
Abstract
Background:
To assess and compare the cardiometabolic risk profile of the Pakistani population between younger (<45 years) and older adults (≥45 years).
Methods:
This is a substudy of a nationally representative community-based epidemiological second National Diabetes Survey of Pakistan (NDSP) 2016–2017. Out of 12,486 individuals approached, 10,834 participants agreed to be included (response rate 87%). Cardiovascular risk factors assessed were obesity, central obesity, hypertension, diabetes, hyperlipidemia, and tobacco use. Participants were stratified into young adults (<45 years) and older adults (≥45 years) and was subcategorized into four groups that is, diagnosed diabetes mellitus (DM), undiagnosed DM, prediabetes, and without diabetes.
Results:
Around 14.3% were prediabetes, 8.8% were undiagnosed DM, and 24% were diagnosed diabetes. Most participants in dysglycemic (prediabetes, undiagnosed DM, and diagnosed DM) groups were females and were from rural regions. Cardiovascular disease (CVD) risk factors were more noted in dysglycemic states, compared with without diabetes. Overall CVD risk profile was worse in males in both age categories, although the accumulation of four or five CVD risk factors at one point was more predominant in females in either age group.
Conclusion:
Overall, the preponderance of CVD risk factors, such as overweight, obesity, central obesity, tobacco use, ex-tobacco uses, and dyslipidemia, were substantially more prevalent in dysglycemia groups of young adults (<45 years) compared with older adults (≥45 years). Early and targeted intervention in young may prevent poor CVD outcomes as they age.
Introduction
Cardiovascular diseases (CVD) remain the leading cause of morbidity and mortality globally and are a serious public health concern in lower-middle-income countries. 1,2 According to World Health Organization (WHO), South Asian and Middle East region is facing an epidemic of CVD risk due to increased urbanization, sedentary lifestyles, increasing life expectancies, and unhealthy food and tobacco consumption. 3,4 These concerns were reflected in Prospective Urban and Rural Epidemiology (PURE) study from 21 countries, wherein two-thirds of CVDs are attributable to a small cluster of modifiable risk factors. 5 Cardiometabolic risk factors may have synergistic and additive effects, increasing the risk for adverse health events.
Amid well-documented contributing risk factors for CVDs, dysglycemia, hypertension (HTN), dyslipidemia, obesity, high abdominal girth, and use of tobacco have risen tremendously in Pakistani inhabitants. It could contribute to further rise in the burden of CVDs. 3,6
The increase in cardiometabolic risk factors in young adulthood, working-age population, are particular areas of concern for Pakistan. South Asians have shown to acquire CVD risk level equivalent to Caucasians and Chinese population almost 10 years earlier. 7 Young adults with CVD risk factors are at increased risk of coronary heart disease later in life, and even borderline levels of these risk factors are associated with atherosclerosis that progress in adulthood. 8 Similarly, increased early-onset type 2 diabetes is of great concern, as prolonged exposure to dysglycemia results in an incremental risk for organ damage and CVD-related morbidity and mortality. 9,10 Accordingly, numerous guidelines now recommend universal screening for HTN and hyperlipidemia in children and adolescents. 11
Studies from local data have reported a high prevalence of cardio metabolic disease in the general Pakistani population in 1990s. 12 This is supported by literature, suggesting high prevalence (27%) of CVDs particularly among Pakistani adults 40 years or older compared with other South Asian populations. 13 More recent findings denoted Pakistani women of a young age may also have an unexpectedly high risk. 14 However, we lack evidence of cardiometabolic risk factors in patients with and without dysglycemia in a general population of Pakistan. Although the prevalence of CVDs has increased recently, yet the prevalence of CVDs implicating to dysglycemia in young and older adults needs further attention. Using the data from the second National Diabetes Survey of Pakistan (NDSP) 2016–2017, we estimated the distribution of CVD risk factors concerning various degrees of dysglycemia.
We also compared relative differences in cardiometabolic risk factors among young versus older adults. It recognizes variation in disease prevalence in the general population of Pakistan.
Methodology
Sample population
We used the data from the Second Epidemiological National Diabetes Survey of Pakistan with participants been enrolled from all four provinces between the period of February 2016 and August 2017. 6 In brief, each province was considered as a stratum and districts (geographical subdivision of provinces legally described by the government) considered as clusters selected from each stratum. Tehsils or towns (further bifurcation of districts legally described by the government) are considered as subclusters. Clusters and subclusters were randomly selected using probabilities proportional to size technique, and number of clusters were selected from each province using “rule of thumb” number of clusters (k) = (sample size of stratum/2)^0.5. 6
Twenty-seven clusters of 213 were included. Of the 46 subclusters, 21 from urban and 25 from rural regions were included.
Out of 12,486 individuals approached, 10,834 participants agreed to be included in the study (response rate 87%). An analytical sample was categorized into four groups that is, diagnosed diabetes (self-reported), undiagnosed diabetes mellitus (DM), prediabetes, and without diabetes residing in rural or urban areas. Participants were also categorized into young adults (<45 years) and older adults (≥45 years).
Inclusion and exclusion criteria
All Pakistani people 20 years of age or above were included in the survey, yet pregnant women, type 1 DM participants, and nonresidents of selected households were excluded from the study.
Definition of diabetes
Undiagnosed DM was defined as fasting plasma glucose (FPG) level ≥126 mg/dL or 2-hr post glucose level (2-hr PGL) ≥200 mg/dL or both. Prediabetes was defined as FPG level between 110 and 125 mg/dL and 2-hr PGL ≥140 mg/dL but <200 mg/dL or both, respectively, for diagnosis (WHO Criteria). Participants with FPG <110 mg/dL and 2-hr PGL <140 mg/dL were called without diabetes. Diagnosed diabetes was categorized as self-reported diabetes or already diagnosed by a physician or taking any antidiabetic medication. 6 Dysglycemia is a combined term used for prediabetes, diagnosed, and undiagnosed diabetes.
CVD risk factors
Each participant was interviewed and a structured questionnaire was completed by a trained interviewer to obtain data on social, anthropometric, and biochemical CVD risk factors. The factors assessed were tobacco use, waist circumference, body mass index (BMI), blood pressure, and dyslipidemia. 6
Current tobacco users were defined as any form of tobacco use without quantification of amount and duration of use within 3 months from time of data collection, whereas used tobacco before 3 months and those who never used tobacco were categorized as ex-addict and nonusers, respectively. 15 Obesity was defined as BMI of 25 kg/m2 or higher for both males and females with or without abdominal obesity as explicated by WHO Asia Pacific Guidelines. 6 Central obesity (abdominal obesity) was calculated from the waist circumference of ≥90 and ≥80 cm in males and females, respectively. 6 Known HTN was defined as a self-reported diagnosis, based on the history of medications for blood pressure control. Newly diagnosed HTN was defined as raised systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg on two occasions for 15 min apart. 6
Dyslipidemia was classified as serum cholesterol >200 mg/dL or low-density lipoprotein cholesterol (LDL-C) >130 mg/dL or high-density lipoprotein cholesterol (HDL-C) <40 and <50 mg/dL for male and female, respectively, and/or triglycerides >150 (mg/dL). 6
Ethics approval
Ethics approval obtained from the National Bioethics Committee of Pakistan remained the same as in the second NDSP (2016–2017). Informed written consent was acquired from each subject before blood sample collection.
Statistical analysis
Data were analyzed by Statistical Packages for Social Sciences (SPSS) version 20. Results were given as median (interquartile range), number (percentage), or percentage [95% confidence interval (CI)]. Normailty of the data was checked by Kolmogorov–Smirnov test. Mann–Whitney U test and two-population proportion test were used to examine the differences in parameters among groups. Multivariate logistic regression models analyzed the association of cardiometabolic risk factors with age, adjusted for gender, marital status, education, diabetes, HTN, obesity, central obesity, tobacco use, and dyslipidemia. A probability value less than 0.05 was considered to be statistically significant.
Results
Diabetes Status of population and its associated factors in Young and Old Groups
Of 10,834 participants, 1547 (14.3%) had prediabetes, 950 (8.8%) had undiagnosed diabetes, 2600 (24%) had diagnosed diabetes, and 5737 (53%) were without diabetes. Undiagnosed diabetes and diagnosed diabetes were higher in ≥45 years than those without diabetes Most participants in prediabetes, undiagnosed diabetes, and known diabetes groups were females and from the rural areas of Pakistan. Statistically significant difference for BMI, systolic/diastolic blood pressure, family history of diabetes, glycated hemoglobin, and lipid profile in prediabetes, undiagnosed diabetes, and diagnosed diabetes groups (Table 1).
Baseline Characteristics, Anthropometric Measurements, and Biochemical Parameters of Pakistani Population on the Basis of Diabetes Status
Data presented as median (IQR) or n (%).
Significantly different from without diabetes.
Significantly different from prediabetes.
Significantly different from undiagnosed diabetes.
Diabetes was defined as FPG level ≥126 mg/dL or 2-hr PGL ≥200 mg/dL or both, prediabetes was defined as FPG level between 110 and 125 mg/dL and 2-hr PGL ≥140 mg/dL but <200 mg/dL or both.
2-hr PGL, 2-hr post glucose level; BMI, body mass index; DM, diabetes mellitus; FPG, fasting plasma glucose; IQR, interquartile range; SD, standard deviation; TG, triglycerides.
CVD risk factors by diabetes status
Table 2 indicates most CVD risk factors, such as known HTN, newly diagnosed HTN, obesity, central obesity, and dyslipidemia, were higher among people with diagnosed diabetes, intermediate among those with undiagnosed diabetes or prediabetes groups, and lowest in the without diabetes group. The most notable variation in HTN with other groups was seen for known diabetes. Percentage [% (95% CI)] was noted as [46.7 (44.7–48.7)] with known HTN, compared with other groups. Persons with undiagnosed diabetes had slightly higher levels of newly diagnosed HTN [28.1 (25.2–31.5)] followed by prediabetes [26.5 (24.2–28.8)], diagnosed diabetes [25.6 (26–29.5)], and people without diabetes [20.4 (19–21)]. Prediabetes populations were most overweight, whereas obesity and abdominal obesity were rising with the degree of dysglycemia, most noticeable in diagnosed diabetes population.
Cardiometabolic Risk Factors by Diabetes Status
Data presented as % (95% CI).
Significantly different from without diabetes.
Significantly different from prediabetes.
Significantly different from undiagnosed diabetes.
Diabetes was defined as FPG level ≥126 mg/dL or 2-hr PGL ≥200 mg/dL or both, prediabetes was defined as FPG level between 110 and 125 mg/dL and 2-hr PGL ≥140 mg/dL but <200 mg/dL or both.
Newly diagnosed HTN: systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg; Known HTN: previous history of HTN; Obesity: BMI ≥25 kg/m2; Central obesity: Waist circumference ≥90 and ≥80 cm in males and females, respectively; Dyslipidemia: serum cholesterol >200 mg/dL or serum LDL-C >130 mg/dL or serum HDL-C <40 and <50 mg/dL for male and female, respectively, or serum TG >150 (mg/dL) or taking any lipid-lowering medications; Current tobacco users were defined as any form of tobacco use without quantification of amount and duration of use within 3 months from time of data collection, whereas used tobacco before 3 months and those who never used tobacco were categorized as ex-addict and nonusers, respectively.
CI, confidence interval; HDL-C, high-density lipoprotein cholesterol; HTN, hypertension; LDL-C, low-density lipoprotein cholesterol.
Tobacco use and ex-tobacco use were observed to be significantly higher in undiagnosed diabetes. It was followed by prediabetes and diagnosed diabetes groups compared with the without diabetes group.
Association of risk factors and diabetes/prediabetes status: comparison of younger and older adults
CVD risk factors by age and diabetes status among the Pakistani population is denoted in Table 3. Known HTN was notably higher (46.8%) in young and (46.7%) in older age in people with diabetes compared with those with undiagnosed diabetes, prediabetes, and without diabetes groups. A similar pattern was seen for obesity, which is substantially higher in individuals with diagnosed diabetes (74.5%) compared with those with undiagnosed diabetes (65.4%), prediabetes (58.6%), and without diabetes (54.3%), respectively. New diagnosis of HTN was most observed in undiagnosed diabetes (24.2.%) in young, whereas 35% belongs to prediabetes older population. The absolute difference of known HTN and obesity in diagnosed diabetes with undiagnosed diabetes, prediabetes, and without diabetes group is higher in the young population compared with the similar status of dysglycemia in the older population.
Cardiometabolic Risk Factors by Both Age and Diabetes Status
Data presented as % (95% CI).
Significantly different from without diabetes.
Significantly different from prediabetes.
Significantly different from Undiagnosed.
Diabetes was defined as FPG level ≥126 mg/dL or 2-hr PGL ≥200 mg/dL or both, prediabetes was defined as FPG level between 110 and 125 mg/dL and 2-hr PGL ≥140 mg/dL but <200 mg/dL or both.
Newly diagnosed HTN: systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg; Known HTN: previous history of HTN; Obesity: BMI ≥25 kg/m2; Central obesity: Waist circumference ≥90 and ≥80 cm in males and females, respectively; Dyslipidemia: serum cholesterol >200 mg/dL or serum LDL-C >130 mg/dL or serum HDL-C <40 and <50 mg/dL for male and female, respectively, or serum TG >150 mg/dL or taking any lipid-lowering medications; Current tobacco users were defined as any form of tobacco use without quantification of amount and duration of use within 3 months from time of data collection, while used tobacco before 3 months and those who never used tobacco were categorized as ex-addict and nonusers, respectively.
Tobacco use and ex-tobacco use were higher in the undiagnosed diabetes group compared with diagnosed diabetes and prediabetes groups in young adults, whereas the most frequent use of tobacco was noted in prediabetes older adults. Central obesity and dyslipidemia were considerably higher in persons with undiagnosed diabetes compared with prediabetes and without diabetes groups. Higher levels of obesity, central obesity, ex-tobacco use, and dyslipidemia were noted in the young prediabetes group compared with the without diabetes group. In older adults, newly diagnosed HTN was higher in prediabetes, undiagnosed diabetes, and those with diagnosed diabetes, respectively, compared with the without diabetes population.
The absolute difference in the prevalence of more than three CVD risk factors was indistinguishable between diagnosed diabetes and undiagnosed diabetes in both age groups. Also, statistically, a significant difference is noted in diagnosed diabetes group in both aged populations compared with undiagnosed diabetes, prediabetes, and nondiabetes groups.
Adjusted odds ratios for age-stratified analyses
Adjusted odds ratios of CVD risk factors for adults with dysglycemia compared with without diabetes (<45 years of age) compared with (≥45 years of age), are presented in Fig. 1. After adjustment for gender, marital status, locality type, education, and physical activity, the odds ratios for CVD risk factors such as in dysglycemic adults, dyslipidemia was the most noticeable risk factor in young adults [adjusted odd ratio (95% CI)] [3.62 (1.69–7.72)] than older adults [2.93 (1.7–5.05)]. Known HTN and new diagnosis of HTN were considerably greater in older dysglycemic adults [2.22 (1.76–2.79)] and [2.07 (1.6–2.69)] compared with young counterparts [1.94 (1.53–2.45)] and [1.52 (1.18–1.96)], respectively. Odds for obesity and central obesity [1.65 (1.25–2.19)] and [1.34 (1.02–1.75)] were more in young dysglycemic adults versus older adults [1.35 (1.04–1.76)] and [1.23 (0.92–1.64)], correspondingly, in comparison to the without diabetes group in both age categories. Ex-tobacco use had a protective effect more in young dysglcemic than old age group, whereas the current use of tobacco had more chances of dysglycemia in the young than the older group.
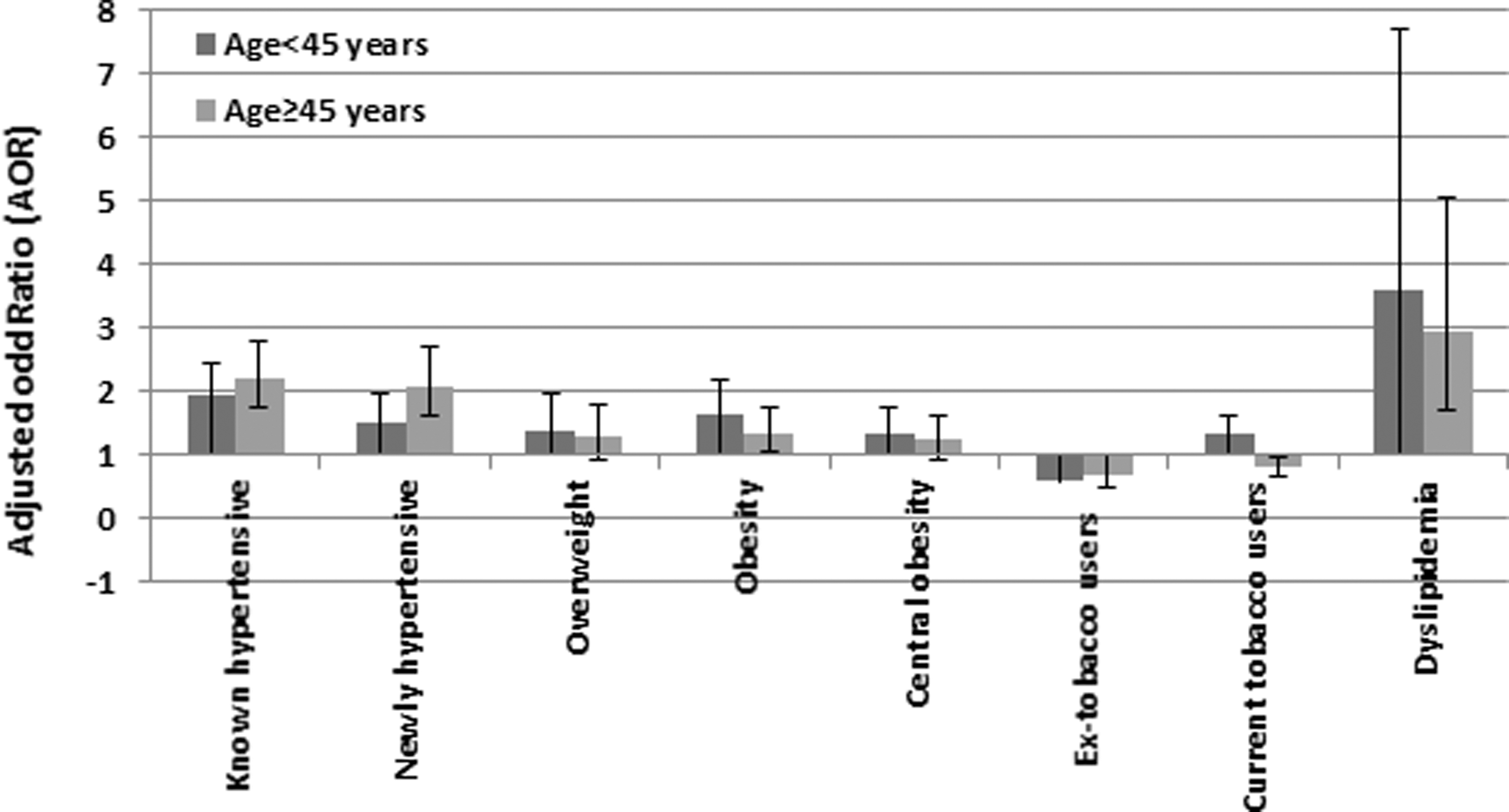
Adjusted odds ratios of cardiometabolic risk factors by age (<45 vs. ≥45 years). Data presented as odds ratio (95% CI). P value <0.05 considered to be statistically significant. Odds ratios adjusted for gender, marital status, locality type, education, and physical activity. AOR were compared separately for young dysglycemic group with the without diabetes young group, and older dysglycemic older adults with the without older adult group. Diabetes was defined as FPG level ≥126 mg/dL or 2-hr PGL ≥200 mg/dL or both, Prediabetes was defined as FPG level between 110 and 125 mg/dL and 2-hr PGL ≥140 mg/dL but <200 mg/dL or both. Newly diagnosed HTN: systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg; Known HTN: previous history of HTN; Obesity: BMI ≥25 kg/m2; Central obesity: Waist circumference ≥90 and ≥80 cm in males and females, respectively; Dyslipidemia: serum cholesterol >200 mg/dL or serum LDL-C >130 mg/dL or serum HDL-C <40 and <50 mg/dL for male and female, respectively, or serum TG >150 mg/dL or taking any lipid-lowering medications. Current tobacco users were defined as any form of tobacco use without quantification of amount and duration of use within 3 months from time of data collection, while used tobacco before 3 months and those who never used tobacco were categorized as ex-addict and nonusers, respectively. The 2-hr PGL, 2-hr post glucose level; AOR, adjusted odd ratio; BMI, body mass index; CI, confidence interval; FPG, fasting plasma glucose; LDL-C, low-density lipoprotein cholesterol; TG, triglycerides.
Overall, the CVD risk profile was worse in males in both age groups, although the accumulation of at least two risk factors was most frequent in young adults, irrespective of gender. At least three risk factors were most frequent in older males, whereas four or more risk factors were noted in female older adults (Table 4).
Frequency of Risk Factors by Age and Gender
Data presented as n (%).
P value <0.05 considered to be statistically significant.
The CVD risk factors assessed were tobacco use, central obesity, obesity, HTN, and dyslipidemia.
Diabetes was defined as FPG level ≥126 mg/dL or 2-hr PGL ≥200 mg/dL or both, Pre-diabetes was defined as FPG level between 110 and 125 mg/dL and 2-hr PGL ≥140 mg/dL but <200 mg/dL or both.
Newly diagnosed HTN: systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg; Known HTN: previous history of HTN; Obesity: BMI ≥25 kg/m2; Central obesity: Waist circumference ≥90 and ≥80 cm in males and females, respectively; Dyslipidemia: serum cholesterol >200 mg/dL or serum LDL-C >130 mg/dL or serum HDL-C <40 and <50 mg/dL for male and female, respectively, or serum TG >150 mg/dL or taking any lipid-lowering medications; Current tobacco users were defined as any form of tobacco use without quantification of amount and duration of use within 3 months from time of data collection, while used tobacco before 3 months and those who never used tobacco were categorized as ex-addict and nonusers, respectively.
CVD, cardiovascular disease.
Discussion
Consistent with conventional wisdom, older adults and men had a significantly higher prevalence of CVD risk factors than younger adults and women. High numbers of CVD risk factors were more prevalent in older adults in our study, yet younger adults also carry a much more profound relative increase in the prevalence of known HTN, obesity, central obesity, dyslipidemia, and tobacco use in undiagnosed diabetes and diagnosed diabetes groups compared with prediabetes and people without diabetes. Although, we found higher trends of CVD risk factors in above 40 years of age groups in line with previous reported data. 16 However, the high prevalence of one or two CVD risk factors forecast a potential epidemic of CVD in younger adults, and is similar to Andersson and Vasan, a study reflecting that high disease rates in young adults carry through into older age. 17 This study also supports the previous findings presenting that CVD risk factors develop at an early age, track through the young age of 30–39 years, and manifest in middle age. 18 Associated risk factors involve increasing age, positive family history of diabetes and overweight, obesity, and dyslipidemia at an earlier age.
Obesity was most frequent in known diabetes, followed by undiagnosed diabetes in both young and older adults, while it is significant in the prediabetes group of the young population. We also found raised prevalence of obesity, central obesity, and dyslipidemia as the most frequent CVD risk factors in younger adults with older adults, increasing the burden of public health challenges. 19,20 Dyslipidemia was remarkably increasing in subcategorizing of both age groups, and is a major risk factor for CVD but more specifically for younger adults. 21 Moreover, the raised prevalence of known HTN in diagnosed diabetes was observed in both age groups.
In younger adults, this may have been caused due to unawareness, undiagnosed HTN at an early age, and low resources for training the community health workers to screen for HTN. Also, lack of access to health care facilities was the main barrier for older population. 22,23
Overall adjusted odds for overweight, obesity, central obesity, tobacco use, ex-tobacco use, and dyslipidemia were more raised in dysglycemic young adults <45 years of age compared with older adults ≥45 years of age. CVD risk factors beginning in young adulthood is a public health concern, represents the future population health burden affecting morbidity and mortality rates, loss of quality of life, and a burden on the health care system. 24 It was also estimated that an individual diagnosed with diabetes at an age of 40 years will lose 6–7 years of life. Age remains a fundamental predictor of future risk of CVD. To improve the life expectancy for an individual, modification of traditional risk factors is necessary.
However, it is important to note that risk factor modification is equally important for both young and older individuals. It will reduce their subsequent risk of CVD. 25
Our findings also indicate the adaption of unhealthy lifestyle, increased urbanization, and lack of awareness in our population. The profound features of Pakistani culture, which include unhealthy dietary practices, liberal use of saturated and trans-fats in daily cooking especially curry-based cuisines, and extensive deep frying along with lack of physical activity are the main cause of dyslipidemia, obesity, and central obesity in younger adults. 26 These CVD risk factors have also been reported in other large community-based surveys. 27 Cardiovascular profile is unsatisfactory for Pakistan similar to other middle-income countries, especially modifiable risk factors. 28 This needs early attention to target them at the earliest since they are now appearing as an “epidemic.”
Adherence to WHO Framework Convention on Tobacco Control (FCTC) and sugar tax may be obligatory to impose consumption tax to reduce consumption of unhealthy food, revenue generation for tobacco control program, and subsidization of healthy food items especially in primary, secondary, and higher education academic institutions. Even though the current management strategies targeting CVD risk profile have been improved in Pakistan, however, majority of continuous treatment is barriered by the low socioeconomic status of the population. 29
Inadequate data for a history of hyperlipidemia, atherosclerotic cardiovascular disease, chronic kidney disease, drug history, and smoking versus smokeless tobacco use, considering these imperative risk factors for premature cardiovascular events, are our limitations. The survey was a cross-sectional study, and therefore, we were unable to determine the direction of the association and the ability to account for premature mortality, which may have contributed to a survivorship bias among older adults, are some other potential limitations. Yet, this inclusive information on various other modifiable and nonmodifiable risk factors, younger versus older Pakistani population, are worth noting in literature.
Conclusion
The overall preponderance of CVD risk factors as overweight, obesity, central obesity, tobacco use, ex-tobacco uses, and dyslipidemia after adjusting odd ratios were unusually more prevalent in dysglycemia groups of young adults (<45 years) compared with older adults (≥45 years). The accumulation of CVD risk factors at an early age with older adults highlights the importance of national prevention strategies to reduce the public health impact of diabetes in the young population of Pakistan. Early, effective, and targetted interventions involving public health strategies in public–private partnership along with allocation of sufficient financial resources for the management of CVD risk factors may be of prime concern.
NDSP members (with surnames in alphabetical order)
Dr. Mujeeb Ur Rehman Abro, Assistant Professor of Medicine, Chandka Medical College, Shaheed Mohtarma Benazir Bhutto Medical University, Larkana, Sindh.
Dr. Khawaja Ishfaq Ahmed, Ex-PGR, Pakistan Institute of Medical Sciences, Islamabad, Punjab.
Dr. Khurshid Ahmed, Consultant Physician, Zahid Medical Center, Hub, Baluchistan.
Dr. Sobia Sabir Ali, Assistant Professor, Department of Diabetes and Endocrinology, Lady Reading Hospital, Peshawar, Khyber Pakhtunkhwa.
Prof. Ahmed Bilal, Professor, and Head of Medical Department Faisalabad Medical College, Faisalabad, Punjab.
Dr. Anam Butt, Research Officer, Baqai Institute of Diabetology and Endocrinology, Baqai Medical University, Karachi, Sindh.
Prof. Bikha Ram Devrajani, Chairman, Department of Medicine and Director Sindh Institute of Endocrinology and Diabetes, Liaquat University of Medical and Health Sciences, Jamshoro, Sindh.
Mr. Ijaz Hayder, Research Officer, Pakistan Health Research Council, Karachi, Sindh.
Dr. Yasir Humayun, EPI coordinator, DHO Office, Mansehra, Khyber Pakhtunkhwa.
Mrs. Rabia Irshad, Research Officer, Pakistan Health Research Council, Karachi, Sindh.
Dr. Riasat Ali Khan, Diabetologist, Canada Medical Group Hospital, Defense, Karachi, Sindh.
Dr. Asima Khan, Head of Diabetes Department, Sindh Government Hospital, New Karachi, Karachi, Sindh.
Dr. Aamir Akram Khowaja, Postgraduate Resident, Sindh Government Qatar Hospital, Karachi, Sindh.
Dr. Raheela Khowaja, Postgraduate Resident, Baqai Institute of Diabetology and Endocrinology, Baqai Medical University, Karachi, Sindh.
Prof. Qazi Masroor, Professor of Medicine and Head of Department, Quaid-e-Azam Medical College, Bahawalpur, Punjab.
Dr. Maqsood Mehmood, Head of Department, Fatma Tu Zahra Hospital, Gujranwala, Punjab.
Mr. Hassan Moin, Statistician, Baqai Institute of Diabetology and Endocrinology, Baqai Medical University, Karachi, Sindh.
Ms. Nida Mustafa, Statistician, Baqai Institute of Diabetology and Endocrinology, Baqai Medical University, Karachi, Sindh, Pakistan.
Dr. Wasif Noor, Diabetologist, Akhuwat Health Services Diabetes Center, Lahore, Punjab.
Dr. Huma Qureshi, Ex-Director, Pakistan Health Research Council, Islamabad, Punjab.
Mr. Ibrar Rafique, Research Officer, Pakistan Health Research Council, Islamabad, Punjab.
Dr. Tahir Rasool, Diabetologist, Akhuwat Health Services Diabetes Center, Lahore, Punjab.
Mrs. Rubina Sabir, Laboratory Manager, Baqai Institute of Diabetology and Endocrinology, Baqai Medical University, Karachi, Sindh.
Dr. M. Arif N. Saqib, Senior Research Officer, Pakistan Health Research Council, Islamabad, Punjab.
Dr. Pir Alam Said, Medical Specialist DHQ, Sawabi, Khyber Pakhtunkhwa.
Prof. Abrar Shaikh, Head Department of Medicine, Ghulam Muhammad Mahar Medical College, Sukkur, Sindh.
Prof. Bilal Bin Younus, Head of Sakeena Institute of Diabetes & Endocrine Research, Lahore, Punjab.
Prof. Salma Tanveer, Professor of Medicine, In-charge Diabetes and Endocrinology, Nishter Medical University, Multan, Punjab.
Prof. Jamal Zafar, Professor of Medicine, Pakistan Institute of Medical Sciences, Islamabad, Punjab.
Data Sharing Statement
Aggregated data may be available upon reasonable request to the corresponding author. Approvals must be obtained from all collaborators with a signed data access agreement.
Footnotes
Acknowledgments
All authors, who are NDSP Members, are thankful to late Prof. Samad Shera, Ex-Secretary General, Diabetic Association of Pakistan and WHO Collaborating Center, Karachi—for his contribution in the conduct of this NDSP survey (2016–2017). The authors acknowledge the support of the Research and Laboratory Department of Baqai Institute of Diabetology and Endocrinology (BIDE), Karachi for data management and Mr. Abdul Rashid and Mr. Muhammad Sohail from Pakistan Health Research Council (PHRC), Karachi. They are also grateful to all study subjects for their participation in the second NDSP (2016–2017).
Authors' Contributions
A.F.: Concept, design, involvement in quality control, editing, and approval of the final article. N.W.: Literature search, interpretation of data, writing, and review of the final article. K.A.B.: Literature search, interpretation of data, writing, and review of the final article. B.T.: Literature search, interpretation of data, editing, and review of the final article. E.W.G.: Interpretation of data, editing, and review of the final article. A.B.: Concept, design, involvement in quality control, editing, and approval of the final article. NDSP Members: Members were responsible for the supervision of the survey, concept, design, involvement in the quality control and data management in their respective areas. All members approved the final submitted version.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
The funding source for the study remained the same as in the second NDSP (2016–2017). Hemoglobin A1c and lipid profiles were performed by the Pakistan Health Research Council (PHRC). Field visits and data collection, including clinical and anthropometric measurements, fasting plasma glucose, and 2-hr post/glucose load samples was run by the respective teams through their funds. The whole survey was coordinated and supported by the Baqai Institute of Diabetology & Endocrinology (BIDE) on their resources.