
Abstract
Background:
The prevalence of nonalcoholic fatty liver disease (NAFLD) is rapidly growing in China, especially in patients with type 2 diabetes mellitus (T2DM). Weight loss strategies have been shown to treat NAFLD effectively. We conducted a 24-week, prospective, randomized study in T2DM patients with NAFLD to evaluate the effects of a 5:2 fasting diet on liver fat content.
Methods:
Sixty-one T2DM patients with NAFLD were enrolled and randomly divided into a 5:2 fasting diet intervention group (5:2 diet group, n = 31) and 1.8 mg/day liraglutide intervention group (Lira group, n = 30). The study was performed for 24 weeks. Data of the body weight, waist circumference, plasma lipids and glucose profile, fasting plasma insulin, and liver function parameters were collected. Controlled attenuation parameter (CAP) was measured to assess the liver fat content. Superoxide dismutase (SOD) and malondialdehyde (MDA) were measured to evaluate oxidative stress status.
Results:
At 24 weeks after intervention, compared with those at baseline, CAP was significantly decreased in both the 5:2 diet group and Lira group, which was 7.4% and 5.5%, respectively. Body weight, plasma lipids and glucose profile, and liver function parameters improved significantly, while homeostasis model assessment-β (HOMA-β) was significantly increased in both groups (all P < 0.05). Stepwise linear regression showed that increased HOMA-β and SOD, as well as reduced body mass index (BMI), were the independent predictors of CAP decrease in the Lira group (P = 0.000, 0.000, 0.015). In contrast, reduced BMI and MDA were the independent influencing factors of CAP decrease in the 5:2 diet group (P = 0.011, 0.043). The common side effects in the 5:2 diet group were hunger (60%), weakness (10%), and constipation (0.3%).
Conclusions:
A 5:2 fasting diet achieved comparable effects with liraglutide on liver fat content in patients with T2DM with NAFLD by reducing BMI and oxidative stress. Both treatment strategies were safe and effective for glucose control.
Introduction
Nonalcoholic fatty liver disease (NAFLD) is characterized by steatosis and may progress to nonalcoholic steatohepatitis (NASH), leading to fibrosis and hepatocellular carcinoma. 1 In China, the prevalence of NAFLD was ∼29.8%. 2 Obesity, metabolic syndrome, and type 2 diabetes mellitus (T2DM) are risk factors for liver fibrosis progression in patients with NAFLD. 3 Weight loss strategies or medicines such as glucagon-like peptide-1 receptor agonists (GLP-1RA) are effective in improving NAFLD. 4,5
Intermittent fasting has been reported effective in weight loss and glycemic control in patients with diabetes 6 and patients with NAFLD. 7 A 5:2 fasting diet strategy is an intermittent fasting pattern in which a zero or very low energy diet is permitted on 2 inconsecutive days and normal diet on the other 5 days. 8 Several studies in the last decade have demonstrated that a 5:2 fasting diet was as effective as continuous energy restriction (CER) on weight loss and metabolic disorder improvement. 9,10 However, only few studies have reported the effect of a 5:2 fasting diet on NAFLD in patients with T2DM. Therefore, a 24-week, prospective randomized study was performed in the present study to explore the effects of a 5:2 fasting diet strategy on NAFLD in patients with T2DM, compared with 1.8 mg/day liraglutide treatment.
Participants and Methods
Participants
Patients with T2DM with NAFLD aged 18–60 years were recruited from the First Central Hospital of Baoding City from February 1, 2020, to October 30, 2020. NAFLD was diagnosed according to Clinical Practice Guidelines for the management of NAFLD recommended by the European Association for the Study of Diabetes. 1 The study was approved by the Ethics Committee of the First Central Hospital of Baoding City (Approval Nos. 2020037 and 2020073). All patients signed informed consent.
Exclusion criteria: body mass index (BMI) <28 or >35 kg/m2; fasting glucose ≥9.0 mM; glycated hemoglobin (HbA1c) ≥8.0%; alcohol consumption >210 grams/week for males or 140 grams/week for females; alanine aminotransferase (ALT) or aspartate aminotransferase (AST) >3 times the upper normal limit; hepatic fibrosis or liver cancer; other types of liver disease; and treatment with medicine, including thiazolidinediones, dipeptidyl peptidase-4 inhibitor, insulin, insulin secretagogues, or any liver protectants that have impacts on liver fat, islet function, or liver enzyme within 2 weeks before enrollment.
Intervention
A total of 61 patients with T2DM with NAFLD were enrolled and randomized into the 5:2 fasting diet intervention group (5:2 diet group, n = 31) or the liraglutide intervention group (Lira group, n = 30). Patients in the 5:2 diet group received a 5:2 fasting diet, which included 5 days of regular diet and 2 inconsecutive days of 500 kcal/day diet. Patients were required not to overeat on regular diet days. Nutrition and protein intake were adequate during the study based on dietary guidelines. 11 Energy supply was recommended as follows: 45%–50% carbohydrates, 15%–20% protein, and 30%–35% fat. Patients in the Lira group received liraglutide treatment (Novo Nordisk A/S, Bagsvaerd, Denmark) at an initial dose of 0.6 mg once daily, which was increased by 0.6 mg/week until 1.8 mg/day. None of the participants took other antihyperglycemic agents or lipid-lowering medicine. Patients in the Lira group only received general dietary guidance. All participants were required to exercise half an hour every 2–3 days without supervision. Two professional nutritionists were responsible for diet and exercise guidance, and the discomfort reactions of patients were recorded. Hypoglycemia was defined as blood glucose ≤3.9 mM. The whole intervention lasted for 24 weeks.
Clinical data collection
Clinical data were obtained before and at 24 weeks after treatment. Body weight and waist circumference (WC) were measured. Fasting plasma glucose (FPG), plasma lipids profile, and liver function parameters were measured by enzymatic colorimetric methods; HbA1c was measured by high-performance liquid chromatography, and insulin was detected by the electrochemiluminescence method. Insulin resistance and β-cell function were evaluated by homeostasis model assessment (HOMA). Homeostasis model assessment of insulin resistance (HOMA-IR) = insulin (mIU/L) × FPG (mM)/22.5; HOMA-β = 20 × insulin (mIU/L)/[FPG (mM) −3.5].
Oxidative stress measurement
Superoxide dismutase (SOD) activity and malondialdehyde (MDA) level were measured using the Superoxide Dismutase Activity Assay Kit (Colorimetric; No. G0101W; Grace Biotechnology Company) and the MDA Assay Kit (Colorimetric; No. G0109W; Grace Biotechnology Company), respectively.
Liver fat content measurement
Controlled attenuation parameter (CAP) was measured after overnight fasting by transient elastography using the FibroScan® device (Echosens, Paris, France) and a 3.5-MHz M probe. Two experienced professionals performed the measurement.
Statistical analysis
SPSS 22.0 software (IBM Corp., Armonk, NY) was used for statistical analysis. Continuous variables are presented as mean ± standard deviation. Comparison of data between two groups was conducted by Student's t-test if the variance was homogeneous; otherwise, Wilcoxon's rank test was used. Differences within the same group were analyzed by paired t-test. Categorical variables were compared using the chi-squared test. Stepwise multivariate linear regression was performed to determine the independent factors of the reduction of CAP. P < 0.05 was considered statistically significant.
Results
Metabolic parameters
There were no significant differences between the two groups with respect to baseline characteristics (all P > 0.05) (Table 1).
Characteristics of Two Strategies Before and at 24 Weeks After Treatment
P < 0.05 for comparison of indexes before and after treatment within groups.
P < 0.05 for comparison of indexes at the end of 24 weeks between groups.
P < 0.05 for comparison of changes between groups.
5:2 Diet group, 5:2 fasting diet intervention group; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; FPG, fasting plasma glucose; HbA1c, glycated hemoglobin; HDL-C, high-density lipoprotein cholesterol; HOMA-β, homeostasis model assessment-β; HOMA-IR, homeostasis model assessment of insulin resistance; LDL-C, low-density lipoprotein cholesterol; Lira group, liraglutide intervention group; NASH, nonalcoholic steatohepatitis; TG, triglycerides; WC, waist circumference.
Compared with those at baseline, body weight, BMI, WC, low-density lipoprotein cholesterol (LDL-C), triglycerides (TG), FPG, HbA1c, HOMA-IR, ALT, and AST were all significantly decreased, whereas high-density lipoprotein cholesterol (HDL-C) and HOMA-β were significantly increased at 24 weeks after a 5:2 fasting diet or liraglutide treatment (all P < 0.05) (Table 1).
At the end of the study, the 5:2 diet strategy achieved similar effects with liraglutide treatment on body weight, BMI, WC, LDL-C, HDL-C, HbA1c, HOMA-IR, HOMA-β, ALT, and AST (all P > 0.05) (Table 1). Interestingly, TG and FPG were significantly lower, and the decline of FPG and HbA1c was more obvious in the Lira group than in the 5:2 diet group, indicating that except for TG and glucose profile, a 5:2 fasting diet might achieve comparable effects with liraglutide treatment in terms of weight loss, liver function, and insulin resistance improvement in patients with T2DM with NAFLD.
Oxidative stress
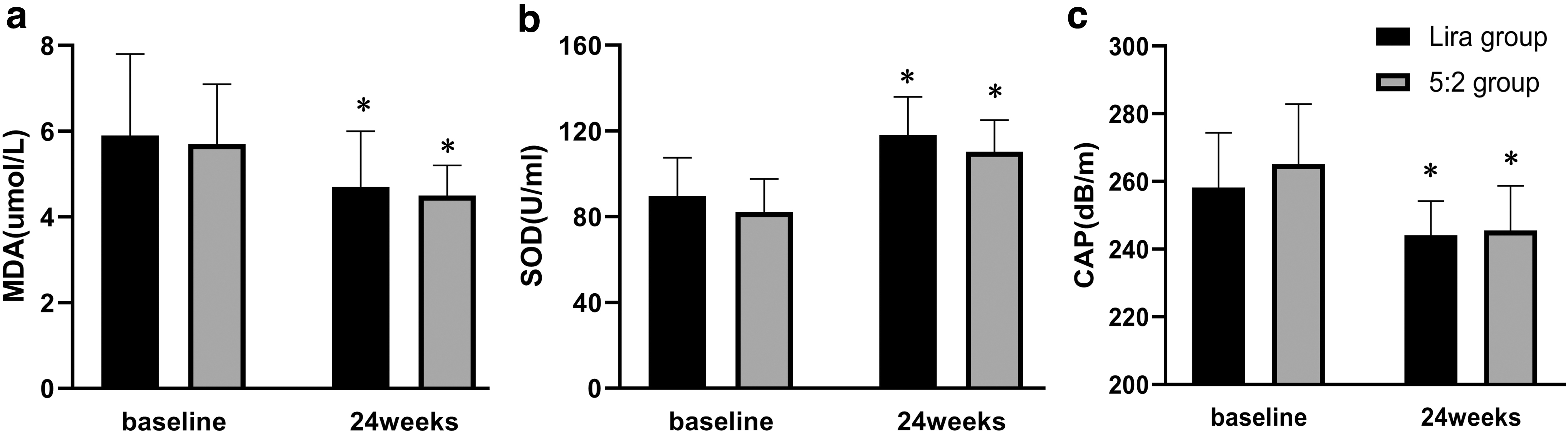
Decreased MDA levels and increased SOD activity were found in both the 5:2 diet group and Lira group at the end of 24 weeks, compared with those at baseline (all P < 0.05) (Fig. 1a, b), suggesting that both treatments might improve oxidative stress in patients with T2DM with NAFLD. In addition, at 24 weeks after intervention, no significant differences were found in MDA level and SOD activity between the 5:2 group and the Lira group (all P > 0.05) (Fig. 1a, b), indicating that to a certain extent, 5:2 fasting diet might exert similar effects on oxidative stress improvement with liraglutide treatment.
The level of MDA
Liver fat content
CAP was significantly decreased at 24 weeks after 5:2 fasting or liraglutide treatment compared with the baseline data (all P < 0.05) (Fig. 1c). However, there was no significant difference in CAP between the two groups both at baseline and at the end of 24 weeks (all P > 0.05) (Fig. 1c), indicating a similar performance of a 5:2 fasting diet and liraglutide in improving fatty liver.
The severity of liver steatosis was significantly improved at 24 weeks after treatment in the Lira and 5:2 groups; however, there was no difference between the two groups (Fig. 2).

Number of patients with different level of CAP before and at 24 weeks after treatment. White bar: CAP <238 dB/m, Gray bar: 238 dB/m < CAP <258 dB/m, black bar: CAP >258 dB/m. At 24 weeks after treatment, the number of patients with CAP <238 dB/m and 238 dB/m < CAP <258 dB/m increased, and the number of patients with CAP >258 dB/m decreased in both groups.
Correlations of CAP decrease with clinical variables
The reduction of CAP was positively correlated with the changes in body weight, BMI, and MDA and negatively correlated with the change in SOD both in the 5:2 diet group (r = 0.445, 0.478, −0.417, all P < 0.05) and in the Lira group (r = 0.417, 0.461, −0.593, all P < 0.05) (Table 2). The reduction of CAP was positively correlated to the alteration of WC and FPG and negatively correlated with the alteration of HOMA-β only in the Lira group (r = 0.408, 0.489, −0.685, all P < 0.05) (Table 2).
Correlations Between the Decrease of Controlled Attenuation Parameter and Clinical Variables
Δ, Change in; MDA, malondialdehyde; SOD, superoxide dismutase.
Independent factors of CAP decrease
Variables significantly correlated with CAP reduction were included in the stepwise linear regression model. Age and sex, as the potential confounding factors, were also included. Increased HOMA-β and SOD and reduced BMI were the independent predictors of CAP decrease in the Lira group (P = 0.000, 0.000, 0.015) (Table 3), contributing to a 72.3% CAP reduction. Decreased BMI and MDA were the independent influencing factors of CAP decrease in the 5:2 diet group (P = 0.011, 0.043) (Table 3), contributing to a 33.5% CAP reduction (Table 3).
Multiple Linear Regression Analysis of the Reductions of Controlled Attenuation Parameter
β, standardized coefficient; R 2, coefficient of determination; SE, standard error.
Safety
No hypoglycemic event was observed in the two groups. In the 5:2 diet group, the common symptoms were hunger (60%), weakness (10%), and constipation (0.3%). No hunger was reported on every fasting day. In the Lira group, two patients were withdrawn due to nausea, vomiting, and diarrhea. All adverse effects disappeared when the treatment was terminated. Mild digestive symptoms were reported in three patients, and the symptoms disappeared with the prolonged treatment.
Discussion
NAFLD and metabolic syndrome share several pathogenetic features, including insulin resistance, oxidative stress, and lipid peroxidation. 12 Evidence suggested a close link between NAFLD and increased cardiovascular risk regardless of age, sex, cholesterolemia, and other elements of metabolic syndrome. 13 Liraglutide, as a glucose-lowering medicine, is effective in reducing body weight and liver fat content, 14 improving metabolic disorder, insulin resistance, 15,16 and oxidative stress 17 in patients with T2DM and NAFLD. Clinical evidence also indicates that liraglutide may significantly lower major adverse cardiovascular events. 18 Several benefits were achieved independent of its glucose lowering effects. 19 To our knowledge, this study is the first to investigate the effect of a 5:2 fasting diet on liver fat content, compared with liraglutide, in patients with T2DM with NAFLD in China. The results showed that the 5:2 fasting diet was comparable with liraglutide in improving BMI, oxidative stress, insulin resistance, liver fat content, and hepatic function in patients with T2DM with NAFLD.
CER has been considered to be beneficial in weight loss and NAFLD improvement. 20 Carter et al. found that a 5:2 fasting diet and CER diet had similar effects on glycemic control and weight loss in patients with T2DM. 21 Conley et al. reported comparable effects of a 5:2 fasting diet and CER diet on weight loss and lipid metabolism improvement. 22 Nevertheless, a 5:2 fasting may be more adaptable to people with different lifestyles and work schedules. 23
Few data are available regarding the effect of 5:2 fasting on patients with NAFLD. However, it has been found that periodic fasting might lead to improved fatty liver index, which was correlated with the number of fasting days and BMI reduction. 24 Holmer et al. also found that a 5:2 fasting diet effectively reduced liver steatosis in patients with NAFLD. 25 A study performed by Vilar-Gomez et al. indicated that a 5%–10% body weight reduction contributed to NAFLD/NASH improvement. 26 In this study, we found that 24 weeks of a 5:2 fasting diet led to 7.3% CAP reduction and 6.1% body weight reduction, consistent with previous data.
Oxidative stress is one of the etiological factors leading to NAFLD. 27 We observed that a 5:2 fasting diet might improve oxidative stress in patients with diabetes with NAFLD. Obesity can cause oxidative stress through endoplasmic reticulum stress in adipocytes. Studies have shown that intermittent fasting can reduce oxidative stress markers, 28,29 which is not solely due to weight loss. 30 In patients with prediabetes whose body weight is maintained, intermittent fasting may lead to reduced plasma levels of 8-isoprostane, a marker of oxidative stress. 31 Clinical studies also found that intermittent fasting might potentiate the antioxidant defense through increasing ketone production in the muscle and circulation in patients with obesity. 32,33 Therefore, a 5:2 fasting diet may improve oxidative stress. However, detailed mechanisms need to be further investigated.
This study also found that a 5:2 intermittent fasting diet might improve liver function and insulin resistance in patients with diabetes with NAFLD. Alternate calorie restriction 7 and Ramadan fasting 34 have been reported to improve liver function, and a 5:2 fasting diet may reduce HOMA-IR in overweight premenopausal women. 35 Intermittent fasting could improve insulin resistance by increasing the level of adiponectin in circulation in patients who are overweight or obese even without fat loss. 36 Intermittent fasting might prompt a “metabolic switch” by targeting several signaling pathways and maintaining metabolic homeostasis and cellular resilience. 8,37 However, further studies are needed regarding detailed mechanisms underlying the effect of a 5:2 diet in improving metabolic disorders.
As we know, liver biopsy is considered the gold standard for diagnosing NAFLD. Masarone et al. found that the prevalence of NAFLD and NASH was 100% and 96.82% separately in patients with T2DM confirmed by liver pathology, suggesting that NASH may be one of the early complications of T2DM. 38 Ultrasound does not reliably detect steatosis in the early stages, and liver biopsy is limited due to its invasive operation. Vibration-controlled transient elastography may achieve reasonable accuracy without invasive damage. 39,40 In our study, we explored a more practical and less invasive method to evaluate liver fat content. CAP reduction was 19.5 ± 12.2 dB/m in the 5:2 diet group which was consistent with previous studies. 25
The limitation of the study is that hepatic steatosis was assessed by ultrasound rather than liver biopsy, and the data could not be stratified by hepatic steatosis and NASH due to the small sample size.
Conclusion
In conclusion, a 5:2 fasting diet is as effective as 1.8 mg/day liraglutide on liver fat content in patients with T2DM with NAFLD, which may improve liver steatosis by decreasing BMI and oxidative stress. Therefore, a 5:2 fasting diet is a feasible and safe strategy for treating NAFLD in patients with T2DM with mild-to-moderate hyperglycemia.
Footnotes
Authors' Contributions
Y.X. performed the experiments, analyzed the data, prepared the figures, and drafted the article; L.Z. performed the measurement of liver steatosis; Y.Z. designed and supervised the project; Y.L. finalized the article. All authors read and approved the final article.
Acknowledgment
The authors acknowledge Baoding No.1 Central Hospital for providing the data.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This work was supported by Natural Science Foundation of Hebei Province (No. H2021206073).