
Abstract
Background:
Statin therapy is a cornerstone of cardiovascular disease treatment and prevention. Unfortunately, 7%–29% of statin-treated patients complain of muscular fatigue, cramps, and/or pain (statin-associated muscle symptoms [SAMS]). In recent years, the important role of vitamin D in muscle health maintenance has been highlighted. In addition, hypovitaminosis D is very prevalent, and might be a reversible risk factor for SAMS occurrence.
Methods:
In our controlled intervention study, patients suffering from both SAMS and hypovitaminosis D underwent vitamin D replacement for 6 months. SAMS intensity and its impact on the quality of life were evaluated with a questionnaire during follow-up. A subgroup of patients who were not at the low-density lipoprotein cholesterol (LDL-C) target attempted a statin rechallenge after 3 months. Control subjects, with SAMS only, were not treated.
Results:
Blood vitamin D levels reached 261% of baseline values. Pain intensity was reduced by 63%, and all life quality indicators improved. At follow-up, percentage variations in SAMS intensity and in vitamin D levels were inversely related (r = 0.57, P = 0.002). In a multiple regression analysis, this association was found to be independent. Among the rechallenge subgroup, 75% successfully tolerated high-intensity statins during the follow-up. The parameters of interest were unchanged in control subjects.
Conclusions:
In our findings, the amount of increase in vitamin D concentrations is directly related to SAMS improvement. Although randomized studies are needed, 25(OH)D levels can be measured, and eventually supplemented, in all patients suffering from SAMS, and this can be done together with a statin rechallenge after 3 months for patients who are not at the LDL-C target.
Register:
The study protocol was registered with the EudraCT clinical trial register [ID: 2019-003250-83] in date April 8, 2020.
Introduction
Statin therapy is one of the most commonly used approaches in the treatment of patients with a high cardiovascular risk. 1,2 A wide meta-analysis showed that a reduction in low-density lipoprotein cholesterol (LDL-C) of 2–3 mM is associated with a 40%–50% risk reduction for all cardiovascular diseases. 3
Although it is still debated, 4,5 long-term adherence to statin therapy appears to be an issue. In randomized controlled trials, 33% of patients in primary prevention and 18% of patients in secondary prevention stop statin intake within 5 years after the first prescription. 6,7 In clinical practice, these rates are even higher (11%–19% just after the first year). Thus, this low statin compliance is responsible for an increase of 15% in cardiovascular risk compared with proper therapy compliance. 8,9
At least half of the treatment interruptions are due to the onset of fatigue, cramps, and/or muscular pain (statin-associated muscle symptoms [SAMS]). 10,11 Approximately 7%–29% of the patients under statin treatment complain of SAMS occurrence. 12
In the field of brawn health, vitamin D also has an important role in the maintenance of muscle trophism and function, and its deficiency can lead to striate muscle impairment. 13,14
Consistently, among the different hypotheses proposed to explain the mechanisms underlying the SAMS pathogenesis, 15 several recent trials showed that low vitamin D levels might be a reversible risk factor for SAMS occurrence. 16 –21 In fact, according to former studies, low vitamin D levels are common among patients who suffer from SAMS. Depending on the cutoff values, the incidence of deficiency is more prevalent in adults with SAMS, ranging from 64% 17 to 81%, 22 than in healthy adults, ranging from 14% 23 to 43%. 17
However, some trials disagree regarding the relationship between hypovitaminosis D and SAMS occurrence. 24 –28 Because of this debate, 29 current guidelines on the clinical management of SAMS do not recommend routine vitamin D use. 12
Despite this, vitamin D use is sometimes carried out in clinical practice, being proposed by physicians to 8.3% of patients complaining of SAMS. 30
Therefore, the present study aimed to evaluate the impact of vitamin D replacement on SAMS and life quality aspects in patients suffering from both SAMS and newly diagnosed hypovitaminosis D.
Materials and Methods
Study design
This was a controlled intervention study with a duration of 6 months.
The intervention group was composed of patients suffering from both SAMS and hypovitaminosis D. The clinical features of SAMS were evaluated with a validated pain questionnaire, and creatine phosphate kinase (CK) levels were measured at baseline and after 3 and 6 months of vitamin D supplementation. When LDL-C was not at target, a statin rechallenge was attempted after 3 months of vitamin D therapy.
The control group was composed of patients suffering from SAMS but with a normal vitamin D level, seen in our outpatient facility during the same period as reported above. No intervention was performed and no placebo was administered in this group, but they were kept only under clinical and laboratory observation, to detect any change in symptoms due to other reasons (e.g., social factors).
Clinical setting
Patients were selected among 2952 patients seen from 2016 to 2018 in the outpatient facility of the Lipid Clinic of Magna Graecia University, Catanzaro, Italy (Fig. 1). Among them, those suffering from SAMS for at least 1 year despite every optimization strategy, already undertaken, were considered for the study. Recruitment of the patient and initiation of therapy were undertaken in the first 6 months of 2019, and treatment of the last patient was ended in December 2019 to rule out seasonal factors.
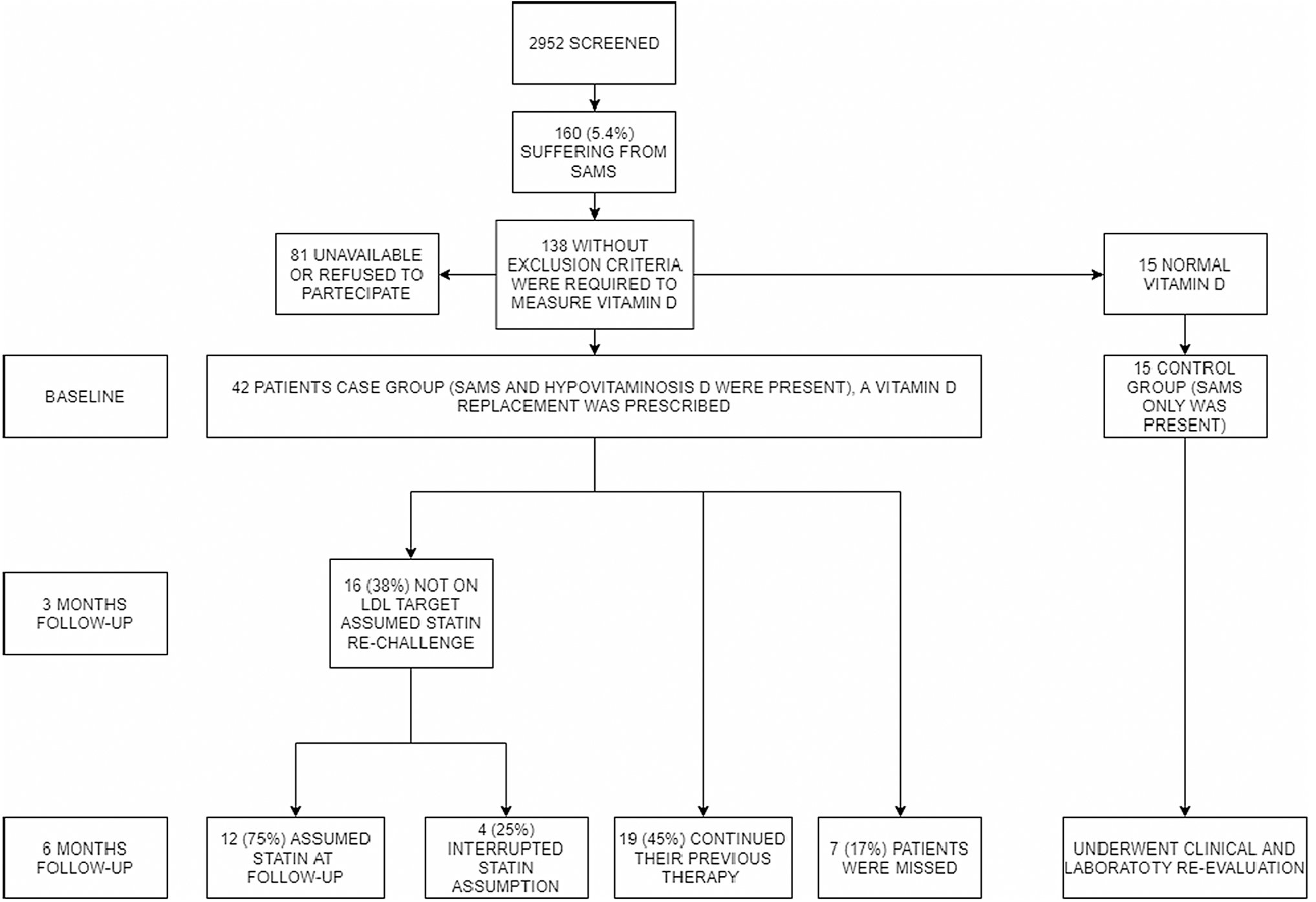
Study flowchart.
Inclusion and exclusion criteria
The inclusion criteria were as follows: SAMS presence, defined as muscle-related complaints (e.g., pain, weakness, or cramps) with or without CK elevation, whose presentation was determined by the assumption of a statin at the highest dose, or two or more statins at lower doses. The interruption of the therapy led to remission of the symptoms. Those conditions could not be better explained by other comorbidities. 31 Hypovitaminosis D was defined as a 25(OH)D concentration <30 ng/mL. 32
The exclusion criteria were as follows: occurrence of rhabdomyolysis (CK more than 10 times the upper limit of normal, typically associated with myoglobinuria) under statin therapy, 26 use of dietary supplements (such as formulation containing red rice yeast and multivitamin), and patients with diagnosed rheumatic or musculoskeletal illnesses whose symptoms included muscular or joint pain, hypothyroidism, alcohol/drug dependence, and life-threatening clinical conditions.
Patients could be either assuming a low-intensity statin therapy at baseline or not taking any statin therapy.
Recruitment procedure
Patients suffering from SAMS who met the inclusion criteria were contacted and invited to undergo a blood vitamin D measurement. The study protocol was approved by the local ethics committee and conducted in accordance with the Declaration of Helsinki. The study protocol was registered with the EudraCT clinical trial register [ID: 2019-003250-83].
Clinical and blood examinations
All subjects included in the study underwent a complete clinical examination at baseline, and after 3 and 6 months.
SAMS intensity was evaluated by the validated Brief Pain Inventory (BPI) short form questionnaire (Fig. 2) 27,33 ; only sections 5 and 9 were administered to assess pain intensity and its influence on the quality of life and common life activities of the patient. The BPI scales showed acceptable internal consistency and reproducibility in Tan et al. 33 There, the Cronbach's α coefficients were 0.85 for the intensity scale and .88 for the life quality indices scales, adequately high to support the use of the BPI scores as outcome variables in treatment outcome studies, and to assess the effectiveness of specific pain interventions, as reported by the authors.
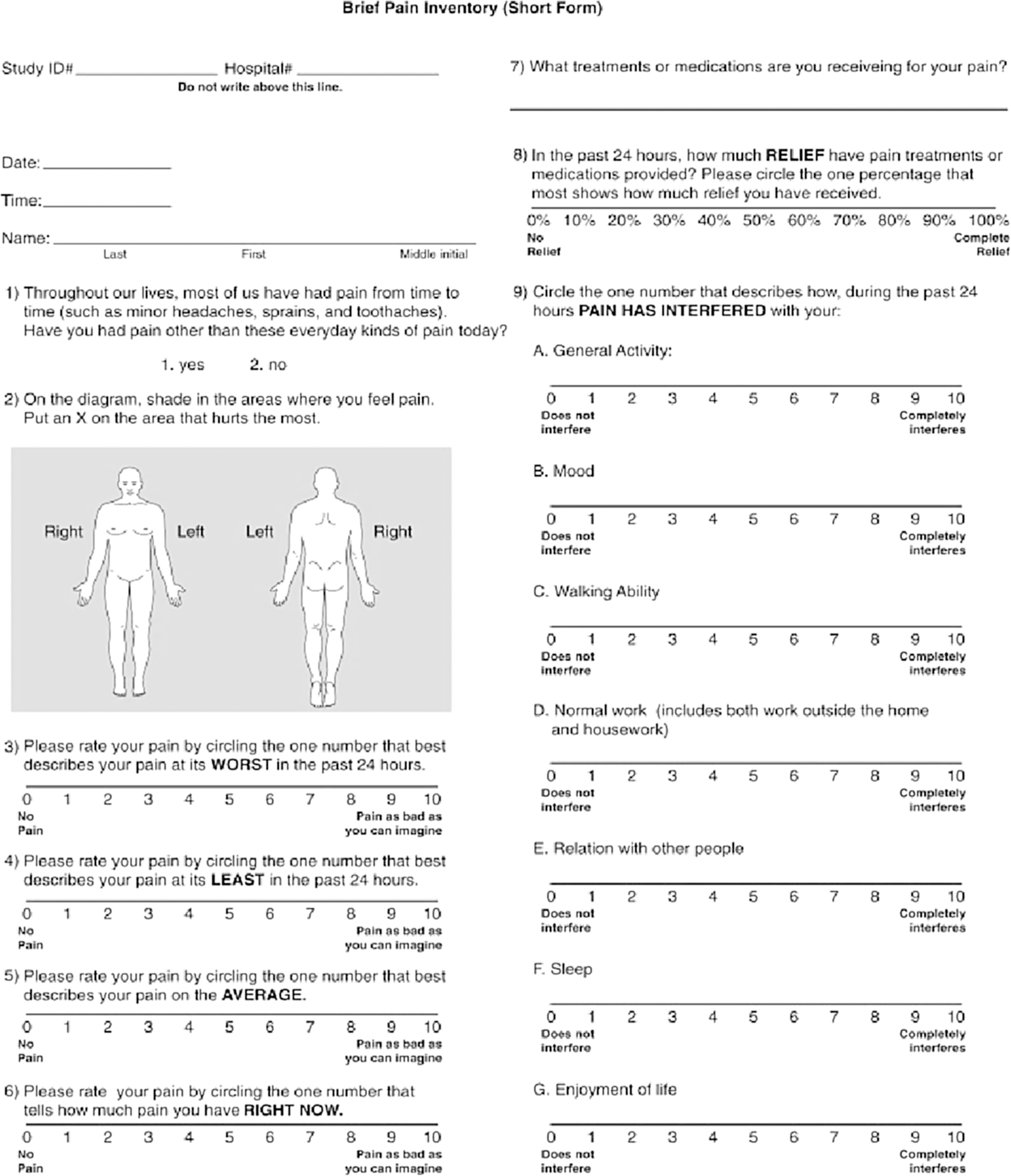
Brief Pain Inventory short form.
Blood tests were performed at baseline and after 6 months of follow-up. Blood 25(OH)D was measured with an immunoenzymatic assay; patients were advised to stop vitamin D supplementation 1 week before the 6-month follow-up examination to avoid measurement bias due to vitamin D assumption immediately before the laboratory test. CK, total cholesterol, high-density lipoprotein cholesterol, and triglycerides were measured with common laboratory kits. LDL-C was determined using Friedewald's formula.
Intervention phase with vitamin D and statin rechallenge
After the first visit, a standard oral cholecalciferol therapy was given to patients at a dose of 25,000 IU once a week for 6 months, up to a total amount of 600,000 IU, which is the annual dose required by an adult person. 32 When clinically indicated, after the vitamin D replacement, causes of hypovitaminosis different from the low solar exposition (malabsorptive, etc.) were evaluated, beyond the study. Patients were not asked to modify dietary habits and physical activity during the follow-up. Vitamin D therapy was added to the patients' baseline therapy, which continued during the entire follow-up period. As stated above, baseline therapy could include the assumption of a low-intensity statin, or could be a statin-free therapy.
Only in a subgroup of participants who were not at the LDL-C target, after examining their cardiovascular status 2 with or without statin therapy, a rechallenge was proposed with the high-intensity statin therapy already assumed by the patient in the past, and then suspended for the appearance of SAMS. During statin rechallenge, the hepatic and renal function was monitored.
Statistical analyses
Continuous variables presented a normal distribution, and non-normally distributed variables were log-transformed before analyses.
Student's t-test or the Mann–Whitney test was used to compare baseline and follow-up data, within and between groups.
The Pearson or Spearman's correlation coefficients were used as appropriate, to determine the correlations between continuous variables in simple and multiple approaches. Multiple regression analyses were performed to test the independent association between muscular pain intensity percentage variation on one side, and sex, age, hypertension, diabetes, obesity, and vitamin D percentage variation on the other side.
A general linear model (GLM) for repeated measures, the Huynh-Feldt test, was used to verify the influence of vitamin D replacement on SAMS intensity changes (pain, life quality indicators) during the follow-up period.
Statistical significance was set at P < 0.05.
Results
The study flowchart is presented in Fig. 1. In a database of almost 3000 patients, only 5.4% (160 patients) had confirmed SAMS. Among SAMS patients who met the inclusion criteria and complied with the study procedures, 26% (15 patients) had normal vitamin D values and were included in the control group, whereas 74% (42 patients) had hypovitaminosis D and were included in the intervention study group.
Among cases at baseline, 46% (19 patients) still tolerated some dosage of low-intensity statins.
During vitamin replacement, 38% (16 patients) were not at the LDL-C target and started a high-intensity statin rechallenge, and 75% (12 patients) of them tolerated the statin increase. Overall, at follow-up, 64% (27 patients) assumed a statin at some dosage. Among 83% (35 patients) who ended the study, the mean follow-up time was 170 ± 10 days.
Features of case and control groups at baseline are presented in Table 1.
Clinical Features, Laboratory Parameters, and Questionnaire Evaluation of Case Group (n = 42) and Control Group (n = 15) at Baseline
AST, aspartate aminotransferase; ALT, alanine aminotransferase; CK, creatine phosphate kinase; GGT, gamma glutamil-transferase; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; LQI, life quality indicators; ns, not significant; TOT-C, total cholesterol.
They were mainly middle-aged males with chronic comorbidities. Clinical and laboratory parameters were comparable, except for vitamin D levels that were significantly higher in the control group, as per the protocol. No new chronic disease, and therefore no therapy change, happened after the 6 months of follow-up, both in the case and in the control groups.
Case group (intervention arm)
The clinical features at baseline and follow-up of the population completing the study are described in Table 2. All patients had myalgias as per the protocol, and 13 (37%) of them also had CK elevations. The maximum baseline CK value was 2386 IU/mL.
Clinical Features, Laboratory Parameters, and Questionnaire Evaluation of 35 Patients with Statin-Associated Muscle Symptoms and Hypovitaminosis D at Baseline and After Vitamin D Replacement
At the follow-up visit, vitamin D significantly increased, reaching 261% of the baseline values, and 24 (68%) patients had normal vitamin D concentrations. The vitamin D increase after replacement was strongly dependent on basal vitamin D levels (r = 0.78, P < 0.0001) in an inverse relationship (Fig. 3).

Scatterplot between vitamin D percentage variation and basal vitamin D levels (r = 0.78, P < 0.0001).
After vitamin D replacement, the pain intensity was reduced by 63% (Table 2), together with improvements in all life quality indicators; pain and its consequences were completely abolished in 11 patients (31%).
Even if no relationships between vitamin D levels and pain intensity were found, both at baseline and in follow-up (data not shown), an inverse relationship was found between percentage variations of SAMS intensity and percentage variations of vitamin D levels at follow-up (r = 0.57, P = 0.002). This association was independent of sex, age, hypertension, obesity, and diabetes in the multiple regression analysis (Table 3).
Multiple Regression Analysis
Dependent variable: muscular pain intensity percentage variation.
Excluded variables: sex, age, hypertension, diabetes, and obesity.
Improvements in the clinical picture of SAMS were progressive during vitamin D replacement (Fig. 4 and Table 4 for the GLM test).
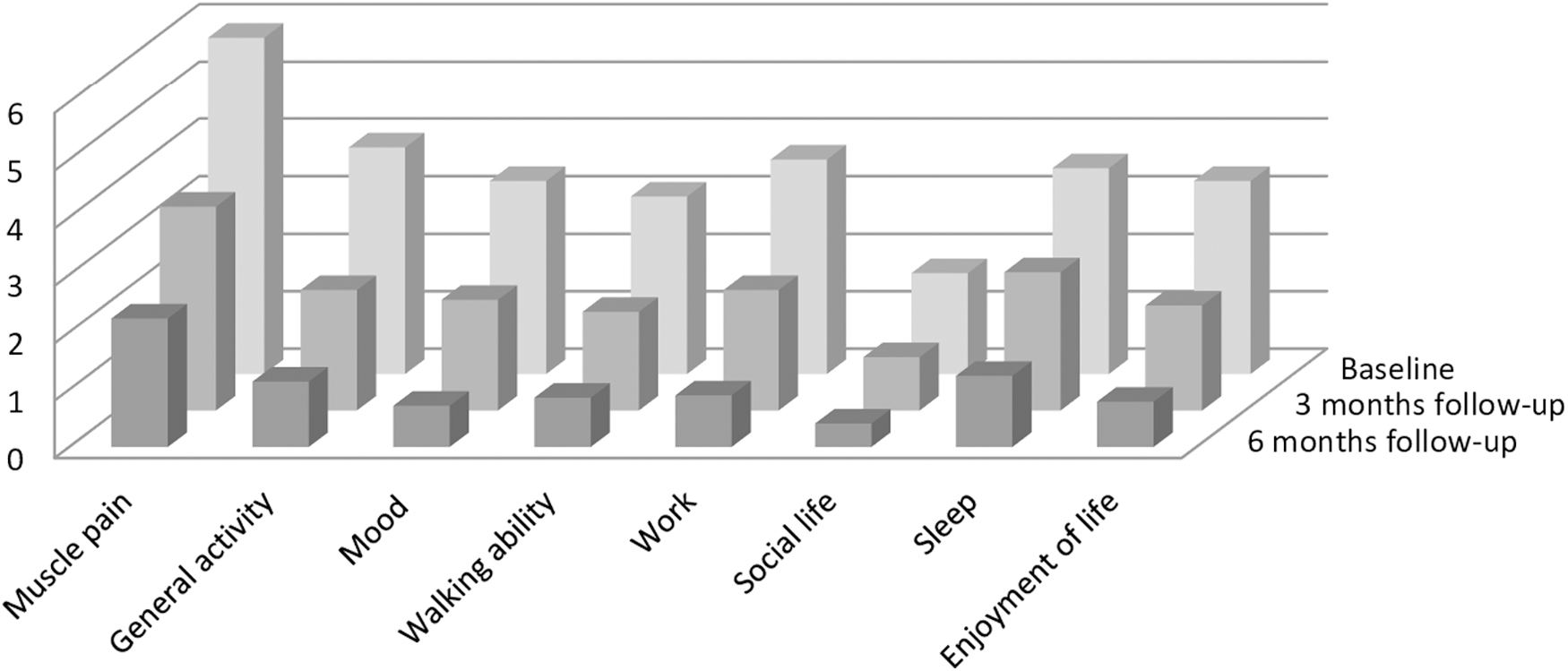
Mean values for muscle pain and life quality indicators at baseline, and at 3 months and 6 months of follow-up (P < 0.05 for all).
General Linear Model Showing the Influence of Vitamin D Replacement on Pain Intensity Values During the Follow-Up Period
Similarly, all indicators of overall life quality, such as daily activities and mood, significantly (Table 2) and progressively (Fig. 4) improved after vitamin D replacement (GLM not shown), and their percentage variations were significantly and inversely related to vitamin D elevations (data not shown).
Length of follow-up, sex, and age were not related to the variations in vitamin D levels or SAMS clinical pictures (data not shown).
Of the 16 (38%) patients who were asked to take their previous high-intensity statins, 12 (75%) successfully accomplished the rechallenge and showed improved lipid values, obtaining a mean LDL-C below 100 mg/dL (Table 5).
Clinical Features of the Rechallenge Subgroup (12 Patients) at Baseline and Follow-Up
Patients not completing their visit schedule were 17% of the cases, and their baseline features were similar to the patients who fulfilled the study time sheet.
Control group
With respect to the intervention group, controls had similar baseline clinical and laboratory parameters. These parameters were unchanged at follow-up (data not shown).
Discussion
The main finding of the study is that an elevation in low blood vitamin D concentrations can progressively relieve muscular and associated lifestyle disturbances, due to statin therapy, and improve statin utilization.
More precisely, to the best of our knowledge, this is the first vitamin D intervention study reporting the clinical quantification of pain and its consequences during SAMS. In fact, in our study, we observed, for the first time, that after vitamin D replacement in hypovitaminosis D conditions, the percentage rise in blood vitamin D concentrations was associated with a percentage regression of reported pain intensity, together with the regression of the negative impacts of pain, on the quality of life of the patients.
However, the impact of vitamin D replacement on muscular symptoms in SAMS patients has already been reported in other studies in the literature. 17,18,34 –36
In previous studies with 6 months of follow-up, resolution of SAMS occurred in 86%–95% of patients. 18,35,36 In Kang et al.'s study, follow-up was longer (12 months), and 100% tolerated statins without complaints after this period. 34 In Ahmed et al.'s study, follow-up was just 3 months, and 92% of patients were free of SAMS at the study end. 17 In contrast to ours and the above reported research, in this last short study, all included patients were on statins, which may suggest only mild statin intolerance.
However, the observed percentage regression of SAMS intensity is not reported in any of the abovementioned studies. There, only the presence or the absence of muscular symptoms was reported, eventually with CK alterations, and this might have discouraged the reporting of even mild symptoms at the follow-up. Furthermore, it is not known whether pain intensity varied or remained unchanged at follow-up in patients who still had myalgias. Regarding the vitamin D dosage used, the total amount in other vitamin D intervention studies was 600,000 IU 17,34 and 750,000 18 administered over 3 months or 1,300,000 over 6 months, 35,36 whereas in our study, it was less (600,000 over 6 months).
For all these reasons, in our opinion, the percentage of patients who had a complete resolution of symptoms in our study (31%) cannot be properly compared with the data in literature.
The vitamin D dose assumed before starting rechallenge (300,000 IU) was equal to other studies, 18,35,36 but the time of assumption was longer in our patients (3 months vs. 3 weeks). Only in Kang et al.'s study, the rechallenge was attempted after a full replenishment of 600,000 IU of vitamin D. 34
The percentage of our patients able to tolerate statin rechallenge at 6 months (75%) was consistent with those reported in literature, ranging from 74% to 100%. 18,34 –36
Regarding SAMS prevalence, it is confirmed to be low, in a lipid clinic setting. In our study, the prevalence of SAMS was ∼5%, similar to the STOMP study, 37 and lower than the prevalence often observed in clinical practice, which ranges from 7% to 29%. 12
Regarding vitamin D levels in SAMS patients, 72% of them who underwent measurements had levels <30 ng/mL, confirming the high prevalence of hypovitaminosis D observed in the literature among statin-intolerant patients. 17,22 Looking at these data in healthy adults, the prevalence of hypovitaminosis D ranges from 14% 23 to 43%. 17
Even if the hypovitaminosis D prevalence among patients suffering from SAMS in Eisen et al.'s study is equal to that in the control group, those results might be due to genetic or geographical factors. In fact, the study was conducted in Israel, where sun exposure is generally high, as proposed by Eisen himself. 24 Another possible explanation is that a selection bias occurred, since the SAMS prevalence among statin-treated patients in the study (39%) was higher than that observed in clinical practice (ranging 7%–29%). 38
In another study, there was no difference in hypovitaminosis D prevalence in the SAMS group, but the control group was composed of people among whom SAMS were not confirmed, but who suffered only from muscular pain of an uncertain origin. 27
Furthermore, SAMS are the main reason for missing LDL-C targets, as commonly observed in clinical practice. 10,11 In the present population with SAMS and hypovitaminosis D, a successful rechallenge by 25(OH)D replacement lowered the mean LDL-C value of 40 mg/dL with respect to baseline levels, helping to reach targets.
Regarding basal vitamin D levels, in the present study, they influenced the response to its replacement, as patients with lower basal 25(OH)D levels had a higher percentage improvement after therapy. This was reported as a negative feedback regulation by serum 25(OH)D concentrations on the vitamin D conversion to 25(OH)D, 38,39 even though the details are still unclear. 40
Therefore, patients who had lower vitamin D levels at baseline, then had better responses in terms of greater reductions in pain intensity and improvements in their quality of life.
None of the abovementioned studies described the impact of SAMS on patient's quality of life. Muscular pain, due to statin intolerance, has a strong influence on the everyday life and mood of our patients, and the improvements in its indicators, measured here, show that vitamin D replacement could be beneficial.
Regarding negative evidence in the literature, some studies do not agree with the existence of a relationship between SAMS and hypovitaminosis D. 24 –28 Despite this evidence, these studies are almost all nonintervention protocols that aimed only to assess the prevalence of hypovitaminosis D among SAMS patients, and/or low vitamin D values as predictors for SAMS incidence. Our study fully agrees with the absence of a relationship between basal vitamin D levels and SAMS intensity.
Even if a large number of investigational or review studies agree with the observation that vitamin D levels are not useful to predict SAMS occurrence, before the beginning of statin therapy, 24 –27,41 some investigations report that very low levels of vitamin D are a risk factor for developing muscle symptoms under statin therapy. 19,42
The only study among those abovementioned, who consider the effect of vitamin D replacement on the success of statin rechallenge, is the study by Compton et al. 28 However, this was a retrospective study that considered a population with higher vitamin D baseline levels than in our study. As above reported, patients with lower baseline blood vitamin D have a higher percentage increase of serum vitamin D, after the supplementation therapy. Moreover, blood vitamin D concentration after the vitamin D replenishment was not measured, and thus, we are not able to know if those patients had a sufficient response to their supplementation therapy.
Taylor et al. suggested that vitamin D deficiency may affect muscle health in general. 27 In fact, CK level variations were inversely related to vitamin D level variations, measured after statin treatment, in both the SAMS and non-SAMS groups. Moreover, even muscle pain complaints in the non-SAMS group increased as vitamin D was reduced. As in our study, pain severity was measured through a clinical scale. In this study, the majority of the population did not have hypovitaminosis D, and only 25% had vitamin D levels <20 ng/mL. Again, a vitamin D replacement was not administered.
Limitations
The present data were derived from a nonplacebo-controlled, monocentric open study. Drug accountability was performed, but based upon patient interviews. These limitations should be accounted into the interpretation of the present results.
Conclusions
The present data confirm that a vitamin D value percentage increase after supplementation is accompanied by a clinical improvement in patients suffering from SAMS, together with a better statin compliance. Furthermore, for the first time, the present study measured the symptom intensities of SAMS, in terms of both pain and quality of life, demonstrating that they all improve, more when higher percentage elevations in vitamin D concentrations are reached. This was more often recorded in severe baseline hypovitaminosis. However, these data need further investigation with double-blinded, placebo-controlled, and randomized studies.
In the meantime, from a clinical point of view, regarding the lowering of cardiovascular risk, it seems reasonable that 25(OH)D is measured in all patients suffering from SAMS, and if below 30 ng/mL, proper vitamin D integration should be prescribed, as indicated in the hypovitaminosis D guidelines. 34 Then, if the patient was not at the LDL-C target at baseline, a (high-intensity) statin rechallenge could be attempted as early as 3 months after the vitamin D assumption.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.