
Abstract
Background:
Settings-based approach has received lot of attention under WHO renewed strategy of health promotion. It advocates regular screening/health check-ups of employees to maintain a healthy workplace. This study aimed to assess prevalence of metabolic syndrome (MetS) among faculty members and its association with selected sociodemographic, behavioral and biochemical parameters, and to determine the 10-year fatal or nonfatal cardiovascular risk using WHO-ISH risk chart.
Methodology:
A cross-sectional study was conducted among 252 teaching faculty members using standardized international protocols to measure behavioral risk factors (smoking, alcohol consumption, diet pattern, physical activity, sleep, and stress), physical characteristics (weight, height, waist and hip circumferences, and blood pressure), and biochemical parameters (fasting glucose and lipid profile). Risk factor profiling was done using WHO/ISH risk prediction chart.
Results:
Among 252 participants (males: 172 and females: 80), 58 (24.1%) were with MetS. Prevalence was higher in males (24.6%) than females (22.6%). The younger doctors (≤40 years) had lesser prevalence of MetS compared with the elderly (>40 years) doctors (20.3% vs. 26%). Age and diet pattern were found to be independently associated with MetS. The risk of having a cardiovascular event in 10 years was <5% (low risk) for 87.5% of study participants.
Conclusion:
Although we included doctors who are probably the most health-conscious population, we have found that one in four have a chance of having MetS. There is a need for periodic screening program and lifestyle modification strategies to control the burden of MetS among doctors.
Introduction
Metabolic syndrome (MetS) is characterized by interlinked clinical, physiological, metabolic, and biochemical factors that directly tend to increase the risk of cardiovascular diseases (CVDs) and associated mortality. 1 MetS is defined as a cluster of the presence of at least three out of five cardiometabolic abnormalities that occur together. These abnormalities are abdominal obesity, hypertension, hyperglycemia, hypertriglyceridemia, and low high-density lipoprotein (HDL) cholesterol. 2 It is not clear to what extent these components differ across populations and ethnic backgrounds.
MetS has been defined based on different criteria like International Diabetes Federation (IDF)/Adult Treatment Panel (ATP) III/AHA/NHLBI criteria. 3 Around 12%–37% among the Asian population and 12%–26% among the European population tend to suffer from MetS. 4
A recent multiethnic population-based survey reports that the highest prevalence of MetS is seen in Indian ethnicity. 5 Various population-based studies were conducted in India and the results of studies are varying between 10% and 50%. 6,7 The variations in prevalence could be attributed to the adoption of different criteria for MetS, study settings, laboratory techniques, and risk factors. MetS is affected by factors such as age, gender, ethnicity, and occupation. A recent study had also shown that the prevalence of MetS varies between different occupational groups. 8
Health care providers particularly doctors are an important segment of society and have better access to information on the disease and its determinants. However, doctors operate in a very stressful working environment and put patient's health before their health. It is very important to be aware and look after their health. Many studies done among doctors have shown an increased prevalence of chronic diseases besides being aware of this condition. 9 –12
The prevalence of MetS worldwide among health professionals are varying between 4% and 45% from various studies. 13 –15 A study data confirms that the doctors in India have MetS of around 30% in both men and women. 16
Settings-based approach advocates regular screening/health check-ups of employees to maintain a healthy workplace. 17 Thus, if Physicians are motivated to a healthy practice and living, it would motivate the public to lead a better lifestyle. 18 Data from studies suggest that health care workers, especially working doctors and faculty members, are prone to sleep quality getting affected, and developing mental health problems, such as depression, anxiety, and stress. 19,20 The WHO ISH SEAR D charts help in estimating the level of CVD risk factors and WHO had recently updated the CVD risk charts based on newly validated risk prediction models in 2019. 21
There is a paucity of data on various lifestyle-associated disorders among doctors in low and middle-income countries. 20,22 Although few studies are available among doctors, the studies are mainly done among the floating population like conference attendee and facility-based studies, including the undergraduate, postgraduate students, and other health care workers. The importance of sleep and stress in the development of lifestyle disease should also be explored, but the few available studies have failed to evaluate these aspects concerning MetS. Hence this study was carried out to assess prevalence of MetS among faculty members and its association with selected sociodemographic, behavioral, and biochemical parameters and to determine the 10-year fatal or nonfatal cardiovascular risk using WHO-ISH risk chart.
Methodology
Study setting
This cross-sectional analytical study was conducted in JIPMER, Puducherry from January 2019 to March 2020. JIPMER is a 2350-bedded tertiary care hospital with a staff strength of about 5000 with more than 2000 undergraduate and postgraduate students in all streams and 350 faculty strength, of which 326 are teaching medical faculty. JIPMER is well known for its teaching, research, and free patient care in the area of health.
Sample size
We included all 255 teaching Faculty members in JIPMER at the time of the study.
Study procedure
The study was done over a period from January 2019 to April 2020. The study tool used was a semistructured questionnaire involving various domains like sociodemographic details, behavioral habits, diet, physical activity, anthropometric measurements, and laboratory investigations. Cohen's Perceived Stress Scale (CPSS) was used for assessing the stress level of the individual and the Pittsburgh Sleep Quality Index (PSQI) for assessing sleep quality. Behavioral habits, including tobacco, alcohol use, diet, and physical activity were measured based on WHO STEPwise approach to surveillance questionnaire (STEPS). 23
The anthropometric measurements include height, weight, blood pressure, waist circumference and hip circumference, and was measured using WHO guideline. 24 Laboratory investigations like fasting plasma glucose levels, total cholesterol, triglyceride level, low-density lipoprotein cholesterol level, and HDL cholesterol levels were measured.
Risk factor profiling of the staff was done using WHO/ISH risk prediction Chart. 21 WHO/ISH risk prediction charts indicate 10-year risk of a fatal or nonfatal major cardiovascular events (myocardial infarction or stroke), according to age, gender, blood pressure, smoking status, total blood cholesterol, and presence or absence of diabetes mellitus. The charts provide approximate estimates of CVD risk in people who do not have established coronary heart disease, stroke, or other atherosclerotic disease. Ethics approval was obtained from the Institutional Ethics Committee, JIPMER. Written informed consent was obtained from participants before recruitment.
Data collection
Department-wise list of faculty members was prepared after obtaining the list of faculty members working in JIPMER from the administration section. Fields that contain personal identification details of the study participants were made optional. The first contact was to know their willingness to participate, and for explaining the study details. Upon expressing willingness to participate, written informed consent was obtained, and the self-administered questionnaire was physically handed over or mailed to the participants.
Two times in a week during any time of the day was spent on collecting sociodemographic characteristics, behavioral habits, dietary patterns, physical activity, and anthropometric measurements. The participant's anthropometric measurements and blood pressure was measured on the same day as per the WHO STEPS protocol. They were informed about the fasting blood sample collection for the next day morning.
Operational definitions
Physical activity was assessed based on WHO STEPS questionnaire regarding physical activity duration at work, travel to places, and recreation activities where 150 min of moderate-intensity physical activity or 75 min of vigorous-intensity physical activity per week was considered as adequate. 23 Current tobacco user was defined as tobacco use in any form within the past 1 month of data collection. 25 Current alcohol user is termed as alcohol use of any type within the past 1 year of data collection. 26 Adequate healthy diet was defined as consumption of at least one serving of fruits and one serving of vegetables per day for 5 days a week. 27 CPSS is the most widely used global scale, which is self-reported to assess the perceived psychological stress status.
This 10-item scale consists of questions which include both positive and negative aspects of stress. Based on the overall score, the stress level was classified as Low (score: 0–13), Moderate (score: 14–26), and High (score: 27–40). 28 PSQI questionnaire was used to assess sleep quality over the last 30 days. If the total global PSQI score is <5, then the participants will be reported to have good sleep quality. 29 To overcome the overestimation or underestimation of the participant's responses, the participants were explained clearly about the questions and the responses were taken.
Statistical analysis
Data were entered into Epicollect 5 software 30 and analysis was done using STATA version 14.3. 31 The independent variables like age were summarized as mean [standard deviation (SD)]. The categorical variables like gender, diet pattern etc. were summarized as percentages.
The prevalence of MetS was summarized as percentage with 95% confidence interval (CI). The association between each of the independent variables (gender, family type, diet, family history of diabetes mellitus and hypertension, tobacco use, and alcohol use) with MetS was assessed using log-binomial regression and expressed as prevalence ratio with 95% CI. P value <0.05 was considered as statistically significant. The variables statistically significant in log-binomial regression was considered for multivariate logistic regression
WHO-ISH risk chart, both laboratory and office-based chart was used to predict 10-year fatal or nonfatal cardiovascular risk, which was categorized as <5%, 5% to <10%, 10% to <20%, 20% to <30%, and ≥30% and summarized as percentages.
Results
In this hospital-based cross-sectional study, we ended up interviewing 252 study participants out of 255. Self-reported biochemical parameter values, done within 6 months before data collection, were obtained from 65% of the participants.
The mean (SD) age of the study participants was 43 (7). Almost half of the study participants, 94 (37.3%), were in age group of less than or equal to 40 years. The majority of the study participants, 172 (68.3%) were men, 242 (96%) were currently married, 182 (72.6%) were belonging to nuclear family, and 231 (91.7%) belonged to Hindu religion (Table 1).
Sociodemographic Distribution and Behavioral Characteristics Among Study Participants in a Tertiary Care Hospital, Puducherry (N = 252)
Widowed/Widower, Never Married, Separated/Divorced.
At least five servings of fruits and vegetables per day.
150 min of moderate-intensity physical activity or 75 min of vigorous-intensity physical activity per week.
PSQI.
Cohen Perceived Stress Scale.
PSQI, Pittsberg Sleep Quality Index.
One-third of the study participants, 95 (37.7%), had ever used alcohol in the past of their lifetime, and 39 (15.4%) consumed alcohol in the past year. Among current alcohol users more than three fourth of them, 31 (79.5%) subjects, were using alcohol monthly once. The median [interquartile range (IQR)] number of occasions was 6 (3–12) days in the past 30 days. Around 16 (6.3%) participants had ever used tobacco in their lifetime. Of the study participants, 6 (2.3%) were current tobacco users in the past 1 month. There were no current female alcohol or tobacco users.
Two hundred eleven (62.3%) were following a healthy diet pattern with 76 (30.1%) having a history of added salt in the diet. Consuming fast food was observed in 119 (47.2%) participants. The median (IQR) number of days of fast food consumption was 2 (1–3) days in a week.
Nearly half of the study participants, 122 (48.4%), had adequate physical activity, 206 (81.7%) participants were having an adequate quality of sleep according to the PSQI. The mean duration of sleep hours among the study participants was 6.7 ± 0.7 hr. The median PSQI score among the study participants was 3 (2–4). Around one-third of the study participants, 94 (37.4), were having moderate stress according to the Cohen Perceived Stress Scale. The median Cohen Perceived Stress score among the study participants was 12 (9–16).
Considering the comorbid conditions, 54 (21.4%) and 19 (7.5) were having only hypertension or diabetes. Seventy-four (29.3%) subjects had a family history of noncommunicable diseases. According to Asian Pacific classification, 153 (60.7%) were obese and 82.5% of the study participants belonged to the overweight/obesity category.
The overall prevalence of MetS among faculty members in a tertiary care hospital, Puducherry during 2018–2019 was 24.1% (95% CI: 18.9%–29.7%). A total of 86 (35.9%) had only two components of MetS. However, only one participant (0.4%) had all five components (Tables 2 and 3).
Prevalence of Metabolic Syndrome Among Study Participants in a Tertiary Care Hospital, Puducherry During 2018–2019 (N = 241)
NCEP ATP III SAS, 2009 criteria.
ATP, Adult Treatment Panel; CI, confidence interval; NCEP, National Cholesterol Education Program.
Distribution of Components of Metabolic Syndrome Among the Study Participants in a Tertiary Care Hospital, Puducherry (N = 241)
NCEP ATP III SAS, 2009 criteria.
HDL, high-density lipoprotein.
Individuals who were more than 40 years of age [unadjusted prevalence ratio (PR) = 1.85, 95% CI: 1.12–3.14, P = 0.02], with inadequate physical activity levels (unadjusted PR = 1.65, 95% CI: 0.74–4.44, P = 0.18), and unhealthy dietary habits (unadjusted PR = 2.4, 95% CI: 0.91–6.42, P = 0.07) had increased proportion of having MetS when compared with individuals of age less than or equal to 40 years, adequate physical activity, and healthy diet pattern, respectively (Table 4).
Association of Sociodemographic and Behavioral Characteristics with Metabolic Syndrome Among Study Participants in a Tertiary Care Hospital, Puducherry During 2018–2019 (N = 241)
Alcohol use in past 1 year.
Tobacco use in the past 1 month.
150 min of moderate-intensity physical activity or 75 min of vigorous-intensity physical activity per week.
At least five servings of fruits and vegetables per day.
PSQI.
Cohen Perceived Stress Scale.
Asian Pacific BMI criteria.
BMI, body mass index.
Using the variables that became significant considering P < 0.2 in the univariate analysis, multivariate analysis was performed. We see that the final model has three independent variables, of which two contribute significantly to the outcome. The predictors for MetS was age more than 40 years [adjusted PR (aPR) = 1.57, 95% CI: 1.13–3.11, P = 0.005] and diet pattern (aPR = 1.88, 95% CI: 1.04–4.21, P = 0.01), which were statistically significant after adjustment for physical activity (P < 0.05) (Table 5).
Multivariate Analysis for Association of Sociodemographic and Behavioral Characteristics with Metabolic Syndrome Among Study Participants in a Tertiary Care Hospital, Puducherry During 2018–2019 (N = 241)
At least five servings of fruits and vegetables per day.
150 min of moderate-intensity physical activity or 75 min of vigorous-intensity physical activity per week.
Figure 1 illustrates the distribution of 10-year cardiovascular risk prediction among Faculty members in a tertiary care hospital, Puducherry during 2018–2019. In this study, participants <40 years have been assessed assuming the risk for them to be at 40 years in the chart. The risk of having a cardiovascular event in 10 years was only <5% (low risk) for 87.5% and 89.2% of study participants based on laboratory-based and office-based charts. Four (1.8%) and 2 (0.9%) had a risk of 10%–20% (moderate risk) based on the charts, respectively. The kappa statistic agreement between two risk scores was found to be 93.4%, with kappa value to be 0.68 (P < 0.001).
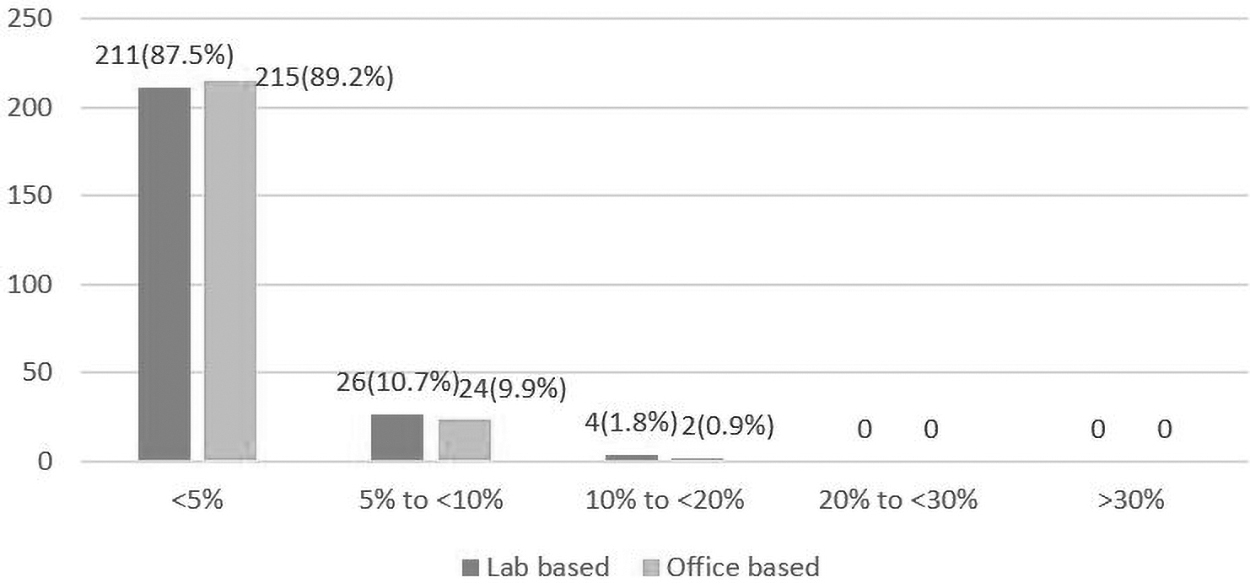
Distribution of 10-year cardiovascular risk status based on the WHO-ISH risk prediction chart 2019 among study participants in a tertiary care hospital, Puducherry, N = 241. The X-axis represent the cardiovascular risk percentage while Y-axis represent the number of persons. The dark gray bars represent the risk assessed using laboratory-based charts, which includes cholesterol levels and the light gray bars represent the risk assessed using office-based charts, which includes BMI. BMI, body mass index.
Discussion
The prevalence of MetS among faculty members was 24.6% in the current study. The prevalence of MetS among doctors and other health care professionals from various studies done worldwide ranges between 5% and 40%. 13,16,22,32,33 Considering a study done by Manjareeka et al. in Bhubaneshwar, in a tertiary care medical college among doctors, showed a higher prevalence of MetS (36%) compared with our study, which might be due to physical activity promoting a working environment in JIPMER and recruitment of young faculty members in our setting. 22 The involvement of faculty members in various sports events by JIPMER had promoted the health of faculty members. JIPMER Quality Council (JQC) involvement in promoting various health-related activities among employees had helped in improving their lifestyle in the workplace.
While looking at some studies done in Southeast Asian countries like Iran (18.90%) and Pakistan (18.56%), they showed a prevalence of MetS to be at a lesser level, the reason being the involvement of resident doctors in their study who are younger than faculty members with lesser comorbidities. Looking at the global level, studies that were done in other countries like Italy (7.1%), Turkey (6.1%), and Brazil (4.5%) among doctors have shown very less prevalence of MetS, as foreign studies state that physicians maintain very good health habits like healthy lifestyle, increased physical activity, and their living standards are improved due to higher economic standards compared with Indian physicians and the development status of those countries. 33,34
Prevalence data of MetS observed among the general population in studies from the North (25.6%), East (31.4%), West (19.5%), and South India (24.8%) were mostly similar to this study. 15,16,35,36 In contrast, results of a study have shown that the prevalence of MetS among doctors was more common than the general population, which may be attributed to a difference in the age (18–80 years) and gender distribution of study participants. In this study, although a comparison with the general population has not been done, looking at results from an unpublished previous study conducted in urban adults of Puducherry, which is a similar setting, showed a higher prevalence of MetS (38.3%).
Doctors have better medical knowledge, higher disease awareness, and easier health care access and are more aware of the avoidable risk factors, which may be a reason for lesser prevalence among doctors in this setting. As health care workers present with better knowledge regarding healthy practices, they are expected to have lesser prevalence of MetS than general population.
The current study showed that the prevalence of MetS was one and half times more (aPR = 1.57) among participants above 40 years of age when compared with those less than or equal to 40 years. The study done in Nigeria reported similar strength of association (adjusted odds ratio = 1.2) among individuals 40 years of age and more. 37 Trends of increasing prevalence of MetS with increasing age were reported in other studies among health care professionals as the elderly are at a higher risk for developing comorbidities, including CVDs. 14,37 Considering our study, faculty are usually recruited at a younger age here and a major proportion belongs to age <40 years.
The present study showed that the majority of the study participants (68.3%) were males. A similar distribution of gender was observed by the studies done by Manjeereka et al., Ramachandran et al., and Mathavan et al. among doctors in India. 16,22,32 Our study showed that there is no significant gender difference in the prevalence of MetS. However, our findings were supported by studies conducted among doctors, which show males having a higher prevalence than the females. 16 Lower prevalence of MetS in our study might be due to higher health consciousness among female doctors and the protective effects of endogenous estrogens, as more women in the study were below the average age of menopause in India (46.2 years). 38
Our study showed that 67.8% of users had a healthy diet pattern and those having an unhealthy diet pattern were having 1.80 times more risk for MetS. A study done by Hegde et al. showed a higher prevalence of unhealthy dietary patterns among health care workers in a tertiary care hospital in Tamilnadu. 39 This difference may be due to the inclusion of other health care workers in the study who are less likely to follow healthy dietary patterns. The diet pattern of this study was assessed by a scoring system described by Deb and Dasgupta, 40 while our study followed the WHO STEPS questionnaire which will provide a more accurate estimate.
According to Physicians Health Study 2007, 40% of doctors were overweight and 23% were obese. 41 Our study has shown an increased proportion of overweight and obesity (60.7%), which might be owing to the different study setting, criteria used for the classification of body mass index, and sedentary lifestyle.
Occupational risk factors like loss of sleep due to shift work and stress are linked to MetS. 42 Our study demonstrated that more than one-third of the study participants (37.4%) had moderate stress but was not significantly associated with the risk of MetS. However, studies done in North India and Brazil among doctors with higher stress levels have a four-fold to six-fold greater risk of being affected by MetS than doctors with lower levels of stress. 33,43 The study done in North India has shown 67% of doctors have moderate stress. This may be due to a difference in the study setting and characteristics of the study population. Faculties in our study working in a tertiary care hospital like JIPMER are in permanent job positions and a comfortable working environment for job satisfaction may be the reason for the prevalence of low stress levels.
A study done among doctors in Brazil has shown that around 60% of the doctors had poor quality of sleep, but was not significant. 43 This difference may be due to the involvement of resident doctors in the study. Our study showed that the mean score of PSQI (3.00) was below the limits recommended by Buysse et al., 29 indicating good sleep quality. Shift-work is frequently described to be associated with sleep disorders, although we have not looked into that aspect in this study.
Our study has assessed the prevalence of MetS based on NCEP ATP III criteria, which is most commonly used. A study done in Madurai among both practicing and teaching physicians showed a higher prevalence, as the criteria used for assessing MetS was IDF criteria, which tends to show a higher prevalence compared with NCEP ATP III criteria. 32 ATP III defines a person as having MetS when three or more risk factors are present, whereas the IDF criteria require two or more risk factors in the presence of increased waist circumference. A study comparing different definitions of MetS has shown that the performance of the ATP III/MetS was superior to the IDF-MetS score for Asians. 3
Ten-year CVD risk using WHO-ISH chart
No studies assessing the 10-year cardiovascular risk using WHO-ISH risk chart 2019 among physicians are available, while studies among the general population can be found. A study done in Bangladesh has shown that the majority of adults (85.2%) have a 10-year CVD risk of <10%. 44 The proportion of adults with a 10-year CVD risk of ≥20% was 0.51%. This study shows a similar result to our study. Studies from a rural area of South India revealed that 17% of participants had moderate-to-high risk (10% to ≥20%), indicating a higher prevalence in the general population. 45,46
In the present study, it was seen that as the age increases the risk of CVD increases. This denotes that the majority of our study participants are in the younger age group and are more health conscious leading to most of them having a lesser risk for CVDs at present. Although studies are not available comparing laboratory-based and office-based WHO ISH risk charts, the agreement between laboratory-based methods and non-laboratory-based methods have been shown to have moderate-to-good agreement. 47
The strengths of the study involved privacy and anonymity during data collection, standard questionnaires like WHO STEPS, Cohen perceived stress scale, and PSQI was used and prevalence ratio was used for assessment to avoid overestimation of association. Limitations included Social desirability bias that might have affected the ascertainment of behavior characteristics like tobacco use and alcohol use, but we have tried to reduce this, by maintaining confidentiality and anonymity during data collection. The study participants are working in a tertiary care hospital, which is an Institute of National Importance. Thus, it may be difficult to generalize the findings to faculties in other hospitals, which may not have a similar kind of setting and facilities.
Conclusion
The current study showed that one in four doctors have MetS. So routine screening of doctors regularly must be ensured. Doctors with increased age, inadequate physical activity, moderate-to-high stress, and having an unhealthy diet pattern had more risk for MetS. First, they should be targeted as they need additional attention and adopt appropriate methods of lifestyle modification. Creating conducive environments for engaging in physical activity like the use of stairs than elevators, using a bicycle as a mode of transport, and availability of healthy foods in campus canteens are necessary to promote behavioral change, which will benefit this working population.
Footnotes
Author Disclosure Statement
The authors have declared that no conflict of interests exist between them.
Funding Information
No funding was received for this study.