
Abstract
Background:
The visceral adipose tissue excess in patients with diabetes mellitus (DM) is one of the mechanisms that plays role in the development of coronary atherosclerosis. Our study aimed to investigate the relationship between visceral adiposity index (VAI), an indicator of visceral adiposity, and Syntax score (SxS), a predictor of the severity of coronary artery disease (CAD), in patients with stable angina pectoris (SAP) and type 2 DM.
Methods:
A total of 253 patients with SAP and type 2 DM were included in this cross-sectional study. The patients were divided into three risk groups (low risk <22, 32 ≥ intermediate risk ≥22, high risk ≥33) according to the SxS based on invasive coronary angiography. Several adiposity indexes such as body mass index, waist-to-hip ratio (WHR), waist-to-height ratio (WHtR), body adiposity index (BAI), and lipid accumulation product index (LAPI) were calculated using relevant formulas. In addition, VAI scores for each patient were calculated.
Results:
There were no statistically significant differences between the low-, intermediate-, and high-risk groups for WHtR, BAI, and LAPI. WHR was found significantly lower in the low SxS group (P = 0.0038), and VAI was found significantly higher (P = 0.021) in the high SxS group. Besides, in multivariate logistic regression analysis, the VAI (odds ratio: 2.455; 95% confidence interval: 1.244–4.845; P = 0.010) was an independent predictor of high SxS. In the receiver operating characteristic curve analysis, VAI with an optimal cutoff value of 2.048 predicted the severe coronary lesion with a sensitivity of 60.8% and a specificity of 61.5%.
Conclusion:
This study showed that VAI was an independent predictor in estimating CAD severity in patients with SAP and type 2 DM.
Introduction
World Health Organization declared that 17.9 million people died due to cardiovascular causes (32% of all deaths) in 2019, and coronary artery disease (CAD) may be increased depending on the prevalence of the many triggering factors, such as obesity. 1 For this reason, the studies assessing the relationship between obesity and cardiovascular risk gained more significance recently. It has already been shown that not only weight and height but also visceral adiposity, which is the indicator of the adipose tissue surrounding the intra-abdominal organs, should be take into account during the assessment of obese persons in terms of cardiovascular risk. 2 Visceral adipose tissue has been found to be associated with cardiovascular risk even if individuals are not overweight. 3
The most reliable tools are computed tomography (CT) and magnetic resonance imaging (MRI) to evaluate visceral fat tissue, regional fat deposition, and the total fat amount. 4 However, these imaging techniques are expensive, not widely accessible, and require experience. Recently, several indexes, such as body mass index (BMI), waist circumference (WC), waist-to-hip ratio (WHR), waist-to-height ratio, body adiposity index (BAI), lipid accumulation product index (LAPI), and visceral adiposity index (VAI), were used in cardiovascular risk assessment. 5 The capability of VAI to provide information about visceral adipose tissue was confirmed by MRI, and it was found to be useful in cardiovascular risk assessment. 2
The powerful results through the VAI are probably due to its formula, which takes into account gender, anthropometric measurements (WC, BMI), and lipid levels such as triglycerides and high-density lipoprotein cholesterol (HDL-C). 2 Diabetes mellitus (DM) is a definitive risk factor for cardiovascular diseases and CAD. 6 In addition, patients with DM have increased visceral adiposity, which is an indicator for ectopic and dysfunctional fat tissue accumulation, compared with the healthy population. 7 The opposite of this is also accepted as true, that is, people with excess visceral adipose tissue have a higher risk of DM. Visceral fat tissue excess in patients with DM was found to be related to increased risk of hypertension, atherosclerosis, and mortality. 8
Coronary atherosclerosis, one of the most common causes of sudden death, is significantly common in patients with DM. 9 Therefore, it is important to evaluate visceral adiposity, especially in patients with high risk for atherosclerosis such as patients with DM. When evaluating coronary atherosclerosis, it is not sufficient to evaluate its presence alone. The location and morphological features of the coronary plaque (length, calcification, presence of thrombus) are also important for predicting the complications of CAD. Therefore, the Syntax score (SxS), which is a valuable scoring system that evaluates the features of the coronary plaques and provides information about the severity of CAD, has been developed. 10
The increasing prevalence of DM worldwide has led to an increase in the importance of all kinds of indexes that show diabetic complications. At present, there are several indexes that can predict the severity of CAD in patients with stable angina pectoris (SAP) and type 2 DM. However, the potential of VAI, which is calculated by a cost-effective, simple, and additional device-free method, in predicting the severity of atherosclerosis in these patients is unknown. Therefore, we aimed to investigate the relationship between VAI, an indicator of visceral adiposity, and SxS, a predictor of the severity of CAD, in patients with SAP and type 2 DM in this study.
Materials and Methods
Study population
In this cross-sectional study, the patients who visited the cardiology outpatient clinic between February 2018 and April 2020 were evaluated. Participants were patients with type 2 DM who were diagnosed with SAP. A total of 253 consecutive patients were included in the study after the exclusion of the patients who met the exclusion criteria (Fig. 1). Coronary angiography was performed in all patients. The diagnosis of SAP was made by the criteria specified in the guidelines. 11 Exclusion criteria were as follows: patients younger than 18 years, type 1 DM, acute coronary syndrome, peripheral artery disease, stroke, history of revascularization, left ventricular ejection fraction <50%, moderate-to-severe valvular disease, chronic liver disease, renal failure, acute or chronic inflammation, malignancy, and other endocrinological disorders.
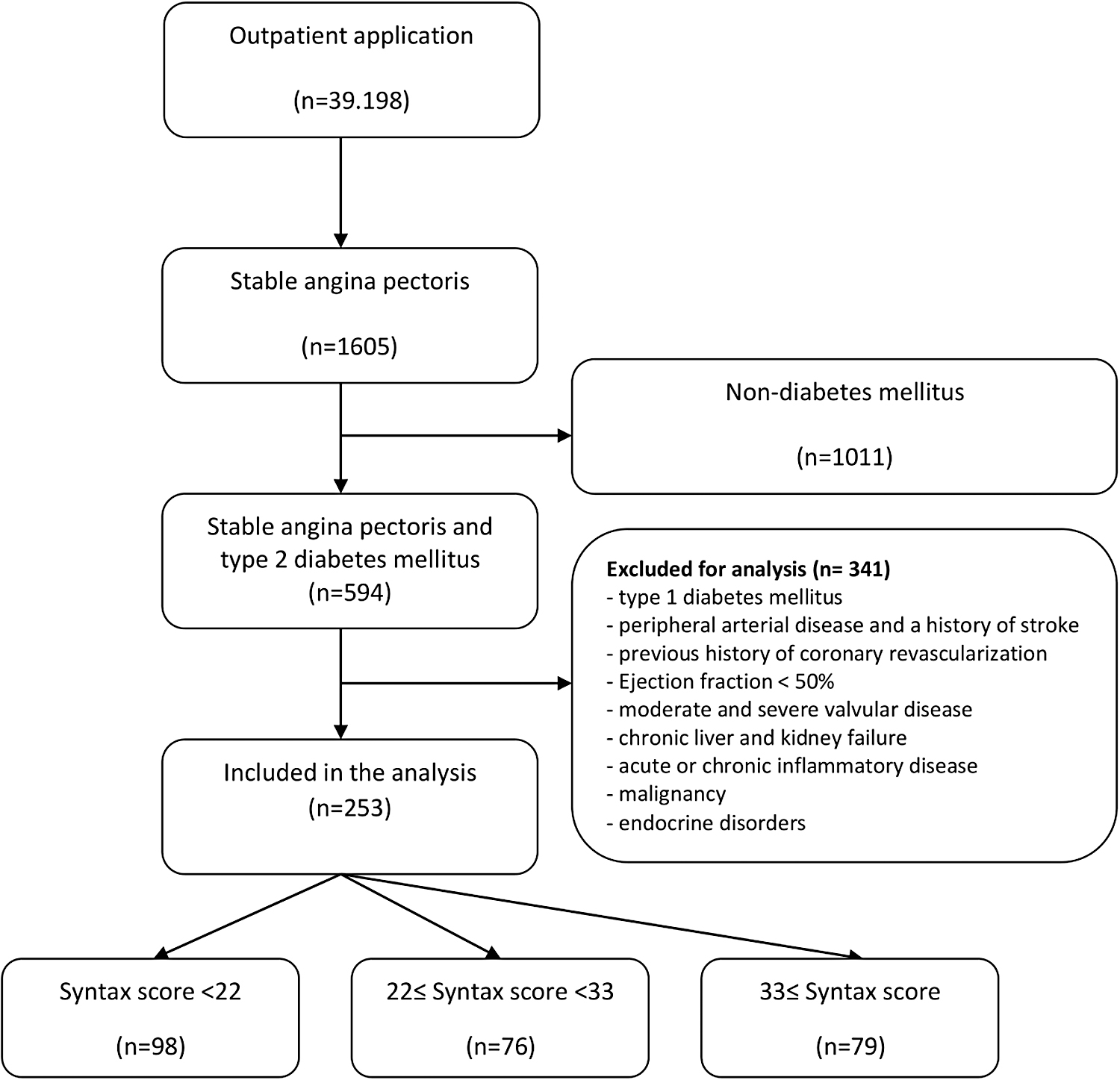
Flowchart of the study.
Written informed consent was received from all patients. The study was designed according to the principles of the Declaration of Helsinki and was approved by the local ethics committee.
Clinical assessment
Demographic characteristics (age, gender, smoking) and co-morbidities were obtained from the medical records. The intravenous blood samples were collected after overnight fasting. Complete blood count was measured by an autoanalyzer (Beckman Coulter DxH 900; Beckman Coulter, Miami, FL). Total cholesterol, HDL-C, low-density lipoprotein cholesterol, triglyceride values, and other biochemical measurements were measured by an automatic chemical analyzer (Olympus AU2700 analyzer; Olympus CO Ltd., Tokyo, and Hamburg, Germany). In addition, routine echocardiography was performed before angiography for all patients.
Anthropometric measurements were conducted with all participants wearing light clothes and without shoes after 8 hr overnight fast. WC was measured from the subcostal region at the level of the umbilicus when the patient was standing and the hands were extended laterally. Hip circumference was measured from the most protruding part of the gluteal region posteriorly and the symphysis pubis anteriorly. Measurements were performed at least twice by the same person. The average of the measurements was recorded. Some indexes were calculated as follows:

Angiographic analyses
Coronary angiography was performed using the standard Judkins technique. SxS was used to evaluate the severity of CAD. 13 SxS was calculated by two experienced interventional cardiologists who were blind to the patients' clinical data. Then, the mean of the two measures was calculated. Patients were divided into three groups (low-risk SxS <22, 32 ≥ intermediate-risk SxS ≥22, high-risk SxS ≥33) according to the SxS international accepted scoring.
Statistical analysis
Statistical analysis was performed by IBM SPSS Statistics for Windows (Version 22.0; Armonk, NY). Categorical variables are expressed as number and percentages, continuous variables are expressed as median ± standard deviation or median (interquartile range). The chi-squared test was used for the assessment of categorical variables in between groups with low, intermediate, and high SxS. Among these groups, at first, distribution pattern of the continuous variables was determined by the Kolmogorov–Smirnov test for the analysis of the continuous variables; variables showing normal distribution pattern were assessed by one-way analysis of variance (ANOVA) test; variables not showing normal distribution pattern were assessed by the Kruskal–Wallis test.
The homogeneity of variances was assessed by Levene's test for the variables used in the ANOVA test. In the case of significant differences among groups, post hoc analyses were performed by using the Tukey test or the Bonferroni correction. One variable logistic regression analysis was performed at first for the assessment of predictivity of the VAI with high SxS. Regression models were developed by adding possible confounding variables and multiple regression analysis were performed for the assessment of the predictive power of VAI, and predictive power of VAI with high SxS. A type I error level of 5% was used for statistical significance.
The results of the study by Sahin et al. 14 were used to calculate the minimum required sample size. A priori minimum required sample size that was calculated based on an alpha of 0.05 and a power of 85% for VAI was 228.
Results
A total of 253 patients were included in the study. Demographic features and laboratory parameters of the study groups are presented in Table 1. The frequency of male gender was significantly lower in the low SxS group compared with the other groups. The platelet count (P = 0.016) and C-reactive protein levels (P = 0.001) were higher in the high SxS group compared with the other groups (Table 1). Anthropometric measures of the study patients are given in Table 2. WHR was significantly lower in the low SxS group compared with the other groups [low vs. intermediate vs. high: 0.88 (0.79–1.02) vs. 0.94 (0.82–1.04) vs. 0.94 (0.86–1.13), respectively; P = 0.0038]. VAI was found significantly higher in the high SxS group compared with the other groups [low vs. intermediate vs. high: 1.88 (1.41–2.29) vs. 1.87 (1.41–2.38) vs. 2.17 (1.65–2.77), respectively; P = 0.021].
Demographic Features and Laboratory Parameters of the Study Groups
Statistically significant results (P < 0.05) were shown in bold type.
Denotes statistically significant column.
CRP, C-reactive protein; HDL, high-density lipoprotein; LDL, low-density lipoprotein; WBC, white blood cell count.
Anthropometric Measures of the Study Groups
Statistically significant results (P < 0.05) were shown in bold type.
Denotes statistically significant column.
BAI, body adiposity index; BMI, body mass index; LAPI, lipid accumulation product index; VAI, visceral adiposity index; WHR, waist-to-hip ratio; WHtR, waist-to-height ratio.
Different models were generated by logistic regression analysis to evaluate the relationship between the VAI and the high SxS. In Model 1, unadjusted association between VAI and high SxS was demonstrated. In Model 2, other anthropometric measurements were added to Model 1 as potential confounders. In Models 3, 4, and 5, other potential clinical and laboratory variables were added to the prior models. In each model, VAI was found to be an independent predictor of high SxS in our study population (Table 3). Receiver operating characteristic curve analysis revealed that the value of VAI ≥2.048 can predict the presence of a high SxS with a sufficient accuracy (60.8% sensitivity and 61.5% specificity area under the curve: 0.608; 95% confidence interval: 0.530–0.686; P = 0.006) (Fig. 2).

ROC curve for visceral adiposity index as a predictor of high syntax score. ROC, receiver operating characteristic.
Logistic Regression Models Evaluating the Impact of Visceral Adiposity Index on Predicting High Syntax Score
Discussion
This study showed that VAI is an independent predictor of severity of CAD in patients with SAP and type 2 DM. In addition, VAI may predict the presence of high SxS with adequate specificity and sensitivity.
CAD is an important cause of morbidity and mortality worldwide. 1 Cardiovascular mortality is two to three times higher in men with DM and three to five times higher in women with DM compared with the patients without DM. 15 Cardiovascular diseases are responsible for 70%–80% of deaths among patients with DM, and three quarters of these deaths are related to CAD. 15 Furthermore, silent ischemia, which is more frequent in patients with DM, contributes to increased mortality by causing difficulties in the diagnosis of cardiovascular diseases. 16
Concomitant cardiovascular risk factors (hypertension, dyslipidemia, obesity, etc.) are also more common in patients with DM than those without DM. 15 The main goal is the prevention of chronic complications, especially cardiovascular complications in the management of DM. 15 For these reasons, various screening recommendations have been made in patients with DM, in whom it is aimed to reduce cardiovascular mortality and morbidity. 16
Obesity is one of the leading causes of cardiovascular morbidity and mortality. 3 Visceral adipose tissue excess is one of the most important factors responsible for these negative outcomes of obesity. It has been shown that excess visceral adipose tissue leads to impaired insulin sensitivity, increase in proinflammatory adipokines, and a higher incidence of type 2 DM. 3,17 In addition, visceral adipose tissue excess also leads to atherosclerosis via the inflammatory “atherothrombotic pathway.” 18
Recently, cardiovascular risk has been found to be different in persons with different fat tissue distribution even with similar total fat mass. 19 Even though persons are at a normal weight, the distribution of adipose tissue may lead to an increase in cardiovascular risk. Cardiovascular risk is much more in persons who have intra-abdominal or visceral fat accumulation. Although some populations have a low BMI, they have more tendency to the cardiovascular events due to visceral fat accumulation and insulin resistance. 19,20
Recently, various anthropometric measurement scores such as BAI and LAPI have been proposed for the assessment of cardiovascular risk in obesity in addition to measurements such as BMI, WC, and WHR. 2,5,12 These scores have been developed to be able to make better predictions on visceral adiposity. Also, a score named VAI has been developed, which consists of anthropometric measurements, triglyceride, and HDL-C. 2 It has been reported that VAI can be used to differentiate subcutaneous and visceral adipose tissues and gives better information about visceral adipose tissue compared with other scoring systems. 2
It has been shown that VAI is associated with cardiovascular diseases in several studies. 2,21 Similarly, it has also been shown that VAI also correlates with the coronary calcium score (measured by coronary CT), which gives information about subclinical atherosclerosis. 22 In addition, it is reported that VAI is a predictor of cardiovascular events in chronic kidney patients 23 and in patients with prehypertension and hypertension. 24 In our study, we found that VAI can provide information about the CAD severity in patients with type 2 DM similar to the literature.
The best treatment in the management of cardiovascular diseases is disease prevention. Therefore, clinicians should evaluate patients' modifiable risk factors for cardiovascular disease. It is crucial to identify the patients with a higher cardiometabolic risk, even if they have similar demographic characteristics. Therefore, indexes such as VAI can be used to detect visceral adiposity, which leads to increased cardiovascular risk.
The strengths of the study are that it has a prospective design and the patients included in the study are well characterized. In addition, VAI had not been evaluated in this patient group previously, and VAI was evaluated in different models in the present study. This study has several limitations. First, the sample size was relatively small. Second, the causality relationship between VAI and our results could not be established since this was a cross-sectional study. Third, there was a statistical difference between groups in hypertension and gender, but despite this, VAI was determined as an independent predictor of SxS.
In conclusion, we found that VAI was an independent predictor of the SxS, which indicates the severity of CAD in patients with SAP and type 2 DM. So, it can be thought that VAI, which can be calculated with simple measurements, may be used for cardiac risk classification in patients with type 2 DM. Further prospective studies with a larger sample size are needed for the confirmation of the results obtained with this study and its widespread use in clinical practice. Our findings may be enlightening for further studies.
Footnotes
Authors' Contributions
Concept—M.C. and A.Ş. Design—M.C., E.K., and B.C. Materials—M.C., B.C., and S.N. Data collection and/or processing—B.C. and S.N. Analysis and/or interpretation—M.C., E.K., and A.Ş. Literature search—M.C. and B.C. Writing and critical review—M.C. and A.Ş. All authors have read and agreed to the published version of the article.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.