
Abstract
Background:
We aimed to investigate the influence of locomotive dysfunction (LD) on the future prevalence of metabolic syndrome (MetS) in community-dwelling people using propensity score matching (PSM).
Materials and Methods:
Two hundred and twenty-five volunteers (87 men and 138 women, mean age: 66.9 years) underwent a health screening program in 2012 and 2014. We extracted 92 volunteers with LD and 133 without LD in 2012. After performing 1:1 PSM using clinical variables, including age, sex, individual MetS components, and comorbidities between the two groups, we investigated the prevalence of MetS between the two groups (LD and non-LD) in 2014.
Results:
Seventy-three subjects were enrolled in each group. In 2012, the mean the 25-question Geriatric Locomotive Function Scale was 2.6 in the non-LD group and 13.4 in the LD group. The baseline prevalence of MetS was 9 (12.3%) in non-LD group and 8 (11%) in LD group. After 2 years, the prevalence of MetS in the LD group increased to 18 (24.7%), but only by 8 (11%) (P = 0.031) in the non-LD group. Among MetS components, waist circumference (84.9 vs. 82.5 cm) and systolic blood pressure (SBP) (145 vs. 140 mmHg) in the LD group were significantly higher than in the non-LD group (P = 0.047, P = 0.023).
Conclusions:
The longitudinal analysis showed that LD increases the prevalence of MetS and deteriorates SBP and abdominal circumference over 2 years.
Introduction
Metabolic syndrome (MetS) has been defined as the concurrence of impaired glucose regulation, abdominal obesity, dyslipidemia, and hypertension; insulin insensitivity is a major characteristic. 1,2 MetS causes endothelial disease and subsequently promotes atherosclerosis, cerebral stroke, and myocardial infarction. Several risk factors, such as insulin resistance, obesity, poor diet, smoking, lack of exercise, aging, socioeconomic status, and hormone imbalances, have been identified. 3 –9 The prevalence of MetS is rapidly increasing worldwide and affects ∼12% of men and 1.3% of women in Japan. 10
Given the role sedentary living likely has in MetS development and progression, the Japanese orthopedic association (JOA) has established the Locomotive Syndrome Test in 2013 and publicized its clinical criteria in 2015. Previous reports have suggested that locomotive dysfunction (LD) may be related to MetS. 11 –14 Yoshimura et al. described that MetS increased the risk of knee osteoarthritis (KOA), which is the main pathology of LD. 15 However, the influence of LD on MetS, especially among elderly community residents, remains unknown.
Therefore, understanding a causal relationship between LD and MetS may help clinicians to intervene at an earlier stage, possibly before biomarkers indicate MetS presence. This study aimed to investigate whether LD contributes to MetS onset based on longitudinal cohort analysis. We hypothesize that subjects with LD developed MetS and increased systolic blood pressure (SBP) and waist circumference within a short period.
Materials and Methods
Subjects and study design
Subjects were community-dwelling volunteers who attended a local government health screening program in 2012 and again in 2014. This health screening program was held once every 2 years in Toei town, with most residents attending. 16 –18 Toei is located in the Aichi prefecture in central Japan and has a population of 3800 people, of which 49.6% are elderly (over 65 years). Toei is in a relatively rural area, and many of its residents work in the agriculture and forestry industries.
In this study, we examined medical check-up data and investigated residents' habitus and lifestyles from several questionnaires. The background factors of age, sex, body mass index (BMI), past medical history, and comorbidities were also recorded. The inclusion criteria were: (1) Japanese ethnicity, (2) over 50 years of age, (3) participation in a medical check-up, and (4) ability to walk independently. Individuals were excluded if they had severe walking or standing disabilities or dysfunction of the central or peripheral nervous systems. Individuals who could not respond to the questionnaire by themselves were also excluded.
This study was approved by the Institutional Review Boards of the authors' institutions (no. 15-060). Informed consent was obtained from subjects who agreed to participate in the study.
Definition of LD and MetS
LD was defined based on the 25-Question Geriatric Locomotive Function Scale (GLFS-25). GLFS-25 is a self-administered, but relatively comprehensive questionnaire consisting of 25 items graded on a 5-point Likert scale from no impairment (0 points) to severe impairment (4 points). 19 The questionnaires were administered to the subjects by the same city official throughout the study period. LD was determined as a GLFS-25 marked over 7, and non-LD as under 6. Following the recommendations of the Japanese Committee for the Diagnostic Criteria of MetS, 20 we defined MetS as the presence of central obesity and two or more of the following risk factors: high blood pressure, lipid abnormality, or hyperglycemia (Fig. 1). The severity of comorbidities was assessed using the Charlson Comorbidity Index (CCI). 21
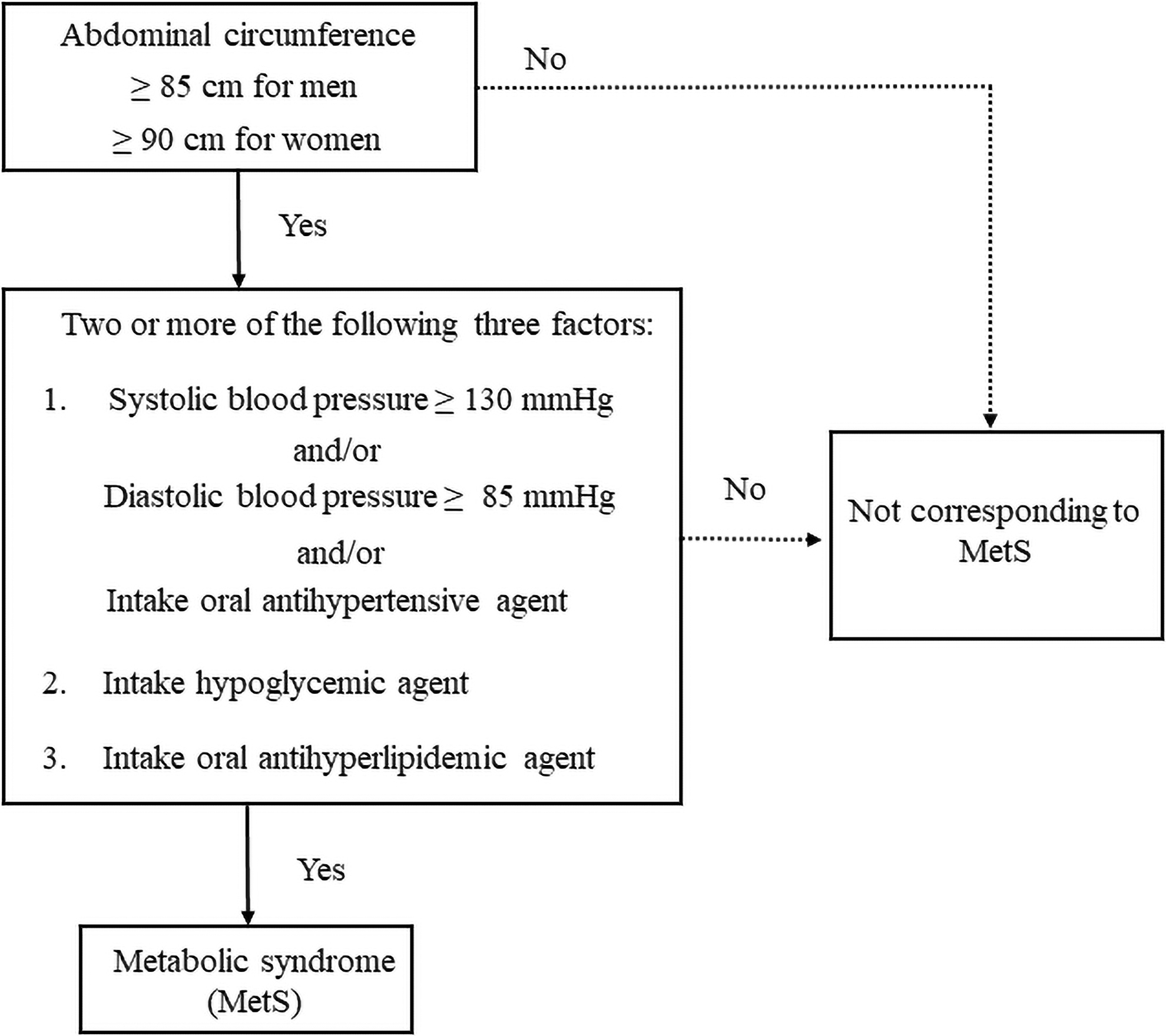
Definition for MetS based on abdominal circumference, blood pressure, and drug history. MetS, metabolic syndrome.
The definition of an exercise habit was as follows: the person has participated in exercise that causes them to sweat lightly for a period of over 30 min each time, twice per week, for over a year.
Statistical analyses
Statistical analyses were performed using SPSS version 25 (IBM-SPSS, Inc., Chicago, IL). Propensity score matching (PSM) models were performed using 1-to-1 nearest neighbor matching techniques without replacement and with a caliper that counts for two times of standard deviation (SD). 22 All continuous variables were expressed as the mean ± SD. Background characteristics, GLFS-25, and MetS components were assessed using Student t-tests, paired t-tests, and χ 2 test or Fisher's test, respectively. The primary outcome of this study was to investigate the prevalence of MetS in 2014, and the secondary outcome was to examine the transition of MetS components between two groups. Values of P < 0.05 were considered to be significant in all analyses.
Results
A total of 367 volunteers participated in the health screening program in 2012. Of those 367 individuals, 142 could not be followed up for 2 years. Therefore, 225 participated in the 2014 health screening program. The eligible 225 volunteers were divided into non-LD and LD groups based on their GLFS-25 score in 2012 (Fig. 2). Table 1 shows the clinical baseline characteristics of each group. Age, sex difference, MetS prevalence, the rate of current smoking, and exercise habitus in the LD group were all significantly different from the non-LD group. Volunteers with MetS tended to have higher GLFS-25 scores than volunteers without MetS (8.7 ± 4.3 vs. 6.8 ± 5.2), regardless of whether no significant difference was found.

Patient allocation to the LD and non-LD groups from the total volunteers. Flow chart of participant selection and study design. LD, locomotive dysfunction.
Comparison of the Eligible (n = 225) and Excluded (n = 142) Participants
Data are presented as the mean ± SD.
Statistically significant.
MetS, metabolic syndrome; SD, standard deviation.
Because the non-LD volunteers were not randomized to LD volunteers, we performed PSM between the two groups using prespecified clinical variables, including age, sex, BMI, MetS prevalence, individual MetS components, smoking, exercise habits, steroid use, and CCI score. The validity of PSM values was confirmed by calculating the area under the curve: 0.740. Finally, a total of 146 subjects composed of 73 non-LD subjects and 73 LD subjects were enrolled. A comparison of the eligible and excluded participants is shown in Table 2. There was no significant difference in age, sex, and MetS prevalence between participants who were not eligible and those who were included after PSM (Table 2).
Clinical Background of Both Groups in Baseline
Data are presented as the mean ± SD.
Statistically significant.
BMI, body mass index; CCS, Charlson Comorbidity Score; LD, locomotive dysfunction.
Baseline characteristics of the PSM participants are shown in Table 3. After performing PSM, confounding variables such as age, sex, the prevalence of MetS, and exercise habitus were controlled. Table 4 shows the comparison of GLFS-25 and MetS prevalence of both groups. In 2014, after 2 years, the LD group showed a significantly higher prevalence rate of MetS than the Non-LD group. However, there were no significant differences in the change of GLFS-25 scores between both groups.
Clinical Backgrounds of Propensity Score Matching Participants in Baseline
Data are presented as the mean ± SD.
BP, blood pressure; DBP, diastolic blood pressure; PSM, propensity score matching; SBP, systolic blood pressure.
Comparison of 25-Question Geriatric Locomotive Function Scale and Metabolic Syndrome Prevalence of Both Groups
Data are presented as the mean ± SD.
Statistically significant.
GLFS-25, 25-Question Geriatric Locomotive Function Scale.
Figures 3 and 4 show the corresponding changes in MetS prevalence and GLFS-25 between both groups. Table 5 shows the components of MetS after 2 years in both groups. Waist circumference and SBP in the LD group increased significantly compared with the non-LD group. Other variables, such as diastolic blood pressure, antihypertensive, hyperglycemic, and anticholesteremic drug prescription rates, did not show significant differences.
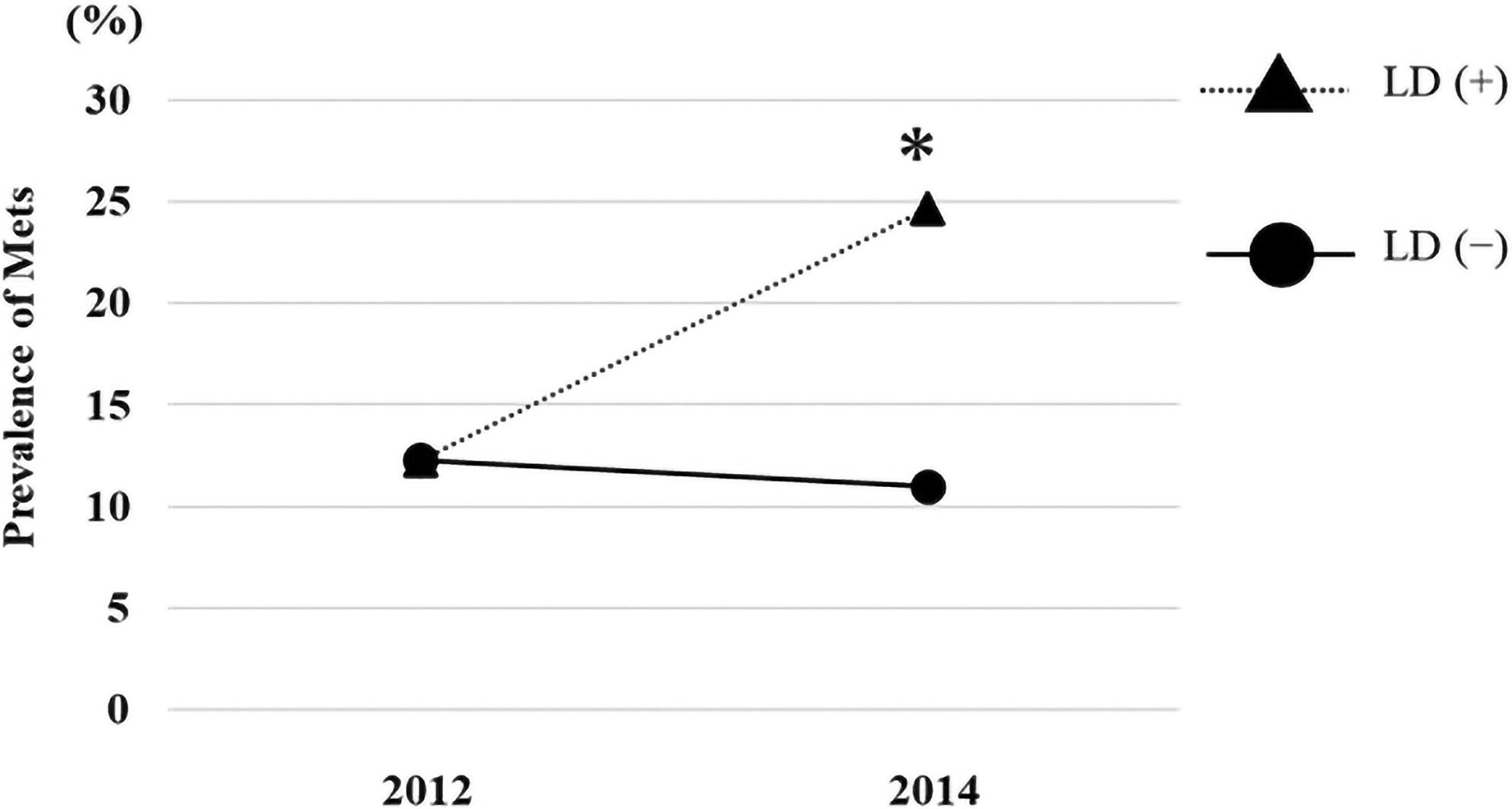
Prevalence of MetS changes from 2012 to 2014 in both groups.*Statistically significant.

GLFS-25 score changes from 2012 to 2014 in both groups. GLFS-25, 25-Question Geriatric Locomotive Function Scale.
Metabolic Syndrome Components After 2 Years in Both Groups
Data are presented at the mean ± SD.
Statistically significant.
Discussion
We have demonstrated that subjects in the LD group experienced a greater prevalence rate in 2014 than subjects in the non-LD group. We also demonstrated that SBP and abdominal circumference in the LD group were significantly higher than those in the non-LD group in 2014.
To the best of our knowledge, this is the first study to examine the influence of LD over MetS components with longitudinal cohort analysis. Several studies have revealed the relationship between LD and MetS components. Mitani et al. reported in a cross-sectional study that increasing SBP and abdominal circumference were associated with a more severe grade of locomotive syndrome risk level in men and women. 23 The risk of hypertension and dyslipidemia has been increased by KOA, composing the main factor for LD. 15
In a Japanese cohort analysis, the presence of KOA has been significantly associated with MetS compared with non-KOA. 11 We also clarified that subjects with LD had a significantly higher prevalence of MetS over 2 years. Therefore, the present study provides additional evidence that LD does not only correlate with MetS, but also increases the risk for MetS in a short period.
Several studies have shown that resistance training such as squatting affects body circulation and metabolism. In a meta-analysis, Lemes et al. described that resistance training reduced SBP. 24 Yagi et al. reported that lower limb muscular fitness, maintained through daily activities, would be useful for controlling obesity. 25 In this study, exercise habits, a confounding factor for MetS, did not show a difference between both groups using PSM. Therefore, further study is required to examine the details of exercise habits, which would affect MetS components.
We encountered several limitations. First, we could not obtain serum total glyceride and serum blood sugar levels from the participants. Although an alternate indicator showing the history of drug treatment for increased triglycerides and fasting glucose as the diagnostic criteria of MetS has been reported, 26 we could have possibly underestimated the correct number of MetS. Therefore, MetS prevalence may not have reflected the correct values. Second, we could not evaluate other risk factors for MetS, including daily diet, socioeconomic status, and individual stress, 27 –29 as well as the effect of hypertensive agents on blood pressure measured at the office. Third, selection bias has to be acknowledged, as excluded volunteers were significantly older than included subjects (Table 1).
Regardless of these limitations, the strengths of this study include longitudinal evaluation of the impact of LD on MetS prevalence and the clarification that LD deteriorates SBP and abdominal circumference.
Conclusion
Our findings have indicated that LD increased SBP and abdominal circumference, suggesting an increase in the prevalence of MetS. Our study highlighted the strong interaction between LD and MetS in a longitudinal analysis.
Footnotes
Acknowledgment
The authors would like to thank Editage for English language editing.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.