
Abstract
Background:
The metabolic syndrome (MS) is associated with an increased production of nitrogen metabolites and elevated oxidative stress, which favors progression of nonalcoholic fatty liver disease (NAFLD). Subjects with the phenotype known as metabolically unhealthy obese (MUO) meet most of the MS cardiometabolic risk criteria and show a higher risk of advanced NAFLD severity, compared with the so-widely known metabolically healthy obese (MHO). Obese individuals with MS are more susceptible to abnormal lipid accumulation in different tissues, whereas oxidative stress and nitrogen metabolites are increased in MS and/or obesity. This study aimed to explore whether plasma- or liver tissue-determined biomarkers of nitrogen metabolism and oxidative stress relate to NAFLD severity and/or metabolic phenotype.
Methods:
This cross-sectional study included candidates for bariatric surgery with biopsy-proven NAFLD diagnosis and staging. For comparison, the study population was divided according to NAFLD damage (steatohepatitis F0–F1 vs. steatohepatitis F2–F4) and metabolic phenotype (MHO vs MUO, based on the MS criteria). Hepatic and plasma concentrations of nitrogen metabolites and oxidative stress biomarkers were determined by enzymatic kinetics assays, enzyme-linked immunosorbent assay, and Greiss reaction.
Results:
The study population (N = 45) was constituted by patients with obesity and higher prevalence of dyslipidemia, diabetes mellitus, and hypertension. According to plasma biomarkers, MUO phenotype was related to higher cardiometabolic risk; meanwhile, advanced NAFLD damage was related to higher glycated hemoglobin (HbA1c) and triglycerides. Elevated hepatic concentrations of ammonium, nitrites, arginine, and citrulline were found in MUO phenotype, but only higher plasma concentration of malondialdehyde was found as specifically related to advanced NAFLD damage.
Conclusions:
Circulating biomarkers of redox state were selectively related to advanced NAFLD damage, suggesting prognostic and therapeutic targets. Hepatic concentrations of nitrogen metabolism biomarkers may be more related to cardiometabolic risk.
Background
Nonalcoholic Fatty Liver Disease (NAFLD) affects about 30% of the population worldwide. Several reports show that the population of Mexico has multiple risk factors for the NAFLD development, whereas prevalence has been estimated as higher than 50%. 1 NAFLD has become a public health major issue due to potential liver damage progression, including fibrosis, cirrhosis, or hepatocarcinoma, 2 as well as high cost for therapy, reaching up to $7804 United States dollars (USD) for a new NAFLD diagnosis and $3789 USD for long-term management. 3
NAFLD progression is influenced by local noxious environmental mediators, such as oxidative stress and nitrogen metabolites, 4,5 as well as metabolic factors, such as obesity, diabetes mellitus, and/or dyslipidemia. In fact, NAFLD is particularly frequent in population with metabolic syndrome (MS); meanwhile, obese individuals with MS are more susceptible to abnormal lipid accumulation in different tissues. 6 Furthermore, oxidative stress markers such as malondialdehyde (MDA), as well as nitrogen metabolites, are increased in MS and/or obesity. 7,8
Currently, there is a lack of a well-established method for a clear pathophysiological characterization of local noxious mediators and metabolic risk factors during NAFLD severity progression. Likewise, whether hepatic damage is reflected by plasma biomarkers in patients with NAFLD and MS is unknown.
The present study evaluated the activity of oxidative stress-related enzymes, nitrogen metabolism, both in plasma and in liver tissue, which may identify potential targets for prevention and/or prognosis of advanced NAFLD damage in population with MS.
Materials and Methods
Participants
Participants were subjects with obesity, candidates for bariatric surgery [as defined by body mass index (BMI) >40, or >35 with co-morbidities], older than 18 years, with and without MS. Subjects were eliminated if they consumed drugs with potential effect on oxidative stress or nitrogen metabolism mediators, or were exposed to any hepatotoxic condition (alcohol, drugs, hepatitis virus, cholestasis, among others). All patients had psychological and endocrine profile assessments. This project was registered and approved by Institutional Ethics and Biosafety Review Boards (ID 500.2017) and complies with recommendations from the Declaration of Helsinki. All participants signed informed consent.
Design
The study design was an observational, cross-sectional, analytical, and comparative study performed at the Centro Médico Nacional “20 de Noviembre,” ISSSTE, a third-level referral medical center based in Mexico City. The study was designed to evaluate whether liver-specific biomarkers of nitrogen metabolism and oxidative stress may relate to NAFLD severity and/or metabolic phenotype. The study population was recruited at the Department of Bariatric Surgery.
Demographic and anthropometric data and sample collection
Age, sex, BMI, waist circumference, and blood pressure were obtained during clinical history and physical examination before bariatric surgery. On the day of the procedure, before the surgery, a sample of peripheral venous blood (10 mL) was obtained and centrifuged to obtain plasma, which was frozen at −80°C until further analysis. Liver biopsy was performed during bariatric surgery, in those cases with previous biochemical or ultrasound evidence suggestive of NAFLD; or at surgeon discretion, based on macroscopic liver tissue changes.
Plasma biomarkers
Quantification of plasma glucose, lipid profile, and glycated hemoglobin (HbA1c) was evaluated through routine automatized nephelometric laboratory assays. Plasma concentration of MDA and nitric oxide was determined by Colorimetric/Fluorometric Assay Kit (BioVision, Incorporated, CA) and Nitric Oxide Colorimetric Assay Kit (BioVision, Incorporated), respectively, following the provider's instructions.
Hepatic biomarkers
A liver sample of ∼0.5–1.0 cm3 was obtained by wedge biopsy during the surgical procedure. Then, ∼200 mg of liver tissue was deproteinized in 1 N perchloric acid, neutralized, and the following analytes were determined in the acid extracts: nitrite (Griess reaction), citrulline, and pyruvate according to colorimetric methods. 9 –12
Additionally, the amount of MDA was measured by its reaction to thiobarbituric acid. 13 The activities of the arginase and ornithine transcarbamylase-transferase enzymes were also determined by previously described techniques. 14
NAFLD damage assessment
A piece of liver tissue was fixed in 4% paraformaldehyde, paraffin-embedded, and slides were processed with hematoxylin and eosin and Masson's trichrome staining protocols. Histological assessment of liver fibrosis progression was performed by two experienced pathologists (interobserver coefficient correlation >0.8), based on Brunt and Kleiner classification, as follows: steatohepatitis refers to liver damage including ballooning and different degrees of necroinflammation, such as: G1 (mild) refers to ballooning in some hepatocytes and minimal portal inflammation; G2 (moderate) refers to ballooning, abundant steatosis, and evident portal inflammation; G3 (severe) refers to diffuse balloning, diffuse inflammation, and portal inflammation. Liver fibrosis was assessed as follows: F0, no fibrosis; F1, perisinusoidal or periportal; F2, perisinusoidal and portal/periportal; F3, bridging fibrosis; F4, cirrhosis. 15,16 Only for analytic purposes of this study, low liver fibrosis was considered at stages F0–1, whereas advanced liver fibrosis was considered at stages F ≥ 2.
Metabolic risk phenotype and subgroups
MS was defined according to the U.S. Adult Treatment Panel-III criteria 17 meeting at least three of the following five criteria: (1) fasting plasma glucose >100 mg/dL; (2) plasma triglyceride level ≥150 mg/dL; (3) plasma high-density lipoprotein cholesterol (HDL-C) level for women ≤50 mg/dL and for men ≤40 mg/dL; (4) blood pressure ≥130/85 mmHg; and (5) waist circumference for women >88 cm and for men >102 cm.
Patients without MS were considered as metabolically healthy obese (MHO) patients. Likewise, the patients meeting the MS criteria were considered as metabolically unhealthy obese (MUO) patients. To perform a systematic analysis, we subdivided the study population according to the metabolic phenotype and the hepatic fibrosis progression as follows: group 1: MHO phenotype with liver fibrosis stages 0 to 1 (low fibrosis); group 2: MUO with liver fibrosis 0 to 1 (low fibrosis); and group 3: MUO with liver fibrosis ≥2 (advanced fibrosis).
Statistical analysis
Due to the methodological strategy of the study, sample size was calculated considering 95% confidence interval, alpha = 0.05, adjusted by the total number of patients who met the selection criteria. Data are expressed as median and interquartile range or n (%) according to their nature. Two-way, independent U Mann–Whitney or one-way analysis of variance (ANOVA) was performed for median comparison, as appropriate; while chi-square was applied for qualitative data. P < 0.05 was considered statistically significant. Data were analyzed using SPSS v.25 (IBM Corp., Armonk, NY).
Results
The study population consisted of 45 patients with obesity (female, 64%), candidates for bariatric surgery under criteria of the Department of Bariatric Surgery. These patients presented with diabetes mellitus, arterial hypertension, and dyslipidemia as the most prevalent co-morbidities. The study population was further divided according to the cardiometabolic risk, where MUO phenotype was characterized by younger age and lower prevalence of females, as well as significantly higher cardiometabolic risk evidenced by higher BMI, waist circumference, systolic blood pressure, accompanied by dysmetabolic markers such as increased glucose, HbA1c, triglycerides, and lower HDL-C. Clinical characteristics are shown in Table 1.
Characteristics of the Study Population (N = 45)
Quantitative data are shown as median (IQR), categorical data are shown as n (%). Significant difference was considered when P < 0.05 (two-tailed, independent U Mann–Whitney test MUO vs. MHO).
BMI, body mass index; DBP, diastolic blood pressure; FBG, fasting blood glucose; HbA1c, glycated hemoglobin; HDL-C, high-density lipoprotein cholesterol; IQR, interquartile range; MHO, metabolically healthy obese; MUO, metabolically unhealthy obese; NS, nonsignificant; SBP, systolic blood pressure; TG, triglycerides; WC, waist circumference.
Analyses of liver biopsies revealed different stages of NAFLD severity. Such features allowed subdividing patients in three categories, considering the cardiometabolic phenotype (MHO and MUO) and liver histological characteristics including the degree of steatosis, severity of steatohepatitis, and fibrosis (Table 2, and representative biopsies of each subgroup are shown in Fig. 1). Of note, the subgroup of MHO with advanced liver fibrosis was unable to integrate, due to the scanty number of patients.
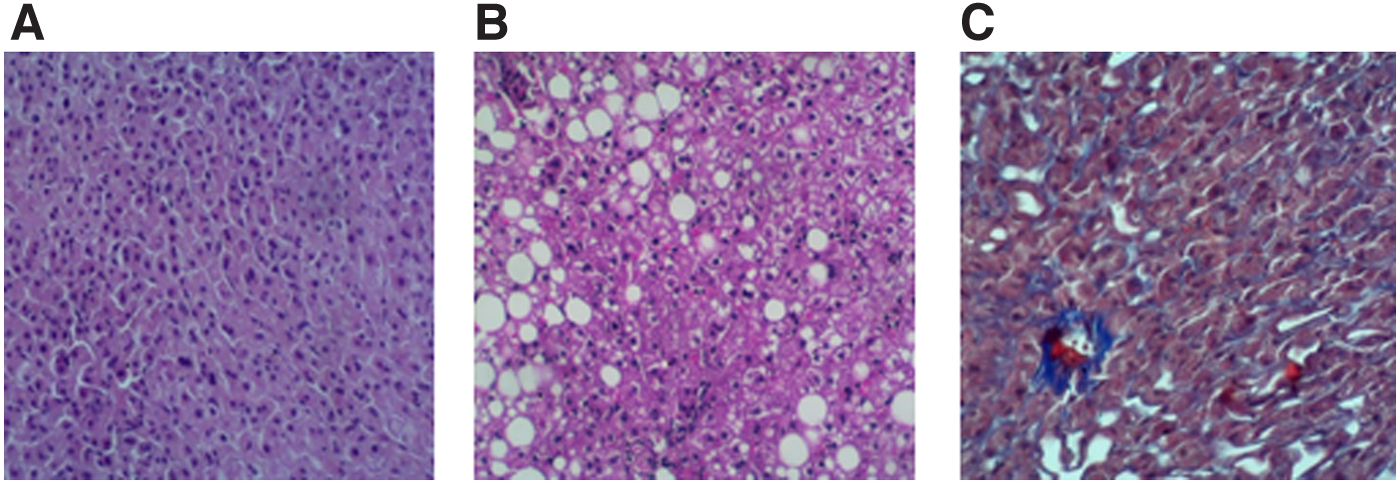
NAFLD and metabolic risk phenotype. Representative images of liver histology in Masson's trichrome staining, subgroups according to metabolic risk phenotype.
Cardiometabolic Phenotype and Nonalcoholic Fatty Liver Disease Scoring (N = 45)
Data are shown as n (%). Significant difference was considered when P < 0.05 (one way, ANOVA between MHO+LF vs. MUO+LF vs. MUO+HF).
It refers to relative quantification of liver parenchyma with steatotic damage.
Steatohepatitis refers to liver damage including ballooning and different degrees of necroinflammation, such as: G1 (mild) refers to ballooning in some hepatocytes and minimal portal inflammation; G2 (moderate) refers to ballooning, abundant steatosis, and evident portal inflammation; G3 (severe) refers to diffuse balloning, diffuse inflammation, and portal inflammation.
ANOVA, analysis of variance; MHO+LF, metabolically healthy obese with low hepatic fibrosis; MUO+HF, metabolically unhealthy obese with high hepatic fibrosis; MUO+LF, metabolically unhealthy obese with low hepatic fibrosis.
During comparative analysis, MUO phenotype was related to higher BMI, systolic blood pressure, plasma glucose, HbA1c, and triglycerides, whereas the progressive liver fibrosis was specifically related to higher plasma HbA1c and triglycerides (Table 3).
Metabolic Profile and Liver Fibrosis Progression (N = 45)
Quantitative values are shown as median and IQR (p25, p75). p Value=*statistically significant difference between metabolic phenotypes (MHO vs. MUO) two-tailed U Mann–Whitney. **Significant difference between stages of nonalcoholic fatty liver disease progression, one-way ANOVA.
Biochemical analyses showed that liver concentration of ammonium, nitrites, arginine, and citrulline was significantly elevated in MUO phenotype, regardless of NAFLD condition (Fig. 2).
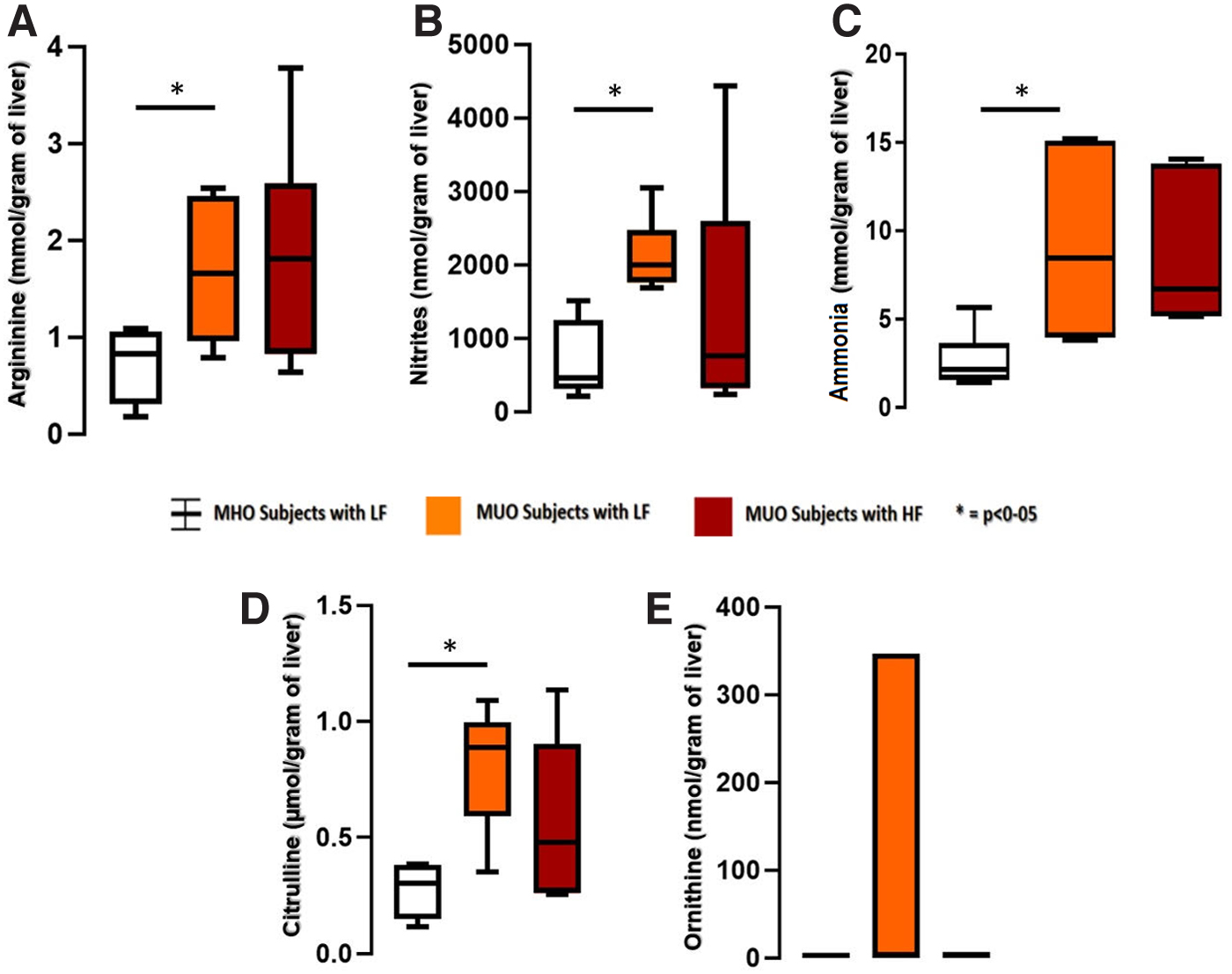
Liver tissue nitrogen metabolic products and metabolic phenotype. Hepatic concentration of nitrogen metabolism products, such as
However, higher plasma concentration of MDA was found to be specifically related to the advanced NAFLD damage, regardless of the metabolic phenotype (Fig. 3).
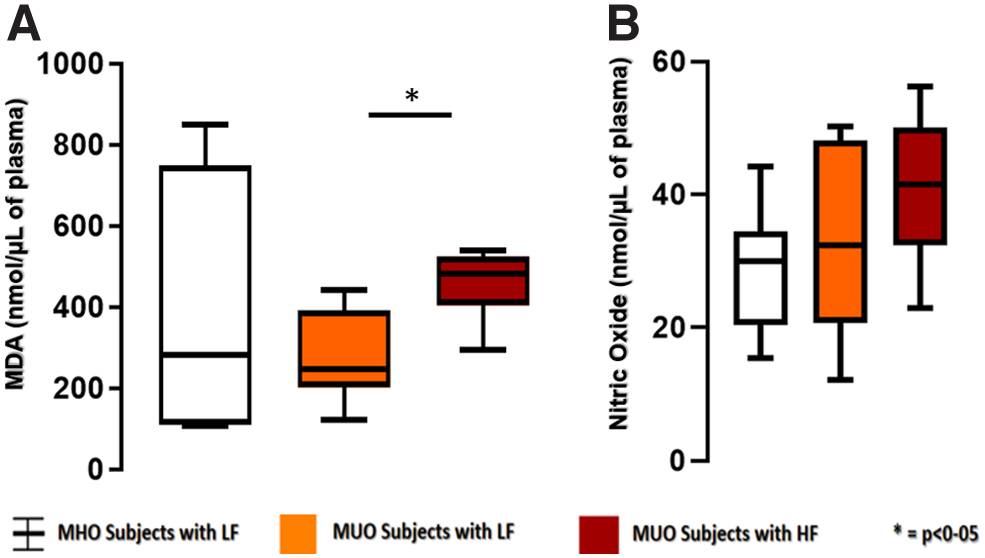
Plasma metabolic products and metabolic phenotype. The levels of
Discussion
Chronic impairment of lipid metabolism observed in MS is related to oxidative unbalance and cellular mechanisms leading to inflammation and fibrogenesis, contributing to the development of NAFLD and progression into nonalcoholic steatohepatitis (NASH). Likewise, expression of urea cycle-related genes is downregulated in NAFLD and NASH, suggesting the role of nitrogen mediators in NAFLD damage. 4,18
Gutiérrez-Grobe et al 19 reported a higher prevalence of hepatic histological damage in MUO phenotype, compared with MHO phenotype, during analyses of biopsy-proven liver damage in populations with cardiometabolic risk. Consistently, we observed similar findings in our study group of patients with MUO phenotype. This observation may have several possible explanations. MUO phenotype shows a higher activation of the NLP3-inflammasome-related molecule in macrophages in adipose tissue, compared with MHO. Such difference may favor proinflammatory responses, 20 along the ability of NLP3 to interact with protein PYCARD/ASC and promote local inflammation and apoptosis, which may be involved in NAFLD progression; 21 likewise, liver metabolism disorders and lipid accumulation in hepatocytes are strongly linked to insulin resistance and components of MS, which are cumulative in the MUO phenotype.
Furthermore, we observed that circulating pro-oxidative mediator MDA was selectively related to advanced NAFLD damage. In this regard, oxidative stress is known to be associated with NAFLD progression into NASH. Videla et al found an increase in oxidative mediators in patients with NAFLD, which further exacerbated in cases with steatohepatitis. 22 In addition, considerable evidences support the role of oxidative stress in NAFLD progression: (1) increase in reactive oxygen species may promote liver parenchymal cell death 22 and trigger transition from steatosis to steatohepatitis; 23 (2) lipid peroxidation, as reflected by MDA, may be related to depletion of n-6 long-chain polyunsaturated fatty acids and impairment of fatty acid oxidation and triacylglycerol metabolism; 22 (3) a recent study showed that oxidative stress in the liver tissue was related to increased lipotoxicity and steatosis exacerbation in humans. 24
Unexpectedly, nitrogen metabolism biomarkers within the hepatic tissue were mainly related to cardiometabolic risk, more than advanced NAFLD damage. This observation is consistent with the already described role of reactive nitrogen species in the cellular redox system related with cardiometabolic diseases. 25 Recently, the relation between NAFLD and cardiovascular disease has been increasingly recognized. Heart diseases are the most common cause of mortality in individuals with NAFLD, 26 larger than the number of liver-related deaths, whereas the estimated 10-year risk score is increased in individuals with NAFLD, and multivariable regression analyses demonstrate up to a 3.4-fold increase in cardiovascular risk for advanced stages of hepatic steatosis. Consistently, the group with MUO phenotype from our study population shared several components of MS and higher cardiovascular risk.
However, the finding of specific increase of plasma MDA during advanced NAFLD damage, regardless the metabolic phenotype, suggests that oxidative stress is clinically relevant for NAFLD pathophysiology and therapeutic targets. Consistently, intervention of carotenoid-rich diets results in MDA reduction as well as decrease of NAFLD biomarkers in rats. 27 Likewise, the pro-oxidant biomarkers associated with advance NAFLD have also been described as proinflammatory and pro-atherogenic mediators and then representing a potential link between NAFLD and cardiovascular disease. 28 However, the role of MDA as specific biomarker of advanced hepatic damage deserves a careful interpretation since other observations from our group, addressing different damage mechanisms, suggest that either oxidative stress or nitrogen reactive species are involved in metabolic disease. 29
Unfortunately, we were not able to weight additional factors and potential interactions influencing the effect of oxidative stress on advance hepatic fibrosis in NAFLD, which constitutes a study limitation. Additional aspects to be considered include: (1) the cross-sectional nature of this study might not objectively evaluate the time-course prospective evolution of NAFLD progression and related biomarkers; therefore, a causal role of the proposed study biomarkers deserves careful interpretation; (2) small sample size, which may be compensated by the methodological design of a concomitant study of liver and plasma tissue biomarkers. This is relevant since liver biopsy is the gold standard for the diagnosis of fibrosis and precise classification of NAFLD, despite only few studies have been able to do so. Regardless of the small sample size, we were able to obtain significant results in the biomarkers.
Finally, our study suggests that patients with MS and NAFLD should not be equally treated, given their corresponding association with either cardiovascular risk or pro-oxidant status and advanced NAFLD damage, respectively.
Conclusions
Circulating MDA, as surrogate biomarker of lipid peroxidation and redox state, is selectively related to advanced NAFLD damage, supporting prognostic and therapeutic potential target, whereas hepatic concentrations of nitrogen metabolism biomarkers may be related to the cardiometabolic risk phenotype.
Footnotes
Acknowledgment
The authors acknowledge Dr. María Angélica Díaz-Aranda for her academic assistance.
Authors' Contributions
The authors certify that each author participated sufficiently in the study. J.A.S.-C. designed the study, discussed and interpreted the data, and drafted the article. G.A.D.-P. collected the liver biopsies and the data, carried out the colorimetric assay techniques and analysis, discussed and interpreted the data, and drafted the article. R.E.H.-M. conceived the study, carried out the colorimetric assay techniques and analysis, discussed and interpreted the data, and drafted the article. A.H.-P. and E.V.-G. carried out the colorimetric assays and analysis, discussed and interpreted the data, and drafted the article. J.A.G.-B. collected the liver biopsies and the data, discussed and interpreted the data, and drafted the article.
M.S.-G. designed the study, performed the histopathologic grading of steatosis and fibrosis, discussed and interpreted the data, and drafted the article. J.M.-R. and O.F.G.-F. designed the study, performed the surgical interventions and obtained the liver biopsies, discussed and interpreted the data, and drafted the article. C.A.-R., A.R.R.-N., S.G., and P.M.-T. designed the study, discussed and interpreted the data, and drafted the article. All authors have agreed to be accountable for all aspects of the work. All authors have read and approved the final article.
Ethics Approval and Consent to Participate
This project was registered (ID 500.2017) and authorized by Institutional Ethics and Biosafety in Research Review Boards and complies with recommendations from the Declaration of Helsinki.
Availability of Data and Materials
The data sets generated and/or analyzed during the current study are not publicly available due to institutional data use guidelines but are available from the authors on reasonable request.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
The authors state that this study was partially supported by the grant S0008-2015-1 - project ID 262335, funded by Consejo Nacional para la Ciencia y Tecnología (CONACYT); and by the support from Programa E-015 de Investigación y Desarrollo Tecnología en Salud, Project ID 500.2017, from Instituto de Seguridad Social para los Trabajadores del Estado.