
Abstract
Background:
The alteration in the composition of the gut microbiota has been associated with an increased risk of developing cardiovascular and metabolic diseases. The present study evaluated the association between the relative abundance (RA) of intestinal Staphylococcus aureus and the inflammatory response with cardiometabolic alterations in children.
Methods:
This cross-sectional study included 1142 children (age 6–12 years), which were classified by degree of adiposity. Anthropometry, cardiometabolic markers, and RA of intestinal S. aureus were measured. Cytokine concentrations were available in 626 children. Path coefficients (PC) were estimated by path analysis.
Results:
RA of S. aureus was positively associated with cholesterol PC = 24.98 (95% CI 10.76 to 39.21) and negatively with triglycerides PC = −13.10 (95% CI −22.73 to −3.48). Body mass index (BMI) Z-scores had significant mediation effects on the association between RA of S. aureus with waist circumference PC = 2.87 (95% CI 0.58 to 5.16), triglycerides PC = 6.63 (95% CI 1.29 to 11.98), low-density lipoproteins (LDL) PC = 1.73 (95% CI 0.27 to 3.18), and high-density lipoproteins PC = −1.20 (95% CI −2.19 to −0.22). Interleukin 6 (IL-6) was negatively associated with glucose PC = −3.01 (95% CI −5.85 to −0.17) and LDL PC = −8.65 (95% CI −16.54 to −0.77), and interleukin 10 (IL-10) was positively associated with glucose PC = 3.37 (95% CI 0.47 to 6.26).
Conclusions:
It is suggested that the RA of S. aureus, IL-6, and IL-10 are associated with cardiometabolic alterations in children, where BMI Z-scores have an important mediating effect for the development of these.
Introduction
According to the World Health Organization (WHO), cardiovascular and metabolic alterations have reached epidemic dimensions, these being the ones that contribute the highest annual mortality from noncommunicable diseases in the world. 1 Various risk factors that promote the development of cardiometabolic disorders have been described as genetic factors [family history of dyslipidemia, type 2 diabetes (T2D), overweight/obesity (OW/OB)], environmental factors (sedentary lifestyle, alcohol consumption, quality diet, stress, smoking) and alterations in the gut microbiota (intestinal dysbiosis). 2
Intestinal dysbiosis has been associated with an increased risk of developing cardiovascular diseases, such as metabolic syndrome, obesity, insulin resistance, and T2D. 3 –5 This association is due to the fact that intestinal dysbiosis causes a deficiency in the energy extraction of food, a decrease in the synthesis of hormones, and the release of short-chain fatty acids (SCFA).
Intestinal dysbiosis also interferes with the insulin signaling pathway, the systemic inflammatory state, and increased body deposits of adipose tissue. 6,7 An increase in the relative abundance (RA) of Staphylococcus aureus has been reported in overweight pregnant women compared with normal weight pregnant women, as well as a positive correlation between weight and body mass index (BMI) with S. aureus RA. 8 Another finding has shown that S. aureus RA is associated with increased plasma cholesterol levels. 9
The effect of the mother's weight on the infant's early childhood gut microbiota has also been studied, finding that the children of women who gained more weight during pregnancy, presented a higher RA of S. aureus like them, suggesting a relationship between the mother's weight gain during pregnancy and the gut microbiota of her children. 10 In the first week after birth, preterm infants, babies born by cesarean, and breastfed babies tend to have a higher abundance of S. aureus, and high concentrations of S. aureus may predispose children to enhanced energy storage, chronic low-grade inflammation, and obesity. 10 –13
Most studies show similar results, associating S. aureus with increased weight gain. OW/OB is considered a worldwide epidemic, and the prevalence of this condition in children is alarming. Since a large percentage of children with OW/OB will continue to present this problem in adulthood, the prognosis for adults includes an increase in cardiovascular and metabolic alterations. 14 Our research aimed to evaluate the association between the RA of intestinal S. aureus and the inflammatory response with cardiometabolic alterations in children. The taxonomic composition of gut microbiota has great diversity, however, based on what has been reported in the international literature, S. aureus has gained great importance, and this study will generate evidence to propose a longitudinal study and evaluate the RA of other bacteria later.
Materials and Methods
Study design and study population
We performed a cross-sectional study between June 2011 and July 2013. The project complies with the Helsinki Declaration and was approved by the Ethics, Research, and Biosafety commissions of the National Institute of Public Health (INSP CI: 1129, No. 1294). The children and parents who agreed to participate gave their assent and signed an informed consent, respectively. The original study database consisted of 2637 children 6 to 14 years of age.
Two thousand one hundred seventeen children between 6 and 12 years of age, not related to each other, residents of four regions of Mexico City (North, South, East, and West) were selected. Children with a diagnosis of infectious and/or gastrointestinal diseases and those under antibiotic treatment 2 months before the start of the study were excluded. Children with no RA information for S. aureus were removed from the study, resulting in a final sample size of 1142. Subsequently, a subsample of 626 children with complete information on serum cytokines was obtained (Fig. 1).
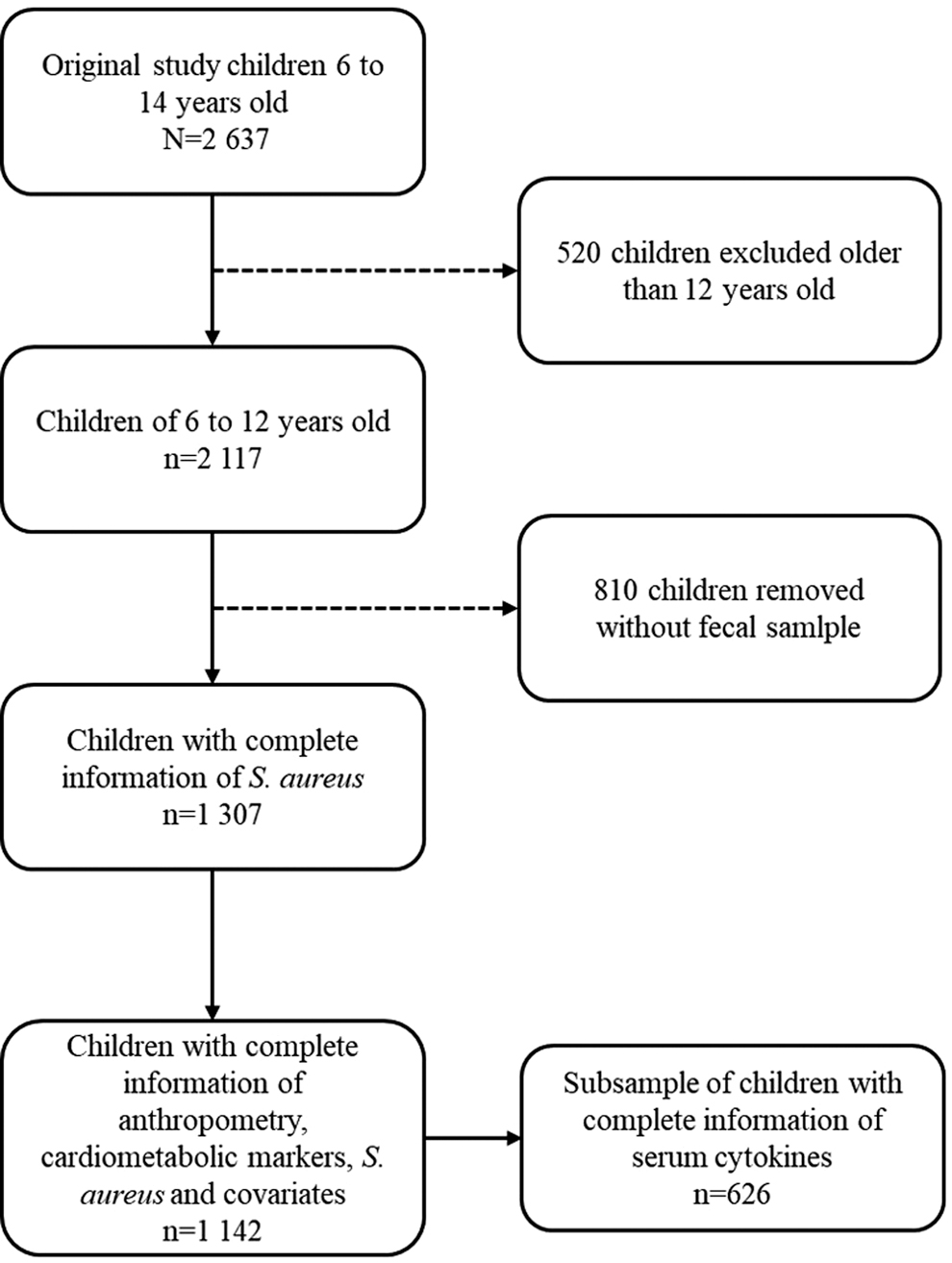
Study sample of children from Mexico City.
Data collection
A questionnaire consisting of 18 questions was applied to collect personal and family pathological antecedents. Subsequently, blood samples were collected by antecubital venipuncture in a 12-hr fast. The samples were centrifuged to obtain the serum. A stool sample was also requested, fecal aliquots were made, and stored in a cryogenic vial at −80°C until use.
Anthropometry
Measurements were made with calibrated instruments and personnel that were previously trained in the use of standardized techniques. 15 The children were evaluated without shoes and with the least amount of clothing possible. Weight and height were measured, these measures were used to calculate the BMI. Waist and hip circumference measurements were made to assess adiposity in the participants.
Cardiometabolic markers
The levels of glucose, total cholesterol, high-density lipoproteins (HDL), low-density lipoproteins (LDL), and triglycerides were measured with the Clinical Chemistry System ILAB 300 plus®. Insulin levels were measured by chemiluminescence on the IMMULITE® equipment. The parameters were established according to the American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement (AHA/NHLBI). 16
Serum cytokines
Serum concentrations of tumor necrosis factor alpha (TNF-α), interleukin 6 (IL-6), and interleukin 10 (IL-10) were measured by the ELISA Kits according to the manufacturer's instructions (PeproTech®, Rock Hill, NJ). The absorbance was determined in a LabSystems Multiskan MS® equipment.
RA of S. aureus
DNA extraction was performed with the QIAamp® DNA Stool Kit (Qiagen, Germany), from 200 mg of stool. DNA concentration was measured at an absorbance of 260 nm and purity was evaluated from the ratio 260/280 nm using a NanoDrop™ Lite spectrophotometer (Thermo Scientific™, Wilmington, DE). The RA of S. aureus was determined by quantitative polymerase chain reaction (qPCR) using the following primers: first sense GCC ACG TCC ATA TTT ATC AGT TC; and first antisense GAT ACA CCT GAA ACA AAG CAT CC. 17
Each PCR reaction was performed in duplicate and required 5 μL of Maxima SYBR Green/ROX qPCR Master Mix (2 × ) (Fermentas®), 1 μL of each primer (concentration of 5 pmol for first antisense and 5 pmol for first sense), 10 ng of DNA template, and 2 μL of nuclease-free water (Fermentas®) in a final volume of 10 μL. The qPCR amplifications were performed on the StepOnePlus™ Real-Time PCR System (Applied Biosystems).
The samples were processed under the following amplification conditions: an initial thermal cycling of 10 min at 95°C, 40 cycles with a denaturation phase at 95°C for 15 sec, 60°C for 15 sec for alignment, and for 20 sec at 72°C for elongation. In addition, to normalize the RA of S. aureus, we use specific universal primers: forward 5′AAA CTC AAA KGA ATT GAC GG3′; and reverse 5′CTC ACR RCA CGA GCT GAC3′. 18 The amplification conditions of the universal primers were: 10 min at 95°C, 40 cycles with a denaturation phase at 95°C for 15 sec, and an alignment and elongation phase of 58°C for 60 sec. The RA of S. aureus was obtained with the following formula: UAR = 2−ΔCt, where UAR = units of relative abundance and ΔCt = S. aureus Ct − universal Ct. 19
Statistical analysis
For the descriptive analysis, we stratified our population by BMI for age according to the Z score as a normal weight [−2 to 1 standard deviation (SD)], overweight (1 to 2 SD), and obese (>2 SD). 20 The comparison between groups was made using the Mann–Whitney U test for continuous variables and chi-square (χ 2 ) for categorical variables. The RA of S. aureus and the serum levels of IL-6, IL-10, and TNF-α were categorized based on the mean of the total population, defining high levels (>mean) and low levels (<mean).
To evaluate the association between S. aureus and serum cytokines with BMI Z-scores, a mutually adjusted linear regression model was performed for the independent variables. Direct and indirect associations were evaluated by path analysis adjusting two independent models, with S. aureus RA and cytokines as independent variables; in both models BMI Z-scores was mediator and the response variable was the cardiometabolic markers.
All models were adjusted for age and family history of OW/OB. We established statistical significance with a P value <0.05. All statistical analyzes were performed using Stata® software version 14.0 (College Station, Texas, USA). The sample size was calculated by Monte Carlo simulation for indirect effects, with a power of 0.8 and 95% confidence level, the required sample size is 116 children. With our minimum (626) and maximum (1142) sample size, the calculated power was 1.
Results
Information from 1142 Mexico City children between 6 and 12 years of age, stratified by degree of adiposity, was analyzed. The combined prevalence of overweight and obesity was 51%. We found that, on average, children with OW/OB are older (9.1 years vs. 8.6 years, P < 0.001) and have a greater waist circumference (74.1 cm vs. 57.5 cm, P < 0.001) than children with normal weight. We also observed that serum levels of glucose (83.0 mg/dL vs. 81.6 mg/dL, P = 0.005), cholesterol (166.2 mg/dL vs. 156.4 mg/dL, P < 0.001), triglycerides (113.1 mg/dL vs. 75.0 mg/dL, P < 0.001), and LDL (109.3 mg/dL vs. 98.9 mg/dL, P < 0.001) were higher in the group with OW/OB, and HDL was lower for this same group (48.1 mg/dL vs. 55 mg/dL, P < 0.001).
Likewise, we found a higher prevalence of a family history of OW/OB in the group of children with a higher degree of adiposity (P < 0.001), as well as a lower RA of S. aureus compared with children with normal weight (P = 0.017). We did not observe statistically significant differences in the distribution by sex, family history of T2D, family history of hypertension, and levels of IL-6, IL-10, and TNF-α (Table 1).
General Characteristics by Degree of Adiposity in Children from Mexico City
Original of this article.
Mann–Whitney U or chi-square for continuous or categorical variables, respectively. Statistically significant differences are marked in bold P < 0.05.
The values represent the mean ± SD or percentages.
HDL, high-density lipoproteins; IL-6, interleukin 6; IL-10, interleukin 10; LDL, low-density lipoproteins; RA, relative abundance; SD, standard deviation; TNF-α, tumor necrosis factor alpha.
To evaluate the independent effect of the association between S. aureus RA and cytokines with BMI Z-scores, a linear regression analysis adjusted for age and family history of OW/OB was performed. To analyze the association of our independent variables simultaneously with BMI Z-scores, we performed a linear regression model mutually adjusted for the independent variables, age, and family history of OW/OB (Table 2). We did not find a statistically significant association.
Association Between Staphylococcus aureus and Serum Cytokines with Body Mass Index in Children from Mexico City
Original of this article.
Adjusted by age and family history of overweight/obesity.
95% CI, 95% confidence interval; BMI, body mass index Z-score.
To evaluate the direct and indirect effect of high RA of S. aureus on cardiometabolic markers, we performed a path analysis, adjusted for age, and family history of OW/OB (Fig. 2). Table 3 shows the results of the path coefficients (PC) of the path analysis, considering the low RA of S. aureus as the reference category. In the direct effects, we found a positive association between high RA of S. aureus with cholesterol PC = 24.98 (95% CI 10.76 to 39.21) and negative with triglycerides PC = −13.10 (95% CI −22.73 to −3.48).

Path diagram to evaluate the direct and indirect effect (mediated by BMI) of Staphylococcus aureus on cardiometabolic markers. Rectangles denote observed variables, arrows are used to represent causal relationship between variables, error variables are enclosed by circles, and numeric values represent the path coefficients. Adjusted for age and family history of overweight/obesity. Reference group: Low RA of S. aureus. BMI, body mass index Z-score; HDL, high-density lipoproteins; LDL, low-density lipoproteins; S_aureus, RA of S. aureus; waist_c, waist circumference. RA, relative abundance.
Direct and Indirect Effect of Staphylococcus aureus on Cardiometabolic Markers in Children of Mexico City
Original of this article.
Statistically significant differences in bold P < 0.05.
Adjusted for age and family history of overweight/obesity.
Reference group: Low RA of S. aureus.
PC, path coefficient.
When evaluating the indirect effect mediated by BMI Z-scores, we found a positive association between high RA of S. aureus with waist circumference PC = 2.87 (95% CI 0.58 to 5.16), triglycerides PC = 6.63 (95% CI 1.29 to 11.98), LDL PC = 1.73 (95% CI 0.27 to 3.18), and negative association with HDL levels PC = −1.20 (95% CI −2.19 to −0.22). With respect to the total effect, waist circumference PC = 2.75 (95% CI 0.33 to 5.17) and cholesterol PC = 26.52 (95% CI 12.26 to 40.78) retain a positive association with high RA of S. aureus.
Subsequently, we evaluated the direct and indirect effect between serum cytokines and cardiometabolic markers through path analysis. The analysis was performed by adjusting the model for age and family history of OW/OB and taking low cytokine levels as a reference category (Fig. 3). In Table 4, we observe a direct and negative association between high levels of IL-6 with glucose PC = −3.01 (95% CI −5.85 to −0.17) and LDL PC = −8.65 (95% CI −16.54 to −0.77).

Path diagram to evaluate the direct and indirect effect (mediated by BMI) of cytokines on cardiometabolic markers. Rectangles denote observed variables, arrows are used to represent causal relationship between variables, error variables are enclosed by circles, and numeric values represent the path coefficients. Adjusted for age and family history of overweight/obesity. Group reference: Low serum cytokine levels. IL_6, interleukin 6; IL_10, interleukin 10; TNF_a, tumor necrosis factor alpha.
Direct and Indirect Effect of Serum Cytokines on Cardiometabolic Markers in Children from Mexico City
Original of this article.
Statistically significant differences are marked in bold P < 0.05.
Adjusted for age and family history of overweight/obesity.
Group reference: Low serum cytokine levels.
We also found a direct and positive association between high levels of IL-10 and glucose PC = 3.37 (95% CI 0.47 to 6.26). We found no indirect association mediated by BMI Z-scores with serum cytokines. Regarding the total effects, high levels of IL-6 are negatively associated with glucose PC = −2.89 (95% CI −5.74 to −0.05) and high levels of IL-10 are positively associated with glucose PC = 3.26 (95% CI 0.37 to 6.16).
Discussion
In this work, we found a direct positive association between high RA of S. aureus with cholesterol and negative with triglycerides in children 6 to 12 years of age. Our results are consistent with those reported by Santacruz et al., where a positive correlation is observed between the RA of S. aureus and cholesterol levels in its total population of pregnant women (r = 0.68; P = 0.003) and in the same way in pregnant women with expected weight gain (r = 0.881; P = 0.002). 9
We also found a positive association mediated by BMI Z-scores between high RA of S. aureus with waist circumference, triglycerides, LDL, and negative with HDL, so we could observe that adiposity participates as a mediator for the development of cardiometabolic alterations. In contrast to our results, a study by Vael et al. reported that low Staphylococcus concentrations were associated with a higher risk of obesity, but it is difficult to compare their findings with those we obtained, since their study is in infants and ours in school-age children, which means that the fecal sample they obtained for the measurement was collected before children consumed solid food.
In addition, the analysis includes the abundance of the Staphylococcus genus and we analyzed the abundance of the S. aureus species. 21 On the other hand, results similar to ours associate high concentrations of S. aureus with weight gain, such as is the case of Kalliomäki et al., who reported an increase in the abundance of S. aureus in children with OW compared with children with normal weight (P = 0.013). 22
The mechanism by which S. aureus may be associated with cardiometabolic disorders can be explained by the fact that it is one of the bacteria that colonizes the intestine immediately after birth. During childbirth, S. aureus is transferred from the feces of the mother to the child or in the case of caesarean section by contact with the mother's skin and the newborn, and due to little bacterial competition, it manages to establish itself and finds an optimal environment to proliferate. 23,24
Under normal conditions, there is a predominance of bacteria with potential benefits for the host. When potentially harmful bacteria predominate, such as S. aureus, there is a state of intestinal dysbiosis, 25 which is caused by various factors, such as the use of antibiotics, stress, radiation, peristalsis, and changes in diet. 26 By reducing the RA of bacterial species with potential benefits, there is a decrease in the amount of SCFA, such as acetate, butyrate and propionate, products of the fermentation of complex carbohydrates, which are known to participate in the maintenance and permeability of the intestinal barrier, preventing the passage of certain bacterial molecules. 27,28
The decrease in SCFA facilitates the free passage of lipopolysaccharides (LPS) from the wall of Gram-negative bacteria into the bloodstream. This increase in circulating LPS is known as metabolic endotoxemia, 7 which generates the activation of Toll-like receptors (TLRs). TLR-4 recognizes LPS and TLR-2 recognizes lipopeptides and lipoproteins from S. aureus.
The activation of TLRs is accompanied by the production of various cytokines that participate in the inflammation process, 29,30 such as an increase in inflammatory mediators IL-6 and TNF-α, and reduced levels of adiponectin, which will ultimately provoke, as a response, increased insulin resistance, increased hepatic glucose, and therefore decreased levels of HDL and insulin. 31,32 Another relevant finding was the direct positive association between high levels of IL-10 and glucose levels. In contrast to our results, Hussain et al. describe a negative correlation for cholesterol (r = −0.45, P < 0.001), triglycerides (r = −0.37, P < 0.05), and LDL (r = −0.30, P < 0.05) with IL-10 values.
The discrepancy between their results and ours could be due to the fact that their study population were adults with diabetes and ours were healthy children. 33 Manti et al. found a negative correlation between IL-10 levels with cholesterol (P < 0.001), LDL (P < 0.005), and triglycerides (P < 0.005). Again, it is difficult to compare them with ours because their sample consisted of children with dyslipidemia, atopy, and healthy children. 34 On the other hand, Atta et al. showed a positive correlation between IL-6 levels and dyslipidemia. However, as in the previous cases, its study population was in adult women diagnosed with systemic lupus erythematosus. 35
Within the limitations of our study, 810 children without feces information were excluded, so we cannot rule out a difference between the children who submitted their sample and those who did not; furthermore, we do not know the reasons why a part of our sample of children decided not to submit it. We evaluated total energy expenditure as a proxy variable of diet since we believe that diet is associated with both our exposure and our variable of interest, that is, as a confusing variable, since we did not observe important changes in our association of interest, we decided to stay with the most parsimonious model.
Regarding reverse causality as a possible explanation for our results, we consider that it is unlikely because the children and their parents were unaware of the study hypothesis and were also unaware that S. aureus and cytokines are associated with cardiometabolic alterations, for which they could not modify risk factors before data collection for the study. Furthermore, in Mexico childhood obesity is perceived as a sign of good health and that cardiometabolic diseases only occur in adults. 36 The above suggests that there were no changes in lifestyles that could be causing reverse causality.
Our findings on elevated IL-6 levels associated with low glucose and LDL levels contrast with other research. These results could be explained because IL-6 participates as a risk factor when it is chronically elevated. In our study population, the children are healthy and there is no chronic inflammatory response due to infection, cardiac, or metabolic disease. Therefore, IL-6 is possibly participating as a cardioprotector by decreasing the levels of low-density lipids in the bloodstream. 37
On the other hand, the association of high glucose levels with high IL-10 levels may be explained by the anti-inflammatory effect of this cytokine, which is elevated in response to proinflammatory cytokines associated with elevated glucose in the bloodstream. 38 In the same way, we did not find an effect of TNF-α on cardiometabolic markers since its association with diseases, such as T2D and insulin resistance has been defined, but not with a healthy population. 39,40 Our results provide evidence on the effect of S. aureus and cytokines on cardiometabolic markers in a healthy population.
Conclusions
Our findings suggest that S. aureus RA, IL-6, and IL-10 are associated with cardiometabolic abnormalities in children. We also observed that BMI Z-scores play a mediating role in the association between S. aureus RA and the development of cardiometabolic abnormalities. The results obtained are important because the RA of S. aureus, IL-6, and IL-10 promise to be potential markers of cardiometabolic alterations. Likewise, these results could support the approach and diagnosis of cardiovascular and metabolic disorders in childhood, carrying out early prevention strategies to reduce the incidence of these diseases in adulthood.
Footnotes
Authors' Contributions
All authors of this article have reviewed and approved the final version. J.C.A.-G.: Conceptualization, methodology, formal analysis, investigation, writing of original draft, and visualization. A.L.-M.: Conceptualization, methodology, investigation, resources, supervision, project administration, and writing of original draft. C.E.D.-B.: Resources, writing—review and editing. Y.C.O.-O.: Resources, data curation, writing–review and editing. A.C.C.-M.: Resources, data curation, writing–review and editing. E.O.-P.: Formal analysis, writing-review and editing. V.H.B.-M.: Resources, writing–review and editing. M.B.-R.: Resources, writing–review and editing. M.C.: Resources, funding acquisition. A.I.B.-G.: Conceptualization, methodology, formal analysis, investigation, resources, supervision, project administration, and funding acquisition.
Acknowledgments
The authors thank the children who participated in this work. This article and the research behind it would not have been possible without the support of the team of Medical Research Unit in Biochemistry of Mexican Social Security Institute and the team of Genetic Epidemiology of National Institute of Public Health.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This work was supported by the National Council of Sciences and Technology (CONACYT, Grant No. CONACYT FOSEC SEP-INVESTIGACIÓN BÁSICA FSSEP02-C-2018-1, CONACYT SSA/IMSS/ISSSTE-CONACYT 2015-262133).