
Abstract
Background and Objective:
The combined effect of insulin resistance (IR) and total plasma homocysteine (tHcy) levels on the risk of mortality in nondiabetic populations has rarely been studied. We aimed to examine the association of tHcy levels and IR with the risk of mortality in nondiabetic populations.
Methods:
This observational cohort study was based on data from the Third National Health and Nutrition Examination Survey (NHANES III) database (1999–2002). A generalized additive model based on the Cox proportional hazards models was applied to estimate the relationship of tHcy levels with all-cause and cardiovascular disease (CVD) mortality. Smooth curve fitting was used to analyze their dose-dependent relationship.
Results:
During 5.7 years of follow-up, a total of 146 (5.8%) deaths occurred, including 65 deaths from CVD among 2053 individuals aged 40–80 years. In the multivariable adjusted model, every 1-μM increment of the tHcy level was associated with a 15% increase in risk of all-cause mortality and 20% increase in risk of CVD mortality among participants with IR (adjusted HR [95% CI]: 1.15 [1.06–1.24] and 1.20 [1.04–1.38]). However, among participants without IR, an increase of 1 μM in the tHcy level was associated with a 6% increase in risk of all-cause mortality and 3% increase in risk of CVD mortality (adjusted HR [95% CI]: 1.06 [1.00–1.13] and 1.03 [0.92–1.16]).
Conclusions:
Homocysteine levels were associated with higher risk of all-cause and CVD mortality among individuals with IR than among those without IR in a nondiabetic population aged 40–80 years.
Introduction
Insulin resistance (IR) is defined as a decline in the reaction of insulin tissue targets to insulin, 1 which is not only more obvious in subjects with type 2 diabetes but also has been confirmed to play a pivotal role in the pathogenesis of a cluster of other metabolic abnormalities, such as dyslipidemia, hypercoagulability, hypertension, and inflammation, 2 and is closely linked to impaired metabolic health, which is now also considered an important risk factor for severe coronavirus disease-19 (COVID-19), 3 and has been shown to have extensive metabolic cross talk with the liver, pancreas, and skeletal muscle. 4 This disorder is characterized by a reduced action of insulin despite concomitant hyperinsulinemia.
The results of the Insulin Resistance Atherosclerosis Study show that when compared with individuals in the highest quintile of insulin sensitivity, individuals with lower insulin sensitivity are at high risk of coronary artery disease. 5 Pyörälä et al. 6 also found that hyperinsulinemia predicted the risk of coronary heart disease (CHD), but the risk attenuated after further adjustment for other risk factors, suggesting that some unmeasured confounders may be involved in the relationship between IR and atherosclerosis. Plasma homocysteine levels may be a potential factor.
Homocysteine (Hcy) is a sulfur-containing amino acid that is an intermediate product of methionine metabolites. Hcy has been recognized as an independent risk factor for atherosclerosis within the past decade 7,8 since McCully 9 first studied the relationship between elevated Hcy levels and progression of atherosclerosis. Furthermore, multiple studies have indicated that elevated plasma Hcy levels are associated with high risk of mortality. 10 –12
However, investigation of the combined effects of total plasma homocysteine (tHcy) levels and IR on the risk of all-cause and cardiovascular disease (CVD) mortality has been very limited, particularly in nondiabetic individuals, which may be clinically important as homocysteine-lowering treatments based on folic acid regimens may be especially effective. Thus, this study was initiated to determine the potential interaction between tHcy levels and IR in nondiabetic individuals from the Third National Health and Nutrition Examination Survey (NHANES III).
Methods
Study population
Data in this study were obtained from the NHANES III database, which is a continuous cross-sectional survey dating back to 1999. The NHANES database collected demographic, physical examination, laboratory, and questionnaire data of noninstitutionalized civilian individuals in the United States. Sample weights and adjustments were made for a complex survey design (including oversampling or nonresponse). 13,14
We conducted a secondary analysis of the data from two 2-year NHANES cycles: 1999–2000 and 2001–2002. The protocols were approved by the National Center for Health Statistics (NCHS) Ethics Review Board. Written informed consent was obtained from all survey participants.
Exposure and outcomes
The tHcy was the primary exposure variable. tHcy was measured in μM using a fluorescence polarization immunoassay on an Abbott IMx analyzer during the period 1999–2001 and Abbott AxSYM analyzer in 2002. Details of the tHcy measurement process are available at
The endpoint was all-cause and CVD mortality. Data of the incidence of mortality were obtained through the NCHS by linking mortality data from the NHANES to death certificate data in the National Death Index. 15 All deaths from CVD, coded as International Classification of Diseases and Related Health Problems, 10th Revision (ICD-10), codes I00-I09, I11, I13, I20-I51, and I60-I69, were classified as CVD mortality in accordance with ICD-10. The follow-up period was from the date of the initial interview to December 31, 2006.
IR definitions
Currently, the gold standard for IR is the euglycemic hyperinsulinemic clamp and frequent intravenous glucose tolerance tests, but both methods are invasive and time-consuming. 16,17 The homeostasis model assessment–insulin resistance (HOMA-IR) is extensively used to evaluate IR based on fasting plasma glucose and fasting plasma insulin levels, which has become a widely used clinical and epidemiological tool. 18,19
Higher values of HOMA-IR indicate more severe IR. In the present study, the HOMA-IR values were calculated using the following formula proposed by Levy et al. 20 : HOMA-IR = glucose × insulin/22.5, in which the unit of glucose is mM and unit of insulin is mU/mL. The presence of IR was defined as an HOMA-IR value greater than the highest tertile of HOMA-IR (>3.0).
Covariates
The following covariates were included as continuous variables: age, body mass index (BMI, kg/m2), waist circumference (cm), mean systolic blood pressure (SBP, mmHg), mean diastolic blood pressure (DBP, mmHg), red blood cell folate level (ng/mL), serum folate level (ng/mL), serum vitamin B12 level (pg/mL), glycohemoglobin level (%), C-reactive protein (CRP) level (mg/dL), total cholesterol level (mg/dL), triglyceride level (mg/dL), low-density lipoprotein cholesterol (LDL-C) level (mg/dL), high-density lipoprotein cholesterol (HDL-C) level (mg/dL), estimated glomerular filtration rate (eGFR, mL/min/1.73 m2), methylmalonic acid level (μM), and levels of dietary supplements such as vitamin B6 (mg), vitamin B12 (mcg), and folic acid (mcg).
The categorical variables included sex, race/ethnicity (grouped as non-Hispanic white, black, Mexican American, other Hispanic, or other), education status (dichotomized as high school diploma, high school diploma, or any training above high school diploma), smoking status (grouped as never smoker, current smoker, or former smoker), alcohol consumption (classified as drinks of less than 5 grams or more than 5 grams per day), physical activity (classified as sedentary, low, moderate, or high levels based on the distribution of metabolic equivalent of task–minute levels in the present NHANES sample), CHD, and hypertension.
CHD was defined as a self-reported diagnosis of CHD by a physician. Hypertension was defined as meeting any of the following criteria: SBP ≥130 mmHg, DBP ≥90 mmHg, or self-reported physician diagnosis of hypertension.
Statistical analyses
Statistical analyses followed the guidelines of the Centers for Disease Control and Prevention (
A generalized additive model (GAM) and smooth curve fitting (restricted cubic spline) were used to determine the relationship of tHcy levels with the risk of all-cause and CVD mortality in participants with and without IR. Covariates were defined as potential confounders if they changed the estimates of tHcy levels on the risk of all-cause mortality by more than 10%. The following covariates were included: age, sex, race/ethnicity, education status, smoking status, alcohol consumption, physical activity, CHD, hypertension, BMI, waist circumference, DBP, serum folate, CRP, total cholesterol, eGFR, methylmalonic acid, and dietary supplements of vitamin B6, vitamin B12, and folic acid. Age covariates were entered into the equation using smooth curve fitting to account for the potential nonlinear relationship between age and mortality.
We presented three models: a nonadjusted model (not adjusted for any covariates), a minimally adjusted model [adjusted for age (smooth), sex, and race/ethnicity], and a multivariable adjusted model (adjusted for all above potential confounders). Hazard ratios (HRs) with 95% confidence intervals (CIs) comparing event rates between groups (with IR vs. without IR) were estimated using the Cox proportional hazards regression models. In the analysis, the tHcy level was entered into the equation as both a continuous variable and a categorical variable (<15 and ≥15 μM).
All tests were two-sided and statistical significance was set at P < 0.05. All analyses were performed using the R statistical software package (
Results
Selection of participants
A total of 2503 individuals aged between 40 and 80 years were selected from the NHANES database from 1999 to 2002. After excluding participants with diabetes (n = 68), missing data on all-cause mortality (n = 8), missing fasting plasma insulin levels (n = 3248), missing fasting plasma glucose levels (n = 3), missing tHcy levels (n = 2), and extreme tHcy levels (>40 μM, n = 5), 2503 eligible participants were included in the final analysis (Fig. 1).
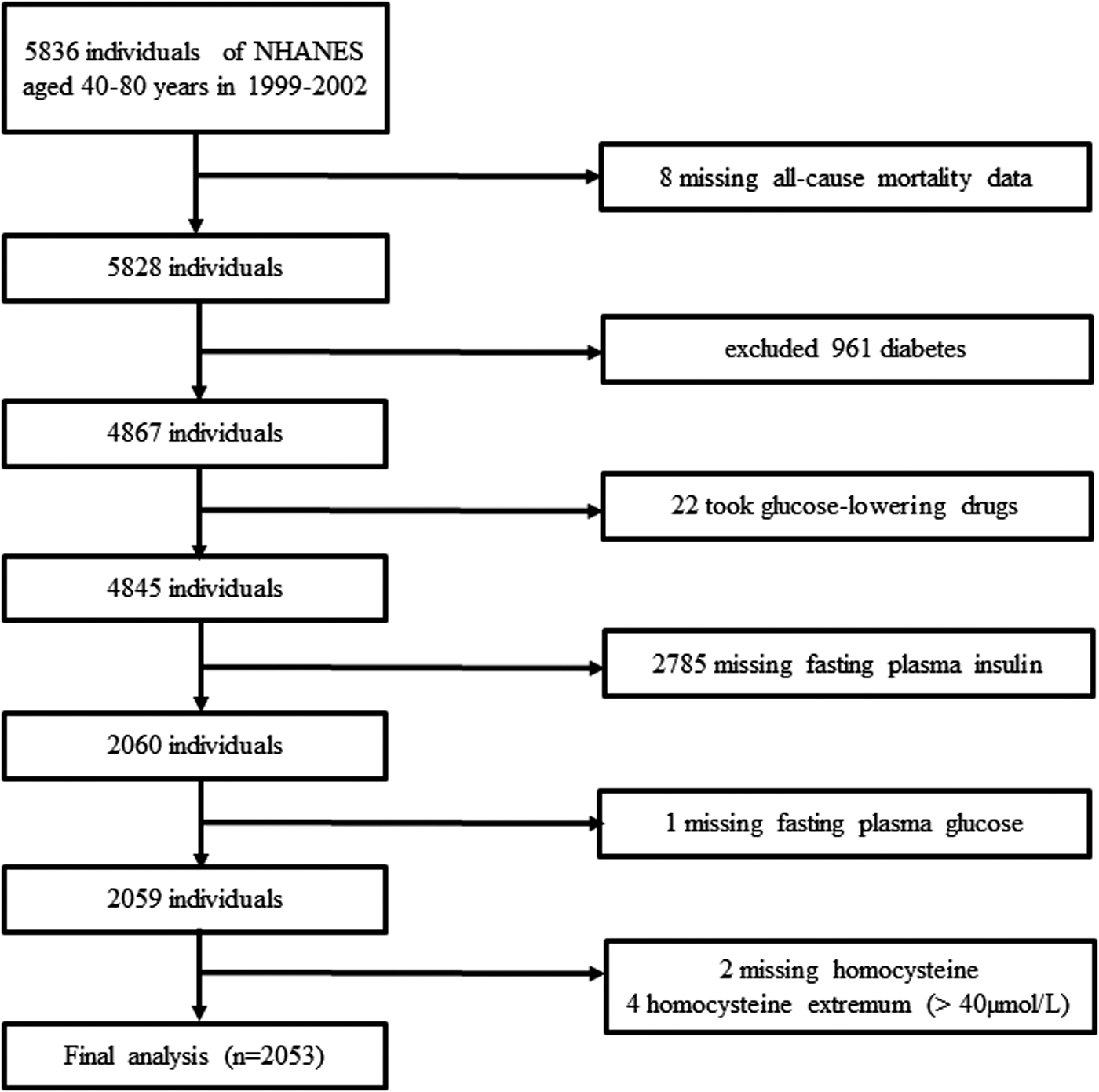
Flow chart of participants.
Baseline characteristics
There were 1267 participants without IR (HOMA-IR ≤3.0) and 786 participants with IR (HOMA-IR >3.0) in the present study. The weighted distribution of the cohort characteristics by tertiles of HOMA-IR is presented in Table 1. The average age was 54 years (47% men). Compared with the low level (Tertile 1) of HOMA-IR, participants with the highest level (Tertile 3) of HOMA-IR were slightly older, more likely to be male, more sedentary, and more likely to be diagnosed with CHD and hypertension; had significantly higher alcohol consumption, BMI, waist circumference, SBP, glycohemoglobin, fasting plasma insulin, fasting plasma glucose, CRP, total cholesterol, triglyceride, and LDL-C levels; and had lower serum folate and HDL-C levels and eGFRs (Table 1).
Characteristics of Study Participants
Continuous variables are presented as mean (SE), calculated by the weighted linear regression model. Categorical variables are presented as n (%) (SE), calculated by the weighted chi-squared test.
Unweighted number of observations in the dataset.
Estimated using the CKD-EPI equation: eGFR = 141 × min(Scr/κ, 1)α × max(Scr/κ, 1)−1.209 × 0.993Age × 1.018 [if female] × 1.159 [if black], where Scr is serum creatinine, κ is 0.7 for females and 0.9 for males, α is −0.329 for females and −0.411 for males, min indicates the minimum of Scr/κ or 1, and max indicates the maximum of Scr/κ or 1.
BMI, body mass index; CHD, coronary heart disease; CRP, C-reactive protein; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; HOMA-IR, homeostasis model assessment–insulin resistance; LDL-C, low-density lipoprotein cholesterol; RBC, red blood cell; SBP, systolic blood pressure; SE, standard error.
Association of homocysteine with all-cause mortality in participants with and without IR
A total of 2053 eligible participants with 11800.8 person-years of follow-up (median follow-up duration, 5.7 years) were included in the study. During the follow-up period, a total of 146 (5.8%) deaths occurred, including 65 deaths from CVD. The HRs and 95% CIs of the three models are listed in Table 2. In the nonadjusted model, the HR (95% CI) for all-cause mortality per 1-μM/L increment of tHcy was 1.09 (1.05–1.13) among participants without IR and 1.17 (1.11–1.23) in participants with IR.
Association of Homocysteine with All-Cause and Cardiovascular Disease Mortality in Participants With and Without Insulin Resistance
Nonadjusted model: no covariates were adjusted.
Minimally adjusted model: adjusted for age (smooth), sex, and race/ethnicity.
Multivariable adjusted model: adjusted for age (smooth), sex, race/ethnicity, education status, smoking status, alcohol consumption, physical activity, CHD, hypertension, BMI, waist circumference, DBP, folate (serum), vitamin B12 (serum), CRP, total cholesterol, eGFR, methylmalonic acid, and dietary supplements of vitamin B6, vitamin B12, and folic acid.
Cox proportional hazards models were used to estimate HRs and 95% CIs.
CI, confidence interval; CVD, cardiovascular disease; HR, hazard ratio; IR, insulin resistance; tHcy, total plasma homocysteine.
In the multivariable adjusted model, the trend was consistent. Every 1-μM increase in the tHcy level was associated with a higher risk of all-cause mortality among participants with IR than those without IR (aHR [95% CI]: 1.15 [1.06–1.24] vs. 1.06 [1.00–1.13]). To test the robustness of the results, we also treated tHcy as a categorical variable (<15 and ≥15 μM) in another analysis and observed no changes in the trend (Table 2).
Association of homocysteine with CVD mortality in participants with and without IR
The results of the correlation between tHcy levels and CVD mortality were similar to that between tHcy levels and all-cause mortality. In the multivariable adjusted model, the adjusted HR (aHR) (95% CI) for CVD mortality per 1-μM/L increment of tHcy was 1.20 [1.04–1.38] among participants with IR and 1.06 [1.00–1.13] among those without IR. The trend did not change when the tHcy level was treated as a categorical variable (Table 2).
Moreover, as is shown in Fig. 2, we conducted a GAM and smooth curve fitting to show the dose–response relationship of tHcy with all-cause and CVD mortality in participants with and without IR. A complete case analysis, including participants with missing fasting insulin and fasting glucose levels, was conducted to assess the effect of missing data.
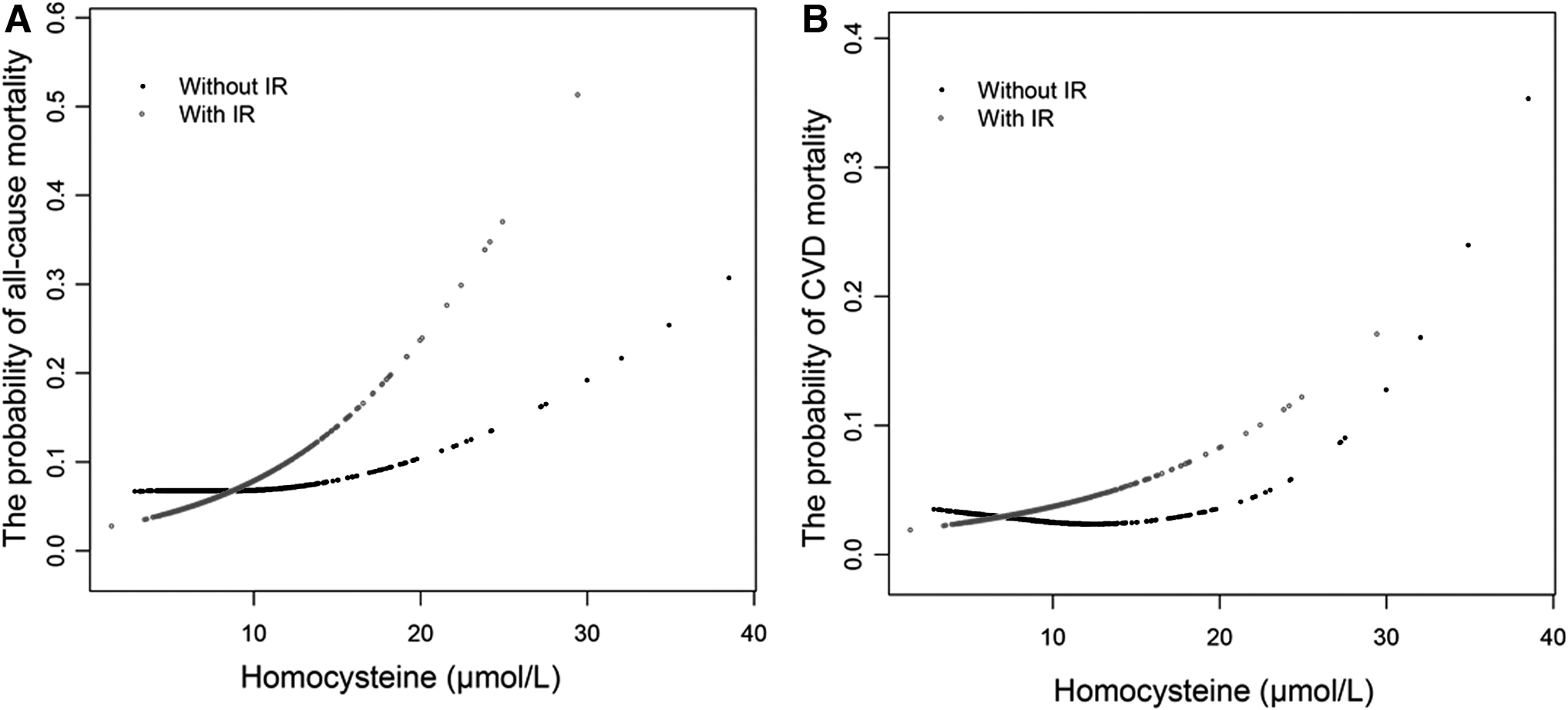
Dose–response relationships between tHcy and the probability of all-cause and cardiovascular disease mortality in participants with and without insulin resistance.
A total of 4280 eligible participants were included in separate sensitivity analyses (Supplementary Fig. S1). We found that the results were consistent with those of the missing dataset (Supplementary Table S1).
Discussion
Our findings
Our study was trying to confirm the effect of the interaction between IR and tHcy on the risk of all-cause and CVD mortality among nondiabetic individuals in an American population. In the multivariable adjusted model, every 1-μM increase in the tHcy level was associated with a higher risk of all-cause mortality among participants with IR than those without IR (aHR [95% CI]: 1.15 [1.06–1.24] vs. 1.06 [1.00–1.13]).
In addition, the aHR (95% CI) for CVD mortality per 1-μM/L increment of tHcy was 1.20 [1.04–1.38] among participants with IR and 1.06 [1.00–1.13] among those without IR.
Previous studies
We noted that tHcy was a risk factor for all-cause mortality in nondiabetic individuals with IR, which suggests that IR or hyperinsulinemia may play an important role in Hcy metabolism. Many previous studies have investigated the interaction between Hcy levels and IR, both of which are well-known cardiometabolic risk factors. 21 –23 The results of the Framingham Offspring Study showed that Hcy is associated with IR, which may be part of the reason for the increased risk of CVD. 24 Tessari et al. implied that decreased Hcy trans-sulfuration is correlated with IR in hypertensive subjects. 25
Several cross-sectional studies have reported an inverse association between plasma Hcy levels and insulin sensitivity. 26,27 However, previous IR studies did not yield consistent outcomes. A secondary analysis of heart disease and diabetes risk indicators in a screened cohort study failed to find a positive relationship between Hcy levels and insulin sensitivity when measured by an intravenous glucose tolerance test. It is important to note that this study included only 100 healthy male participants aged 31–62 years. 28
The NHANES III investigation also examined the association of serum Hcy with IR in a sample size of 560 men aged 40–74 years, and no consistent association was found between the two. 29 However, plasma vitamin B and folate levels were not estimated in this study.
Possible explanations for our findings
Hcy is epidemiologically related to IR, reflecting a low-grade systemic inflammatory condition. However, the specific mechanism underlying the link between Hcy and IR remains unclear. Most studies have suggested that Hcy levels are similar in patients with and without type 2 diabetes. Similarly, in the present study, there was no statistically significant difference in Hcy levels between participants with and without IR.
Therefore, the possible hypotheses are as follows: IR seems to influence Hcy metabolism through a critical mediator in endothelial dysfunction and by promoting atherosclerosis. Li et al. confirmed that Hcy could promote IR and impair the glucose transport process by inducing the expression and secretion of resistin, which has been validated to be involved in the pathogenesis of IR from adipocytes in in vivo and in vitro experiments. 30 –32
In addition, elevated insulin levels may modulate the activity of key enzymes involved in Hcy metabolism, such as 5,10-methylenetetrahydrofolate reductase or cystathionine β-synthase. 25,33 Moreover, some studies have shown that Hcy thiolactone may be a relevant mediator of the inhibition of insulin signaling by oxidative stress, eventually leading to IR. 34
Folate, vitamin B12, and total plasma homocysteine
Folate and vitamin B12 are important for reformation of methionine from Hcy. Elevated tHcy levels may reflect a lack of folate and vitamin B12. 35,36 B-complex vitamins can reduce tHcy levels by promoting Hcy metabolism. 37 In our study, participants in the higher tertile of HOMA-IR had lower levels of serum folate and serum vitamin B12.
The results of another NHANES III investigation confirmed that there was an inverse relationship between serum folate levels and IR in nondiabetic American adults. 38 Setola et al. 39 reported that folate and vitamin B12 supplementation could improve IR accompanied by a 27% reduction in HOMA-IR and decrease in the Hcy level. Therefore, it is reasonable to infer that a relative reduction in folate and vitamin B12 may contribute to this effect.
Clinical importance
IR and hyperhomocysteine are both risk factors for CVD. Our findings imply that IR may enhance the effect of Hcy on progression of atherosclerotic disease. These theories, if confirmed, would help recognize the population at increased risk of CVD, particularly those with the burden of diseases related to IR, such as obesity, type 2 diabetes, hypertension, or dyslipidemia, and who would benefit from folate supplementation.
Limitations
The limitations of this study are noteworthy. First, it was not possible for us to prove a causal link between Hcy levels and IR due to the observational nature of the study. Second, we cannot exclude the possibility of residual confounding effects by an unmeasured baseline characteristic, such as hip circumference, which is now established as an important and independent determinant of IR and CVD. 40 The risk of CVD mortality might be underestimated if hip circumference is not adjusted.
Third, tHcy, glucose, and insulin levels were based on a single measure, and we cannot rule out that the results may be influenced by individuals taking folic acid or vitamin B supplements during the follow-up period. Finally, IR status was measured by HOMA-IR, but not by direct measurement, in our study. This may lead to misclassification of IR, which would weaken the association between the tHcy level and IR and underestimate the effect of IR on Hcy.
Overall, larger scale, randomized controlled trials are needed to more accurately estimate the strength of the correlation between tHcy levels and CVD mortality among individuals with IR.
Conclusions
Overall, the strength of the relationship of tHcy levels with risk of all-cause and CVD mortality was higher among individuals with IR than among those without IR. IR may enhance the role of tHcy in progression of atherosclerotic disease in nondiabetic individuals.
Footnotes
Acknowledgments
The authors thank all the staff members of the NHANES study for their valuable contributions. They also thank Jie Liu of the Department of Vascular and Endovascular Surgery, Chinese PLA General Hospital; Haibo Li of the Fujian Maternity and Child Health Hospital; and Changzhong Chen and Xinglin Chen of Yi-er College for their contributions to the statistical analysis. The authors would like to thank Editage (
Data Availability Statement
The NHANES datasets are publicly available on DataDryad (
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.