
Abstract
Objectives:
Machine learning has potential to improve the management of lipid disorders. We explored the utility of machine learning in high-risk patients in primary care receiving cholesterol-lowering medications.
Methods:
Machine learning algorithms were created based on lipid management guidelines for England [National Institute for Health and Care Excellence (NICE) CG181] to reproduce the guidance with >95% accuracy. Natural language processing and therapy identification algorithms were applied to anonymized electronic records from six South London primary care general practices to extract medication information from free text fields.
Results:
Among a total of 48,226 adult patients, a subset of 5630 (mean ± standard deviation, age = 67 ± 13 years; male:female = 55:45) with a history of lipid-lowering therapy were identified. Additional major cardiometabolic comorbidities included type 2 diabetes in 13% (n = 724) and hypertension in 32% (n = 1791); all three risk factors were present in a further 28% (n = 1552). Of the 5630 patients, 4290 (76%) and 1349 (24%) were in primary and secondary cardiovascular disease prevention cohorts, respectively. Statin monotherapy was the most common current medication (82%, n = 4632). For patients receiving statin monotherapy, 71% (n = 3269) were on high-intensity therapy aligned with NICE guidance with rates being similar for the primary and secondary prevention cohorts. In the combined cohort, only 46% of patients who had been prescribed lipid-lowering therapy in the previous 12 months achieved the NICE treatment goal of >40% reduction in non–high-density lipoprotein cholesterol from baseline pretreatment levels. Based on the most recent data entry for patients not at goal the neural network recommended either increasing the dose of statin, adding complementary cholesterol-lowering medication, or obtaining an expert lipid opinion.
Conclusions:
Machine learning can be of value in (a) quantifying suboptimal lipid-lowering prescribing patterns, (b) identifying high-risk patients who could benefit from more intensive therapy, and (c) suggesting evidence-based therapeutic options.
Introduction
Cholesterol-lowering medications are extensively used to reduce the risk of atherosclerotic cardiovascular disease (ASCVD) as primary or secondary disease prevention. 1 However, real-world data demonstrate that implementation of these agents in clinical practice is often suboptimal. 2,3 In the United Kingdom >50% of patients fail to attain cholesterol goals recommended by the National Institute for Health and Care Excellence (NICE). 4 Escalation of lipid-lowering therapy is frequently not implemented. 5 Concerns about inadequate lipid-lowering and failure to achieve treatment goals is not confined to nonspecialist clinical practice. Recent national and international studies that include secondary care centers of excellence in Europe and the United States have shown that lipid-lowering pharmacotherapy for patients at high risk of ASCVD is not fully aligned with expert guidance. 6,7
The therapeutic landscape has become more complicated in recent years. Novel cholesterol-lowering medications must be positioned within existing treatment algorithms. The limitations of statins to lower cholesterol as monotherapy and issues of tolerability have prompted the development of nonstatin cholesterol-lowering drugs. 8,9 Examples include the Niemann–Pick C1-Like 1 protein inhibitor ezetimibe 10 and the adenosine triphosphate citrate lyase inhibitor bempedoic acid. 11 In the United Kingdom, prescribing proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors have been restricted to secondary care specialist services. 12 –14
Precision or personalized medicine aims to provide best care by considering therapeutic options in the context of individual patient characteristics. 15,16 Machine learning technology offers opportunities to facilitate personalized medicine. Patients are stratified according to factors including disease subtype, risk, prognosis, and treatment response. 17,18 The limited impact of machine learning on clinical practice to date may in part reflect the challenges of interdisciplinary research to provide solutions in which clinicians have confidence. 18 Informed by the principles of precision medicine we explored the potential of machine learning to improve the management of cholesterol in a heterogeneous population of primary care patients with a high prevalence of cardiometabolic comorbidities.
Study Objectives
We sought to (a) identify adult patients at high risk of ASCVD and (b) recommend appropriate cholesterol-lowering therapy where therapeutic goals had not been attained. Our approach meshed classical field knowledge, i.e., clinical guidelines, with electronic medical records (eMRs) to provide evidence-based therapy recommendations. Additional focus was placed on the potential role of bempedoic acid, which at the time of the study was being integrated into UK clinical practice according to specific NICE guidance.
Methods
Algorithms
Neural networks were developed to reproduce the relevant NICE guidelines for lipid management guidance for England (CG 181) 12 using a simple feed-forward neural network (3 fully connected layers, 130 neurons in total) with rectified linear unit activations and a sigmoid function as the final layer. Binary cross-entropy was minimized with an equal probability for each therapy to achieve a 99.9% accuracy in predicting the right therapy ( = sample accuracy) and 95.9% accuracy to both predict the right therapy and none of the alternatives ( = patient accuracy). At the time of the study, the principal classes of cholesterol-lowering medications being employed by primary care clinicians were statins and ezetimibe. Inclisiran, an injectable small interfering RNA, which limits production of PCSK9, had not been introduced into UK clinical practice. 19 Nonetheless, because NICE had given provisional approval to use of inclisiran for secondary prevention of ASCVD this option was included in the neural networks alongside PCSK9 inhibitors. 20 National prescribing recommendations (TA694) for bempedoic acid were also incorporated. 21 According to prevailing NICE guidance at this time, bempedoic acid could be used as an adjunct to diet in adults only if statins were contraindicated or not tolerated and when ezetimibe alone was not adequate to attain therapeutic goals. 21 For the purposes of the study, the definition of statin intolerance applied by the neural network assumed that statins were not tolerated at any dose.
Data extraction and processing
Anonymized eMRs from six South London primary care general practices spanning 1988–2021 were extracted. Data from free text fields were analyzed using natural language processing, and therapy identification algorithms were applied to identify patients with a history of lipid-lowering medication. Patients were classified on the basis of Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) codes * into primary or secondary cardiovascular disease prevention cohorts based on the absence or presence of coded cardiovascular disease, respectively. 22 ASCVD was defined as coronary heart disease, stroke, and peripheral artery disease. Primary prevention patients either had a calculated 10-year risk of a cardiovascular event >10% or belonged to high-risk clinical categories for which lipid-lowering therapy is indicated by NICE. 12 Major comorbidities that often contribute to risk of ASCVD, that is, type 2 diabetes and hypertension, 7 were identified from SNOMED codes as were familial hypercholesterolemia and a coded history of statin intolerance.
Efficacy of cholesterol-lowering therapy
A reduction in non–high-density lipoprotein (HDL) cholesterol >40% from pretreatment level was considered the primary marker of therapeutic efficacy, in accordance with NICE guidance. 12 Cholesterol-lowering medication was subdivided into low, medium, and high-intensity statins, that is, specific doses for pravastatin, simvastatin, atorvastatin, and rosuvastatin. 23 Current cholesterol-lowering therapy was defined as active prescriptions within a 30-day range. Therapy recommendations were generated in accordance with current NICE guidance (Table 1).
Recommendations Generated by the Neural Network
ASCVD, atherosclerotic cardiovascular disease; NICE, National Institute for Health and Care Excellence; PCSK9, proprotein convertase subtilisin/kexin type 9.
Clinical safety validation
Safety considerations, for example, contraindications and major drug interactions, were included as integral elements of the neural network. 10,24,25 To ensure that recommendations made by the neural network were aligned with safe prescribing, two experienced clinicians independently performed a detailed review of the neural network recommendations for a randomly selected sample of patient records. The clinical safety validation exercise spanned patients across a range of ages at different stages in the natural history of cardiometabolic comorbidities. The duplicate results were cross-checked to reach a consensus between the clinicians for each record. Minor adjustments to aspects of data extraction and data processing by the neural network were subsequently implemented where indicated.
Data governance
All patient data were anonymized. Only data from living patients who had previously consented to share their data anonymously for research purposes were included in the analysis.
Results
Study population
The total general practice population studied was 48,226 patients. A subset of 5630 patients with a history of treatment with cholesterol-lowering medications was identified. Of these, 76% (n = 4290) and 24% (n = 1340) were in the primary and secondary cardiovascular disease prevention cohorts, respectively (Fig. 1). The mean ± standard deviation age of the 5630 patients was 67 ± 13 years with a male:female ratio of 55:45. Cholesterol levels requiring pharmacotherapy as an isolated risk factor was present in 1540 (27%) patients. Additional major modifiable comorbidities included type 2 diabetes in 13% (n = 724) patients and hypertension in 32% (n = 1791) patients; all three risk factors were present in a further 28% (n = 1552) patients. A diagnosis of familial hypercholesterolemia was coded in 52 (1%) patients. A history of statin intolerance was coded in 230 (4%) patients; of these, 182 were in the primary prevention and 48 in the secondary prevention cohorts, respectively.
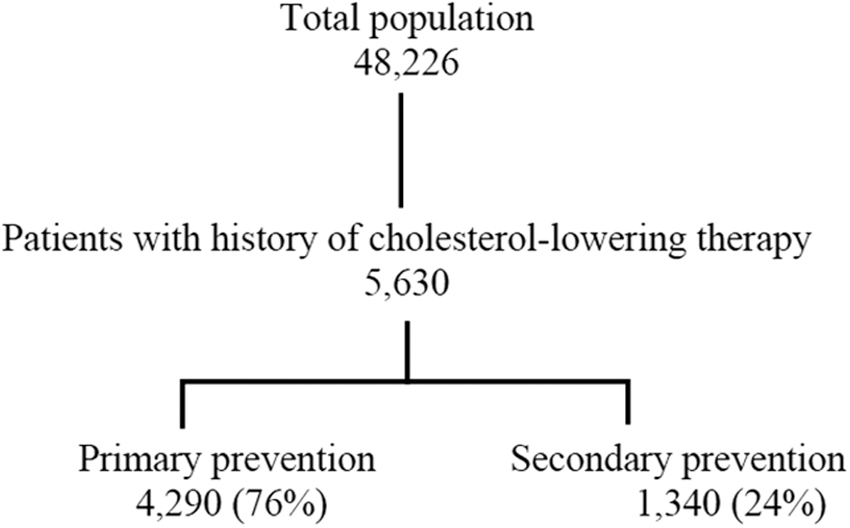
Study population.
Cholesterol-lowering therapy
Prescribing cholesterol-lowering medications gradually increased over time from a low level in the early 1990s to reach a plateau from 2010 onward (data not shown). National prescribing data allied to our own observations from UK primary care settings show that use of more potent second- and third-generation statins—especially atorvastatin—increased between 2010 and 2020. 26 Statin monotherapy was the most common recorded medication at the most recent data entry point (82%, n = 4632) with no difference in rates for the primary and secondary prevention cohorts at 82% (n = 3500) and 84% (n = 1132), respectively. Of the patients treated with lipid-lowering medications the majority (47%, n = 2655) had been prescribed intensive statin therapy as initial pharmacotherapy; therapy had been escalated in a further 29% (n = 1614) patients from a moderate intensity to a high-intensity statin at the time of the analysis.
Among statin-treated patients, 71% (n = 3269) statin monotherapy was high-intensity treatment as per NICE guidance, that is, defined as statins at doses expected to reduce low-density lipoprotein (LDL) cholesterol by >40%. 12 Rates of high-intensity statin use were similar for the primary and secondary prevention cohorts at 70% (2433) and 74% (836), respectively. No current lipid-lowering medication was recorded for the most recent data point in 17% patients in the primary prevention cohort and 11% secondary prevention cohort. Ezetimibe was used either in combination with a statin (n = 184) or as monotherapy (n = 73) with no differences between the primary and secondary prevention cohorts. Among the 184 patients treated with combination statin+ezetimibe the intensity of statin was classed as high in 43 patients, moderate in 12 patients, and low in 129 patients. PCSK9 inhibitor therapy, specifically evolocumab, was identified in a single patient.
Therapeutic goal attainment
Among patients receiving cholesterol-lowering medications within the preceding 12 months 46% failed to achieve the recommended NICE goal of >40% reduction from baseline in non–HDL cholesterol levels. The distribution of goal attainment—as judged by percentage reduction in non–HDL cholesterol from pretreatment levels—was similar for the primary and secondary prevention cohorts (data not shown). This observation held when LDL cholesterol was substituted for non–HDL cholesterol.
Therapy recommendations
Based on the most recent data entry point current cholesterol-lowering therapy was endorsed by the neural network in 40% patients (Fig. 2). The neural network recommended increasing statin dose in 46% patients, adding ezetimibe in 3%, adding bempedoic acid in 1%, or escalating to a PCSK9 inhibitor in 1%. Referral to a specialist lipid clinic for expert clinical advice was recommended in 9% patients where NICE guidance did not provide clear recommendations. As per NICE TA694, that is, interpreting a diagnosis of statin intolerance as indicating no statin therapy at any dose, the neural network identified a total of 78 patients as potential candidates for bempedoic acid at some point during their therapeutic history; of these, 55 were in the primary prevention cohort and 23 in the secondary prevention cohort.

Therapeutic recommendations delivered by the neural network for 2611 patients (%, n) receiving cholesterol-lowering medication based on the last available data point.
Discussion
This proof-of-concept study demonstrates the utility of a neural network to identify patients requiring therapy escalation and to recommend appropriate intensified pharmacotherapy to attain treatment goals in alignment with national management guidelines. We believe our results support the notion that machine learning can help facilitate the aims of precision medicine in managing cholesterol-lowering medication in high-risk patients.
The study demonstrates the value of machine learning to quantify misalignments between national clinical guidance and real-world prescribing of cholesterol-lowering medications. Statins were the most commonly used lipid-modifying pharmacotherapy in our study, as recommended by the guidelines. However, the intensity of statin therapy was suboptimal in approximately one-third patients. Greater use of high-intensity statins was advocated in the 2014 update of NICE guidance; this concept had become well established in UK clinical practice by the time of our study. 12 Failure to attain cholesterol goals in the era of high-intensity cholesterol-lowering therapy has been reported in other surveys of the UK primary care prescribing. 4,23 The similarity of the degree of non–HDL cholesterol lowering for primary and secondary prevention suggests similar therapeutic decisions and/or adherence to cholesterol-lowering therapy for both cohorts.
The algorithms uncovered not only widespread statin underdosing but also evidence of inadequate monitoring of therapeutic response (data not shown). According to NICE guidance operative at the time of the study, low- or medium-intensity statin therapy was restricted to individuals with statin intolerance, patient preference, or drug interactions. 12,27 We suspect that some cases of statin intolerance may not have been recorded in the eMR. 28 Statin intolerance is associated with suboptimal lipid-lowering and hence higher risks of ASCVD. 29,30 We consider that the 4% prevalence of recorded statin intolerance in our study may be an underestimate since under-reporting of statin intolerance has been documented in the United Kingdom and elsewhere. Some studies have estimated rates of ∼10%–15%. 31 A recent international meta-analysis of randomized controlled trials (RCTs) and real-world data involving >4 million patients found an overall global prevalence of statin intolerance of 9.1%. 32 The prevalence of statin intolerance when diagnosed using defined clinical and laboratory criteria was higher in real-world cohorts than among participants in RCTs. While the Cholesterol Treatment Trialists' Collaboration concluded that statin therapy causes a small excess of mostly mild muscle pain, the clinical challenge of statin intolerance or reluctance remains a barrier to cholesterol goal attainment. 33
Patients receiving suboptimal pharmacotherapy are potential candidates for additional or alternative lipid-modifying therapy. 34,35 The algorithms trained on NICE guidance endorsed current cholesterol-lowering therapy in 40% of the patients. For the remaining patients, an increase in statin dose was the most frequent recommendation in nearly half of the patients requiring more intensive therapy. In parentheses, our neural networks have the capability to quantify the gap between the non–HDL cholesterol and therapeutic goal at the level of individual patients (data not shown). Such additional information could help prioritize care by focusing on patients who are furthest from target and hence who might benefit most from a change in cholesterol-lowering therapy. Moreover, the neural networks can identify and quantify therapeutic inertia in prescribing cholesterol-lowering medications (data not shown). We are developing a complementary ambient machine-learning solution that integrates with primary care eMR systems to support personalized medicine in the context of complex comorbid cardiometabolic diseases using our neural networks.
The addition of nonstatin medications, injectable therapies or referral to specialist lipid clinics in secondary care was proposed by the neural networks for some patients. Clinical guidelines for treating patients at high cardiovascular risk generally advocate maximally tolerated doses of statins and other drugs to achieve recommended lipid levels or relative reductions of LDL cholesterol or non–HDL cholesterol. 36 In accordance with NICE guidance that was in place at the time of the study, nonstatin oral therapies, ezetimibe and bempedoic acid, were recommended by the algorithms in 3% and 1% patients, respectively. Ezetimibe can be used in combination with statins or as monotherapy. Support for the efficacy of ezetimibe on ASCVD comes from clinical trial data showing reductions in major adverse cardiovascular events in high-risk groups. 10,37 Our results imply that ezetimibe was not being used in accordance with NICE guidance in all eligible patients, that is, added to statin if a 40% reduction in non-HDL cholesterol is not achieved. Bempedoic acid is an effective cholesterol-lowering drug with a novel mechanism of action. 38 Dose–response models predict that combining bempedoic acid with the lowest dose of commonly used statins would achieve a similar degree of LDL cholesterol lowering as quadrupling the statin dose. 39 The prescribing of bempedoic acid in England was subject to restrictions at the time of our study pending the results of cardiovascular outcome trials. 40 According to TA694 guidance, use of bempedoic acid was permissible only if statins were contraindicated or not tolerated and when ezetimibe alone did not adequately control LDL cholesterol. 21 Thus, under the most stringent interpretation of TA694 bempedoic acid either as monotherapy or in combination with statins at any dose was not sanctioned by NICE. For the purposes of our study the neural networks were aligned with this interpretation of the guidance. That said, it should be noted that at the time of our analysis there was a degree of uncertainty among lipid specialists whether the TA694 guidance could potentially be interpreted more liberally to include patients on suboptimal doses of statins. † The US National Lipid Association has defined complete statin intolerance as inability to take any lipid-lowering dose, whereas partial intolerance denotes maximal tolerated doses that fail to achieve therapeutic objectives. 34 A less restrictive definition of statin intolerance would have been expected to increase the number of potential candidates for bempedoic acid in our study because patients with partial statin intolerance would also have become eligible. The impact of changes to prescribing guidance can be readily assessed using the neural network.
The identification of a solitary patient being treated with a PCSK9 inhibitor reflects the generally low level of prescribing for these injectable cholesterol-lowering drugs in England. The constraint that prescribing of PCSK9 inhibitors was confined to secondary care cardiology and lipid clinics may be relevant to this observation. 36
Strengths of our study include a low probability of prescribing bias reflecting NICE guidance and the highly structured primary care eMR system in England. However, caveats and limitations should be considered. First, owing to the UK data governance restrictions no information was available on deceased patients. This limitation applies to mortality from any cause and was not confined to deaths from cardiovascular disease. Whether patients who died from cardiovascular disease had clinical characteristics, for example, greater levels of comorbidity or responses to cholesterol-lowering therapy that were different to the participants, cannot be determined from our analysis. We aim to address these issues in future studies. Second, although our study was principally concerned with common forms of polygenic cholesterol disorders, it should be noted that recorded prevalence of familial hypercholesterolemia was low. In the absence of universally agreed diagnostic criteria underdiagnosis of familial hypercholesterolemia is well recognized in the United Kingdom and elsewhere. 41 Third, missing eMR data reduced the accuracy of some of aspects of the analyses.
To summarize, our results provide support for the utility of machine learning data-science analytics to (a) identify suboptimal cholesterol-lowering prescribing, (b) identify high-risk patients who might benefit from more intensive therapy, and (c) recommend evidence-based next-step therapeutic options aligned with national guidance. Our results are consistent with recent audits that have identified underuse of combination cholesterol-lowering therapies. 42 Our study also demonstrates the utility of machine learning to model specific prescribing scenarios.
Footnotes
Acknowledgments
The authors thank Professor Richard Barker, Dr. Serge Umansky, and Dr. Jonathan Serjeant for helpful insights from conception to analysis and interpretation of this study. Arthur Pere contributed to data extraction. The authors also thank the Daiichi Sankyo UK Ltd Medical Affairs Team; Farhan Mughal, Shahil Lodhia, Dr. Peter Smith, Nitasha Vekaria, and Laura Redhead for their contributions and input into the concept and article. Part of the software library that was used for this study was developed during internships by Valentin Bruttin, Lisa Fournier, Hugo Michel, and Jude Wells.
Authors' Contributions
A.J.K.: Conceptualization, methodology, validation, analysis, writing, visualization, supervision, funding acquisition. G.H.-H.: Methodology, analysis, writing. X.Z.: Methodology, analysis, writing, visualization. N.P.: Analysis, writing, resources, data curation. A.J.: Conceptualization, methodology, validation, analysis, data curation, writing, resources, visualization, supervision.
Author Disclosure Statement
The authors report no other competing interests in this work.
Funding Information
The study was conceived and performed by Metadvice and King's College London. Daiichi Sankyo UK Ltd. funded and had input into the study. Daiichi Sankyo Europe GmBH are marketing authorization holders of bempedoic acid and the bempedoic acid/ezetimibe combination in the United Kingdom, European Economic Area, and Switzerland.