It is known that autonomic neuropathy (AN) is a component of DPN and its consequence, autosympathectomy, triggers the development of neuro-osteoarthropathy in both feet. This complication is characterized by accelerated bone turnover and increased osteoclastic activity. The control of osteoclastic activity through bisphosphonates offers benefits in the disease that (when left untreated) leads to multiple fractures and Charcot foot. 15,16 The DPN impact on the skeletal system is not confined to the lower extremities. Studies have reported that in DPN, bone metabolism is negatively affected by the decrease in peptides secreted from nerve cells. 17 However, data on the association of this complication with bone mineral density loss, osteoporosis (OP), and fracture risk are inconclusive and controversial. 18
Bone is a tissue with many nerves and blood vessels. The central and peripheral nervous systems play an important role in bone turnover by releasing neurotransmitters and neuropeptides. These neuropeptides, which include the calcitonin gene-related peptide (CGRP), substance P (SP), vasoactive intestinal peptide (VIP), and N-methyl-D-aspartate (NMDA), have receptors on all bone surfaces and affect bone remodeling. 19 In a study in 2012 conducted by Wang et al. on mice, it was shown that by employing the method of quantitative polymerase chain reaction in cardiac AN, reduction occurred in the tyrosine hydroxylase (TH) expression and also in the level of norepinephrine (NE) in the left ventricle. These findings suggest that changes in cell signaling and function due to AN may affect bones as well as the heart. 20
We hypothesize that contrary to what is known in patients with type 2 DM, we expect a decreased bone turnover in those with DPN. We expect that neuropathy predicts that too, as it is more evident in those with neuropathy.
This study sought to investigate the associations of type 2 DM, DPN, and AN, which is a component of DPN with OP in individuals who were followed for type 2 DM and diagnosed with OP.
Materials and Methods
Patient selection
Between October 2010 and June 2016, of the 7200 patients, 90 subjects aged 18–80 years met the study criteria and were admitted to the outpatient section of the Department of Diabetes of the Cerrahpaşa Medical School at Istanbul University. A suitable sample is used in our study. According to the type 2 DM diagnostic criteria of the American Diabetes Association and OP diagnostic criteria of the World Health Organization (WHO), 90 of the 7200 applications of patients with type 2 DM and/or OP and 26 healthy volunteers were accepted to be suitable for our study. 21,22 Group 1 included 23 patients diagnosed with diabetes and OP; Group 2 comprised 41 patients diagnosed with diabetes without OP; and Group 3 consisted of 26 healthy volunteers who did not have any illness and applied to the general internal medicine outpatient clinic for health checks.
Exclusion criteria
Patients with any known diseases affecting bone metabolism were excluded, including type 1 DM; hyper/hypothyroidism; hyper/hypoparathyroidism; Cushing's syndrome; hypogonadism; chronic renal failure; chronic liver disease; hematologic diseases; rheumatologic diseases; inflammatory bowel disease; diseases causing malabsorption; Paget's disease; D hypervitaminosis; genetic diseases (Ehlers–Danlos disease and Marfan syndrome, etc.); regular alcohol and cigarette consumers; patients receiving any treatment for osteoporosis; patients receiving treatment with corticosteroids, thyroid hormone, coumadin, heparin, antiepileptic drugs, methotrexate, or cyclosporine or those undergoing hormone replacement therapy; patients who underwent organ transplantation for any reason; those who were pregnant; and patients with bone fracture or osteopenia.
Informed consent for the protocol for sample collection was approved by the Cerrahpasa Medicine Faculty Ethics Committee of Istanbul University and was carried out according to the requirements of the Declaration of Helsinki. All patients were fully informed of the study procedures before they gave their consent.
Study design
The duration of fertility; presence of type 2 DM and its duration and type 2 DM complications; presence of hyperlipidemia; insulin use; and presence of hypertension and ischemic heart disease were recorded according to the statements of patients. Measurements of height, weight, body mass index (BMI), pulse rate, and arterial blood pressure were performed, followed by a neurological examination for neuropathy. The neuropathy test is used in our study because of its high sensitivity for diagnosis of DPN. 23
Distal symmetric polyneuropathy assessment
During the peripheral neuropathy examination, vibration sensation was tested with a 128-Hz tuning fork on both feet. A 10-gram monofilament was used when screening the feet of those with diabetes; two cups filled with hot and cold water were used to confirm heat/cold discrimination, and a pinprick test was performed with a needle. In addition, the Achilles reflex was evaluated. Each pathological condition was assigned a score of 1, and the total neuropathy disability score (NDS) was calculated on a scale of 10 points. 24 –29
AN assessment
The patients' resting heart rates were analyzed for AN; >100 bpm was considered abnormal. Arterial blood pressure was measured in both supine and upright positions at 2 min. Orthostatic hypotension was defined as a decrease of 20 mmHg in the systolic blood pressure and/or a decrease of 10 mmHg in the diastolic blood pressure and was regarded as a sign of AN. Patients who did not report episodes of hypoglycemia the night before underwent an electrocardiogram (ECG) at least 20 min after resting. Frank lead ECGs were recorded according to the following sequence:
Record 1—once in the normal supine position,
Record 2—six times in deep inspiration,
Record 3—six times in deep expiration,
Record 4—once while holding the breath, and
Record 5—once in the upright position.
The R-R interval rates were assessed according to age, and the presence of AN was then assessed. 16,30 AN was accepted if one or more of these findings were recorded as 1. The situation without findings was evaluated as 0.
Diabetic retinopathy assessment
The retinopathy evaluation of patients was performed by an ophthalmologist. The presence of retinopathy was recorded as 1 and absence as 0.
Diabetic nephropathy assessment
Patients with a glomerular filtration rate of 90 mL/min and above were included in the study. Patients with a microalbuminuria level of 30 mg/day and above were considered to have nephropathy. The presence of nephropathy was recorded as 1 and absence as 0.
Type 2 DM assessment
The American Diabetes Association criteria for the diagnosis of diabetes are any of the following: a glycosylated hemoglobin (HbA1c) level of 6.5% or higher—the test should be performed in a laboratory using a method that is certified by the National Glycohemoglobin Standardization Program (NGSP) and standardized or traceable to the Diabetes Control and Complications Trial (DCCT) reference assay; or a fasting plasma glucose (FBG) level of 126 mg/dL or higher—fasting is defined as no caloric intake for at least 8 hr; or a 2-hr plasma glucose level of 200 mg/dL or higher during a 75-gram oral glucose tolerance test (OGTT); or a random plasma glucose of 200 mg/dL or higher in a patient with classic symptoms of hyperglycemia (i.e., polyuria, polydipsia, polyphagia, and weight loss) or hyperglycemic crisis. 21
For biochemical measurements and values, peripheral venous blood samples were taken after at least 8 hr of fasting. The samples were centrifuged at 3600 rpm for 10 min and stored at −70°C. Osteocalcin (Epitope Diagnostics, Inc.), bone-specific alkaline phosphatase (B-ALP; Eastbiopharm), and cross-linked C-telopeptide (Ctx; Eastbiopharm) were measured in the stored serum samples.
OP assessment
Bone mineral density values
T scores (grams/cm2) of the lumbar spine (L1–L4), spine, femoral neck, trochanter, intertrochanter, and Ward's triangle were obtained from the files of patients who underwent measurements by dual-energy X-ray (DXA) within 1 month. The patients were divided into two groups—those with and without OP, according to the criteria established by the WHO.
In postmenopausal women, and in men aged more than 50 years, the WHO defines OP in the femoral neck and L₁–L₄ vertebrae as follows: normal for a T-score of −1 and above, osteopenia for a T-score of between −1 and −2.5, OP for a T-score of ≤−2.5, and severe OP for a T-score of −2.5 and below with history of a fracture. 22 Both the femur and lumbar region T-scores of patients were used in the evaluation.
Statistics
Statistical analysis was performed with the Windows 20 version of the SPSS software. The one-sample Kolmogorov–Smirnov test was used to check whether data were normally distributed. After determining the normal distribution, an independent samples t test was used to compare normally distributed data, and the Mann–Whitney U and Kruskal–Wallis tests were used to compare non-normally distributed data. Correlations between OP and independent variables were assessed by the Spearman test because the data were not normally distributed. Multiple logistic regression analysis was performed to assess the independent variables' association with OP. Odds ratio was calculated using logistic regression analysis. Multiple linear regression analysis was implemented to assess the independent variables' association with the bone turnover markers. The chi-squared test was used to compare proportions. P < 0.05 values were considered to be statistically significant.
Sample size
The required sample size was calculated as 74 for the two-tailed t test with a 5% significance level to achieve 80% power.
Findings
The study comprised a total of 90 patients: Group 1 included 23 patients diagnosed with type 2 DM and OP (duration of diabetes 10.1 ± 7 years; mean age 63 ± 9.1 years; female/male 18/5), Group 2 comprised 41 patients with type 2 DM and without OP (duration of diabetes 10.3 ± 7.6 years; mean age 58 ± 7.4 years; female/male 30/11), and Group 3 consisted of 26 healthy volunteers (mean age 62 ± 11.9 years; female/male 14/12).
The demographic and clinical characteristics and laboratory results of the groups are given in Table 1.
Demographic and Clinical Characteristics and Laboratory Results of Groups
Group 1: patients with diagnoses of type 2 diabetes and osteoporosis. Group 2: patients diagnosed with type 2 diabetes. Group 3: healthy volunteers. AN prevalence Group 1; Group 2 (one-sided P = 0.04, two-sided P = 0.06). Nephropathy prevalence Group 1; Group 2 (P = 0.1). Neuropathy score Group 1; Group 2 (P = 0.9). Retinopathy prevalence Group 1; Group 2 (P = 0.5). Evaluation was performed for all three groups. P < 0.05 was considered significant.
AN, autonomic neuropathy; B-ALP, bone-specific alkaline phosphatase; BMI, body mass index; Ctx, cross-linked C-telopeptide; F, female; FBG, fasting plasma glucose; HbA1c, glycosylated hemoglobin; HDL, high-density lipoprotein; M, male; PG, postprandial glucose; TG, triglycerides.
The demographic and clinical characteristics and laboratory results of the patients according to AN and DPN are given in Tables 2 and 3.
Demographic and Clinical and Laboratory Characteristics of Patients Classified According to Diabetic Polyneuropathy
P < 0.05 was considered significant.
DPN, diabetic polyneuropathy.
Demographic and Clinical Characteristics and Laboratory Results of Patients Classified According to Autonomic Neuropathy
P < 0.05 was considered significant.
Bone turnover parameters
Among the independent variables, gender, age, smoking, alcohol, BMI, AN, neuropathy score, nephropathy, duration of diabetes, duration of hypertension, and 25(OH) vitamin D, the neuropathy score was significantly related to values of osteocalcin (R 2 = −0.29, P = 0.008), Ctx (R 2 = −0.22, P = 0.037), and B-ALP (R 2 = −0.54, P = 0.000) (See Fig. 1). The BMI (R 2 = −0.3, P = 0.000) and smoking (R 2 = −0.24, P = 0.002) had important negative effects on B-ALP, while age (R 2 = 0.25, P = 0.021) had a positive effect on osteocalcin.
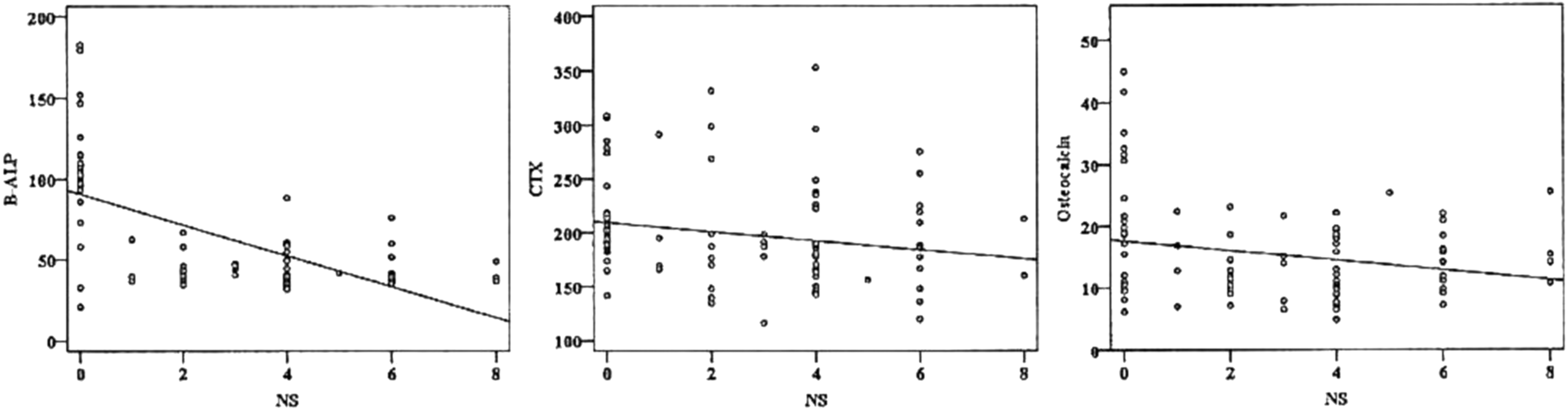
The effect of neuropathy score on bone turnover.
The levels of osteocalcin (13.3 ± 5.2 ng/mL) and B-ALP (44.7 ± 10.9 IU/L) in patients with type 2 DM were lower than those of healthy subjects: osteocalcin (20.6 ± 10 ng/mL) and B-ALP (111 ± 31.4 IU/L) (P = 0.001 and P = 0.000, respectively). Ctx levels (193.5 ± 49.3; 207.6 ± 40 ng/mL) were recorded as similar (P = 0.2) (Table 1).
The osteocalcin (13 ± 5.1 ng/mL), B-ALP (43.2 ± 9 IU/L), and Ctx (191.7 ± 42.6 ng/mL) levels in Group 1 were observed to be similar to those of Group 2, where the osteocalcin level was 13.5 ± 5.2 ng/mL, B-ALP level was 46.2 ± 12.8 IU/L, and Ctx level was 195.3 ± 56 ng/mL (Table 1).
Effect of AN on bone turnover
Based on a multiple logistic regression analysis where independent variables were gender, age, BMI, smoking, alcohol, duration of diabetes, duration of hypertension, duration of insulin use, nephropathy, neuropathy score, HbA1c, and 25(OH) vitamin D, we found that AN (R 2 = 0.25, P = 0.002, Nagelkerke R 2 = 0.245) had an effect on OP. For patients without AN, the likelihood of developing OP (odds ratio) was 0.7. The corresponding ratio for patients with AN was 9.3.
Osteoporosis
The presence of OP was positively correlated with fasting blood glucose (P = 0.001, r = 0.32) and HbA1c (P = 0.003, r = 0.3), AN (P = 0.000, r = 0.394), nephropathy (P = 0.004, r = 0.305), and neuropathy scores (P = 0.005, r = 0.294). However, it was not correlated with retinopathy (P = 0.1, r = 0.17) and it was negatively correlated with the parathyroid hormone level (P = 0.007, r = −0.29).
Gender comparison
No differences were determined between women and men when compared by the average age, duration of diabetes, duration of insulin usage, fasting blood glucose, postprandial blood glucose, HbA1c, osteocalcin, Ctx and B-ALP levels, diabetic retinopathy (DRP), nephropathy, AN, OP prevalence, and neuropathy score.
In comparison with women with OP, women without OP had a higher age average (63.9 ± 8.9 years; 57.8 ± 10.5 years; P = 0.03), AN frequency (77.8%; 31.8%; P = 0.001), and neuropathy score (4.1 ± 2.2; 2.4 ± 2.4; P = 0.01), but lower levels of B-ALP (44.3 ± 9.7 IU/L; 71.3 ± 40.5 IU/L; P = 0.000). The two groups were similar in terms of cigarette and alcohol use frequency, type 2 DM and duration of fertility, insulin usage frequency, retinopathy and nephropathy prevalence, FBG, postprandial glucose (PG), HbA1c, osteocalcin, and Ctx levels.
In comparison with men with OP, men without OP had a higher nephropathy frequency (60%; 8.7%; P = 0.007) and levels of HbA1c (8.2 ± 1.6%; 6.2 ± 0.9%; P = 0.05), but lower levels of B-ALP (39.9 ± 5.3 IU/L; 73.8 ± 36.8 IU/L; P = 0.000). The two groups were similar in terms of cigarette and alcohol use rates, type 2 DM duration, insulin use frequency, retinopathy and AN prevalence, neuropathy score, FBG, PG, osteocalcin, and Ctx levels.
Frequency of microvascular complications in patients with and without OP
However, DRP was found in 5 of 22 patients (22.7%) in Group 1 and 6 of 39 patients (15.4%; P > 0.05) in Group 2; AN was detected in 18 of 23 patients (78.3%) in Group 1 and 22 of 41 patients (53.7%; one-sided P = 0.04, two-sided P = 0.06) in Group 2. Similarly, peripheral neuropathy was identified in 22 of 23 patients (95.7%) in Group 1 and 39 of 41 patients (95.1%; P > 0.05) in Group 2, and nephropathy was also found to be similar, with it being detected in 10 of 20 patients (50%) in Group 1 and 12 of 39 participants (30.8%) in Group 2 (P > 0.05) (Table 1).
Discussion
We hypothesize that contrary to what is known in patients with type 2 diabetes, we expect a decreased bone turnover in those with DPN. We expect that too, or it is more evident in those with neuropathy.
Bone formation markers were found to be low in patients with type 2 DM. The neuropathy score was found to be an effective risk factor on the turnover markers.
The presence of OP correlated with complications of type 2 DM. AN was found to be an independent risk factor for OP.
In our study, the osteocalcin and B-ALP levels were found to be lower and Ctx levels similar in patients with type 2 DM compared with healthy individuals. This made us think that the bone turnover decreases in type 2 DM patients. A recent study by Kulkarni et al. showed that serum osteocalcin levels decreased and acid phosphatase levels increased in uncontrolled type 2 DM patients compared with healthy controls. 31 In another study conducted in middle-aged men diagnosed with type 2 DM, the procollagen type 1 amino-terminal propeptide (P1NP) and osteocalcin levels were found to be low and B-Ctx levels were similar compared with healthy controls. 32 The results of the studies were similar, and this indicates that hyperglycemia with impaired functions of osteoblastic and osteoclastic cells may occur in type 2 DM.
Jeffcoate pointed out the influence of DPN on the pathophysiology of skeletal changes for patients with type 2 DM. It is emphasized in the study that DPN caused receptor activator of the nuclear factor kappa-β ligand (RANK-L) to activate irregularly by resulting in CGRP loss, thus adversely affecting bone metabolism in patients with type 2 DM. 33 In a recent study by Rasul et al., the correlation among P1NP, osteocalcin, and Ctx levels, which are bone formation–resorption markers, was examined in 120 patients with type 2 DM: 52 patients were with DPN and 68 patients without DPN. P1NP levels of these markers were higher for patients with DPN than in those without DPN and there was no difference found between the osteocalcin and Ctx levels. For this reason, they reassessed the groups according to gender distribution. The gender distribution analysis showed that among men—43 without DPN and 23 with DPN—P1NP, osteocalcin, and Ctx levels were significantly higher in patients with DPN, but among women—25 without DPN and 24 with DPN—there was no difference in P1NP, osteocalcin, and Ctx levels. 17 In our study, osteocalcin and B-ALP levels were lower in patients with DPN, but there was no difference in the Ctx levels when comparing the two groups. In the subgroup analysis according to gender, it was seen that osteocalcin and B-ALP levels in men and women were less in the DPN group, but Ctx levels were similar in men and women. The results of our own and other studies show that it will be more accurate to carry out a wide range of studies with larger numbers of patients having a similar gender distribution. Another significant consequence of our study is that the neuropathy score assessed by the multiregression analysis was found to be an important risk factor negatively affecting all the bone turnover parameters (See Fig. 1). Thus, we show that in patients with type 2 DM, the bone turnover is reduced in the presence of DPN.
Studies have shown that a high BMI has a protective effect on the bone density in patients with type 2 DM. 34,35 However, despite the protective effect of obesity, the risk of OP in type 2 DM remains controversial due to complications such as nephropathy and neuropathy. 18 Type 2 DM and the factors that have an impact on the pathogenesis of OP are known to result in a prolonged hyperglycemic state, formation of glycosylation end products, Ca-P loss in the kidneys, reduction in the effectiveness of insulin/insulin-like growth factor, nephropathy, changes in vitamin D metabolism, and a decline in the osteoblast function. 36,37 In our study, the fasting blood glucose and HbA1c levels were high in patients with OP. This situation suggests that glycemic control may have a negative effect on bone formation and resorption. Changes in bone metabolism in patients with type 2 DM are caused by the metabolic deterioration accompanying the disease's progression. 34 These are the decrease of osteoblastic activity associated with an increase in oxidative stress and increase in osteoclastic activity associated with an increase in products of advanced glycation. 34,35 One of the most influential factors is hypercalciuria, which is associated with glycosuria. 34 In the study conducted by Anaforoglu et al. on 206 patients with postmenopausal type 2 DM and 61 patients without type 2 DM, the relationship between OP and type 2 DM was analyzed and it was found that there is a negative correlation between microalbuminuria and femur neck bone mineral density. 38 Similarly, in our study, the complications of nephropathy were higher in those with OP.
In the study by Hsu et al., the relationship between high HbA1c levels and OP in patients with type 2 DM was mentioned. In addition, it was found in the same study that the risk of osteoporotic fractures was high due to the high severity of complications in type 2 DM patients and their vulnerability to falling. 39 Chronic hyperglycemia gives rise to a loss of function in the body's systems and organs, including the kidneys, eyes, nervous system, blood vessels, and heart. 6 One of the pathological reactions triggered by hyperglycemia is activation of the polyol pathway, which results in a slowing of nerve conduction. Glucose also tends to irreversibly bind to the amino group of almost any protein it encounters. These binding products, called glycosylation end products, result in a loss of the structure and function of proteins. 9 We determined that patients with type 2 DM had lower osteocalcin and B-ALP levels. When looking at our study in this way, it is evident that nephropathy, the neuropathy score, and AN are related to OP in this same manner. We determined that patients with AN had lower osteocalcin and B-ALP levels. Furthermore, a negative correlation exists between B-ALP, Ctx, osteocalcin, and the neuropathy score. This indicates that in the presence of complications, osteoblasts and osteoclasts are affected, resulting in decreased bone formation–resorption. Our study is of importance because to our knowledge, studies on this issue are limited. There is a need for large-scale work to obtain accurate results in this regard.
There is no clinical study in the literature investigating the relationship between AN and bone formation–resorption in patients with type 2 DM. Our study is quite valuable in terms of investigating the effect of AN on OP. Neuropeptide Y (NPY) and TH, SP, CGRP, and VIP in particular have been found to stimulate the proliferation of osteoblasts in vitro. 19 In addition, they are known to spur both the alkaline phosphatase (ALP) activity and osteocalcin synthesis in osteoblastic cells and regulation of osteoblastic genes. 40 A study by Baldock et al. demonstrated that NPY regulates central and peripheral noradrenergic neurons and their activated receptors, thus releasing blocked noradrenaline. This mechanism protects against bone loss due to the stress associated with catecholamine release. 41 In animals, studies have shown ultrastructural changes in the autonomic nerves of type 2 DM mice, abnormalities in the noradrenergic nerves in the right atrium, and decreased NE content in the left ventricle. 20 In our study, the effect of AN on the bone, another target tissue, was evaluated. In patients with AN, we found lower levels of osteocalcin and B-ALP, indicating bone formation. This result shows that bone formation may be reduced by changes in neurons and released neurotransmitters in the presence of AN.
Serotonin is synthesized in the central and peripheral nervous systems and stimulates proliferation of osteoblasts by means of the hypothalamic neurons. The adrenergic receptors on these osteoblasts become inactivated, and sympathetic stimulation is inhibited as hypothalamic neurons bind to 2C receptors on the plasma membrane. Serotonin also regulates the osteoclast activity and differentiation and may increase the expression of RANK-L. 42 –45 In clinical trials that support these findings at the tissue level, a relationship between the group of antidepressant drugs and bone metabolism has been investigated. Numerous studies have been conducted in recent years on the effect of the selective serotonin reuptake inhibitor (SSRI) on bone metabolism. Some studies have proved bone loss due to long-term SSRI use. These findings show that serotonin plays a critical role in bone formation and resorption. 46 –49 SP, another neurotransmitter, regulates the pathway of Wnt/β-catenin that controls the regeneration of osteoprogenitor cells. 50 In our study, we found that patients with AN related to type 2 DM had a higher risk of OP and those with AN not related to type 2 DM had lower turnover markers such as osteocalcin and B-ALP. When the results of our study are evaluated in light of in vitro studies related to bone homeostasis, changes in cell signaling and function due to AN may influence the bone as well as affect the heart.
Our study has some limitations. The type 2 DM patients who were admitted to the study were diagnosed with OP by DXA. However, the diagnosis of OP needs to be made by computed tomography/magnetic resonance imaging, which is a more sensitive diagnostic method for advanced age and type 2 DM groups. 51 The selection and number of patients were restricted due to the strict exclusion criteria in the study. We think that with a larger group, the results will be significant for turnover markers and neuropathic relationships. Tissue-level studies will be more accurate in terms of clarifying the effect of DPN and AN on bone tissue.
Footnotes
Author Disclosure Statement
The authors have indicated that they have no conflicts of interest regarding the content of this article.
Funding Information
No funding was received for the study.