
Abstract
Background:
Childhood overweight and obesity are among the major public health problems worldwide. In Mexico, it has been reported in 2018 that 35.6% of children between 5 and 11 years old were overweight or obese. Central obesity is associated with the development of different complications, such as cardiovascular diseases (CVDs). An important tool used to evaluate obesity is the waist-to-height ratio (WHtR), and values higher than 0.5 suggest the existence of cardiovascular risk (CVR). The aim of this study was to evaluate CVR by the WHtR in school-age children from Yucatan, Mexico.
Methods:
This study included a sample of school-age children between the ages of 10 and 13 years from public schools in Yucatan, Mexico. Anthropometric parameters such as body weight, height, body mass index z-score (zBMI), waist circumference, WHtR, and CVR were evaluated.
Results:
A total of 2559 children with a median age of 12.1 ± 0.57 years old were evaluated. The classification by height z score showed that 26.8% were of short height, 73.1% were of normal height, and 0.1% were of tall height. The prevalence of body weight excess determined by zBMI was 48%. The prevalence of normal weight was 44%, and the prevalence of body weight deficiencies was 8%. The CVR determined by WHtR was 47.5%. In the population with obesity, 63.3% had an increased risk of CVDs and 30.7% had a very high risk. Moreover, it was observed that 13.2% of the population with normal weight had an increased risk of CVDs.
Conclusion:
One out of two child 10 to 13 years of age is overweight or obese as defined with zBMI in Mexico. According to WHtR, almost half of this population is at increased CVR, while near two-third of child with obesity are at high or very high CVR.
Introduction
Currently, there is an increased prevalence of overweight and obesity worldwide. 1 Epidemiological studies have revealed important lifestyle changes in the population, including increased intake of refined carbohydrates, sweets, and high-fat diets and a decrease in physical activity. 2 –4 These changes have been directly associated with overweight and obesity, which are defined as the abnormal or excessive accumulation of fat that presents a health risk. 5 According to the World Health Organization (WHO), childhood overweight and obesity are among the major public health problems worldwide, particularly affecting this population in low- and middle-income countries. 6 In Mexico, a prevalence of overweight and obesity of 35.6% in children between 5 and 11 years old was reported in 2018. 7 In Yucatan, 43.1% of school children were overweight according to the National Registry of Weight and Height. 8 Childhood obesity is considered one of the main factors in the development of early-onset chronic diseases, including cardiovascular diseases (CVDs). 9 Thus, the early detection of these pathologies is fundamental to preventing metabolic alterations because the maintenance of obesity from early age to adulthood significantly increases the risk of developing various disorders, such as type 2 diabetes (T2D), hypertension, and dyslipidemia. 10 In this sense, anthropometric parameters are usually used as a tool in the diagnosis of childhood overweight and obesity. The use of the body mass index (BMI) can be scrutinized since it estimates total body weight and not the quantity and distribution of fat. In addition, in the young population, BMI is influenced by sexual maturity and also requires reference tables. Currently, there is evidence that the accumulation of visceral adipose tissue (VAT), compared to subcutaneous adipose tissue, is associated with metabolic disorders, such as altered glucose metabolism, dyslipidemia, and CVD. 11 Thus, another tool considered for the evaluation of obesity that includes the waist circumference (WC) is the waist-to-height ratio (WHtR), which is calculated by dividing WC by height. These parameters have gained ground in the evaluation of factors in young people because these indicators aim to estimate central body fat. 12 Several studies have established a value of ≥0.50 as the cutoff point for the WHtR; values higher than this value suggest the existence of cardiovascular risk (CVR). 12 –15 These parameters can be used as an inexpensive strategy to evaluate excessive body fat and to implement preventive interventions applicable to decrease obesity-related complications. The aim of this study was to evaluate and classify CVR by the WHtR in school-age children from Yucatan, Mexico.
Materials and Methods
Study design and sample population
This was a cross-sectional study that included 2259 school-age children between 10 and 13 years of age. This evaluation was part of the strategies established by Secretaría de Salud and Secretaría de Educación Pública through the program “Salud en tu Escuela” (Health in Your School) between January and December 2019. Participants were recruited from 56 public schools in Yucatan, Mexico, which represent 5% of the total public schools in this region. 16 Eighty-six percent of schools were located in urban areas (>2500 inhabitants), and 14% were located in rural areas (>2500 inhabitants). The school principals of the selected schools obtained the permissions, requesting the parents or legal guardians to provide written informed consent for children to take part in the study. The study was conducted in accordance with the Declaration of Helsinki.
Measurement of anthropometric parameters and adiposity indicators
Trained research personnel measured body weight, height, and WC with standardized procedures. 17 Height was measured with a portable stadiometer (ADE®, model MZ10042) with a length of 220 cm and an accuracy of 1 mm. Children were placed in an upright position, with shoulders and arms relaxed and head in the Frankfort horizontal plane. Body weight was evaluated with a TANITA digital scale (model UM-081) placed on the floor on a flat surface. The weight was obtained while the children were wearing the school uniform, but not shoes or heavy clothes, and the children stood in an erect position with their arms at the sides and looking straight ahead. The WC was measured with a flexible, nonelastic anthropometric tape with an accuracy of ±0.1 cm DRY mark. The WC of the school children was measured in a standing position; the children stood erect, with the abdomen relaxed at the end of an exhalation, the arms at the sides of the body, and the feet together. The tape was placed in a horizontal plane at the level of the narrowest part of the torso. The body mass index z-score (zBMI) was classified according to the WHO age- and sex-specific growth standards with WHO Anthro Plus software. 18 We categorized the weight status in reference to zBMI values as follows: obesity z-score > +2 standard deviations (SDs), overweight z-score between +1 and +2 SD, normal z-score between −1 and +1 SD, malnourished z-score between −1 and −1.9 SD, and underweight z-score < −2 SD. Height was classified as tall ≥2 SD, normal −1.5 to −2 SD, short ≤ −2 to −3 SD, and very short ≥ −3 SD. 19 In addition, the WHtR was calculated by dividing the WC by height in cm, and values of the WHtR ≥0.5 were considered high CVR. 12 This parameter was also categorized according to severity, 20 with a WHtR <0.5 considered to indicate “no increased risk,” 0.5–0.6 considered to indicate “increased risk,” and >0.6 considered to indicate “very high risk.”
Statistical analysis
The distribution of the continuous variables was evaluated using the Kolmogorov-Smirnov Z. The variables are expressed as the mean ± standard deviation (SD) or median and 95% confidence intervals (95% CI) depending on the distribution of the variables. The frequencies are expressed as percentages. To determine the differences between the characteristics of the population, the proportions were analyzed through the chi-squared statistical test and chi-squared test for trend. To determine the differences in quantitative variables between sexes, unpaired t-tests or Mann–Whitney U tests were performed. A value of P < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS program Version 25.0 (SPSS, Inc., Chicago, IL) and Prism 5.0 software (GraphPad, San Diego, CA).
Results
A total of 2559 children were evaluated for this study. Approximately half of the children were girls (55%; n = 1413), and the other half were boys (45%; n = 1146). The mean age was 12.1 ± 0.57 years, and the height was 1.41 (1.40 and 1.41) m (Table 1). Moreover, the overall distribution of the height z scores was 26.8% with short height, 73.1% with normal height, and 0.1% with tall height. The prevalence of short height was similar in girls and boys (Table 1).
General Characteristics and Nutritional Status Data from School-Age Children (n = 2559) Classified by Height and Sex
Data are presented as mean ± SD or median (95% CI) and the frequencies by percentages. Data were analyzed using unpaired t-test or Mann–Whitney U test and the frequencies were analyzed by chi-squared test among sex. All results were considered statistically significant at P < 0.05.
CI, confidence interval; SD, standard deviation; WHtR, waist-to-height ratio; zBMI, body mass index z-score.
Nutritional status evaluated by height and zBMI
The zBMI for the total participants was 0.94 (−1.33, 2.72); the overall prevalence of body weight excess was 48% (29% for overweight, and 19% for obese). The prevalence of normal weight was 44%, and the prevalence of body weight deficiencies was 8% (6% were malnourished and 2% were underweight).
In general, there was a significant difference between the proportions of zBMI classifications among boys and girls (P = 0.038) (Fig. 1). The prevalence of excessive body weight in boys was 54.3%, and that in girls was 42.3% (P < 0.001). Specifically, obesity in boys (24.3%) was higher than that in girls (14.8%), and overweight in boys was higher than that in girls (36.2% vs. 27.7%). The prevalence of normal weight in boys was 38.9%, and it was 48.8% in girls. The underweight prevalence was 6.5% in boys, and it was higher in girls, at 8.7%.
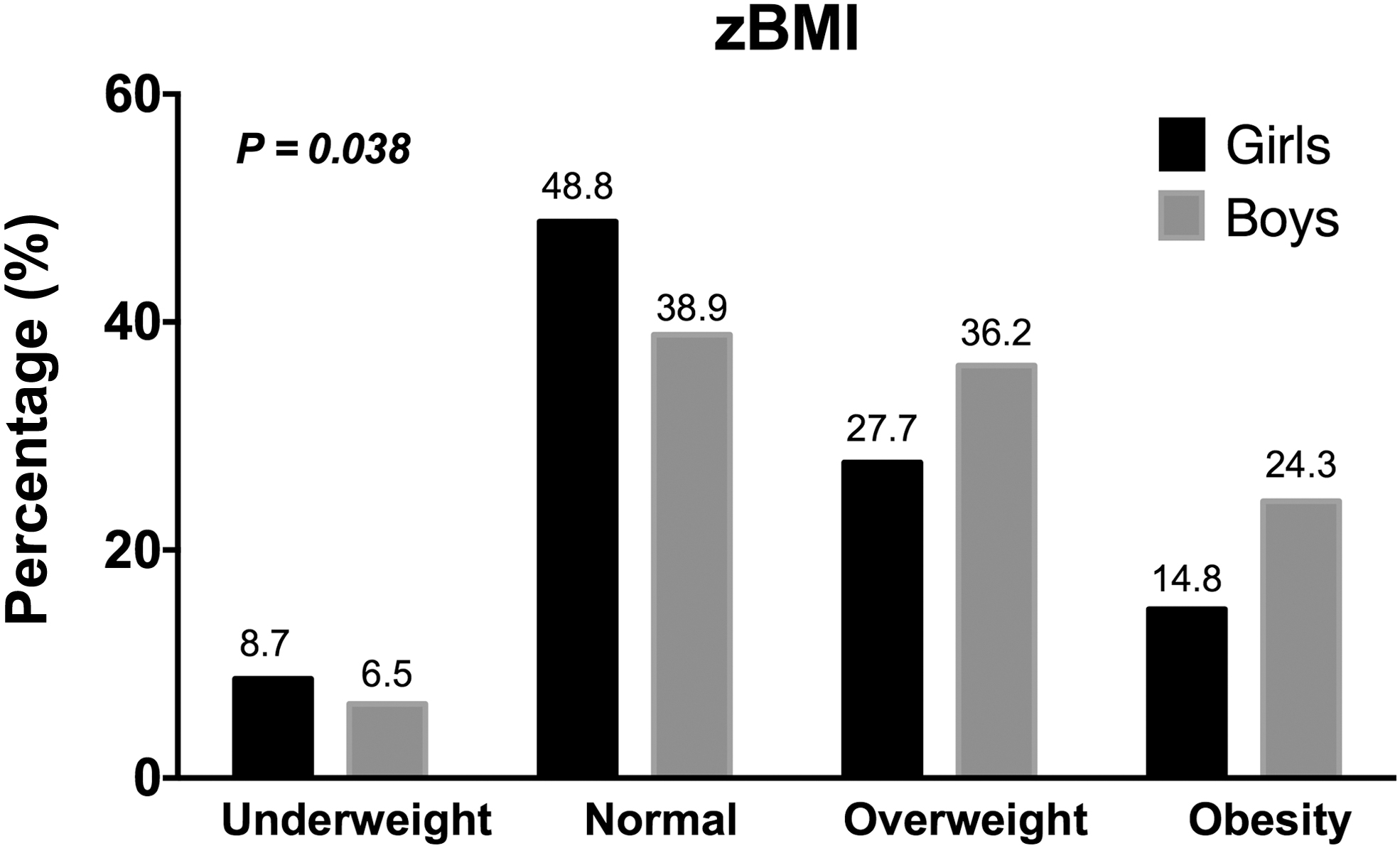
Categorization of school-age children by zBMI (n = 2559). Data were analyzed using chi-squared test for trend. All results were considered statistically significant at P < 0.05. zBMI, body mass index z-score.
Cardiovascular risk
In general, the CVR by the WHtR was 47.5%, as expected, and we observed that the overweight and obese population had a high CVR estimated by the WHtR. Among the children with obesity, 63.3% showed an increased risk and 30.7% showed a very high risk (Fig. 2). On the other hand, 69.8% of the overweight children showed increased risk and 2.2% showed a very high risk, while 28% of the population did not show an increased risk. Interestingly, 13.2% of the population with normal weight had a high CVR, which is of great importance since they are considered a healthy population (Fig. 2). In the stratified analysis by gender, a higher percentage of boys with obesity than girls with obesity presented a very high risk (36.2% vs. 23.4%, P < 0.002). In the overweight population, both genders had similar percentages of increased risk (boys 69.9% vs. girls 69.3%). Finally, in the normal strata, an increased risk was shown in 14.3% of boys and 12.5% of girls (Fig. 2).

Categorization of CVR determined by WHtR and zBMI of school-age children (n = 2559). WHtR <0.5 = “no increased risk” (White bar); WHtR ≥0.5 to <0.6 = “increased risk” (Striped); WHtR >0.6 = “very high risk” (Black bar). Data were analyzed using chi-squared test for trend. All results were considered statistically significant at P < 0.05. CVR, cardiovascular risk; WHtR, waist-to-height ratio.
Discussion
A total of 2559 children were evaluated, and 47.5% of the total population had increased CVR as determined by the WHtR. Among the population, 63.3% of children with obesity were classified as having an increased risk, and 30.7% were classified as having a very high risk. However, 13.2% of the population with normal weight also showed an increased risk. With respect to the evaluation of the nutritional status by zBMI, we observed that 48% of children were classified as having excess weight, and this value is higher than the national average in Mexico. Data from a report in a Mexican population showed that 32.8% of girls and 33.7% of boys between 5 and 11 years of age were classified as overweight or obese, and in the adolescent population, 39.2% of females and 33.5% of males were overweight or obese. 21 The increase in overweight and obesity in the pediatric population has been associated with early development of metabolic disorders that can promote mortality and premature death. 10,22 Thus, it is important to generate strategies for the prevention and early diagnosis of diseases such as T2D, dyslipidemia, and CVD. 23 The WHtR is a simple and inexpensive method recommended for evaluating children. It is an anthropometric index that could help determine if a child has a higher cardiovascular and/or metabolic risk. Our results show that almost half of the total population included in this study had increased CVR, as determined by the WHtR. As expected, the classification analysis of the WHtR showed that 30.7% and 6.3% of overweight and obese children, respectively, had a very high risk (WHtR >0.6). In fact, a higher WHtR value can be used to estimate VAT. In children and adolescents, the increase in VAT could be related to lipid overaccumulation, which in turn promotes alterations such as hyperlipidemia, glucose intolerance, and a proinflammatory state. 24 Indeed, there is evidence of a high correlation between the Z-score and body fat percentage determined by dual-energy X-ray absorptiometry, even when taking racial–ethnic groups into consideration. 25,26 In this sense, there is evidence that there is higher percentages of VAT in the Hispanic children population compared with African American or Asian populations. 27 In fact, a study showed that the prevalence of body fat in Mexican American children was higher than that among white and black American children. 25 Body fat may be modified in the puberty stage, which is a critical period for growth and changes; there is a greater secretion of growth hormone, which causes an increase in fat mass, fat-free mass, and height. 28 Changes in body fat are greater in females than in males (19% vs. 14%). Accordingly, we observed that in Yucatan, 42.5% of the girls presented excess weight according to their zBMI (27.7% overweight and 14.8% obese). This could cause menarche to occur at earlier stages and promote negative effects on longitudinal growth, BMI, and WHtR. 29,30 However, it is known that central adiposity evaluated by the WHtR is minimally affected by age. 31 The optimal cutoff point for the WHtR is associated with CVR and is used for the early detection of abdominal obesity among children in different populations. 9,12,32 High WHtR cutoff values were found to be associated with a higher risk of metabolic syndrome in Mexican adolescents with obesity, 33 and those with a WHtR >0.65 at age 12–39 years were shown to be at a 139% greater risk of death before age 55 years than those with a WHtR <0.538. 12
Interestingly, our results also showed that 13.2% of children with a WHtR >0.5 were classified as normal weight based on the zBMI. Data obtained from a study that included 2457 adolescents (12 to 18 years old) recruited for different surveys in the United States showed that 9% of the population with normal weight had a high prevalence of cardiometabolic risk factors. This risk was defined by the presence of two or more metabolic disorders, such as triglycerides >110 mg/dL and high-density lipoprotein cholesterol <40 mg/dL. 34 Another study that included 178 children from Eastern Finland also showed a WHtR >0.5 in children with healthy weight (normal weight) for 2.97% (95% CI: 2.69–3.25) of boys and 2.44% (95% CI: 2.20–2.68) of girls. 32 Another study showed the presence of risk factors for CVD in 3565 Iranian normal-weight children and adolescents (10–18 years old). 35 The WHtR and BMI percentiles are discordant, and it is suggested that elevated WHtR values allow the identification of a greater amount of central fat. 36 This discrepancy could be explained by the metabolically obese normal-weight (MONW) phenotype, which causes these individuals, despite their normal BMI, to have a higher risk for cardiometabolic diseases. The main determinants of MONW are the anatomical location of fat and inflammation of adipose tissue. 37 The characterization of MONW children has been gaining popularity in public health because it focuses not only on the presence of excess body weight but also on the prevention of future metabolic disorders and cardiovascular events. In this sense, the WHtR is a body fat anthropometric index that targets these diseases, showing an excellent discriminatory CVR power in children and adolescents of both sexes. Thus, the WHtR value could be considered an independent risk factor for several noncommunicable chronic diseases, such as central fat, insulin resistance, high blood pressure, metabolic syndrome, and CVR factors associated with obesity. 38,39
The first limitation of this study is the cross-sectional design. The second limitation is the possible lack of representativeness of the sample, mainly because of the reduced number of individuals included from rural areas, the failure to include private schools, and the possible bias due to the selection of the population as part of a program in public schools, which could have in turn modified the parents or legal guardians tendency to allow their children to participate. In addition, the results could be difficult to extrapolate to other populations due to the age and ethnicity of children. However, we believe that our results in a significant subset of the total public Yucatan schools are especially useful for evaluating fairly accurately the current situation of school-age children, as well as for the generation of new studies.
Conclusion
The prevalence of excessive weight in children was higher than the national prevalence in Mexico, with one out of two children 10–13 years of age overweight or obese. Almost half of this population and near two-third of children with obesity are at increased CVR according to WHtR, an easily performed anthropometric measure that should thus be routinely used in clinical practice as a complementary anthropometric tool to BMI.
Footnotes
Acknowledgments
We acknowledge the teams of nutritionists from the Secretaría de Salud. In addition, we acknowledge the students, parents, teachers, and authorities of the elementary schools of the Secretaría de Educación General del Estado de Yucatán.
Author Disclosure Statement
The authors declare no conflicts of interest with respect to the publication of this article.
Funding Information
The author(s) received no financial support for the research. The editing of this article was supported by the Hospital Regional de Alta Especialidad de la Península de Yucatan.