
Abstract
Background:
Prostatic growth has been thought to be the systemic manifestation of some metabolic derangements in recent studies. Nonalcoholic fatty liver disease (NAFLD), a hepatic manifestation of the metabolic syndrome, might be closely linked with benign prostate hyperplasia and lower urinary tract symptoms (BPH/LUTS). Several studies have been conducted regarding NAFLD and BPH/LUTS association. However, the results are yet to reach a clear conclusion. We aimed to gather these studies' results to make a more robust analysis through a systematic review and meta-analysis.
Methods:
We systematically searched Pubmed-Medline, Cochrane Library, and Science Direct databases. We excluded all experimental studies, case reports, and reviews. Our search was restricted to the English language. We used standard mean difference for BPH/LUTS-related parameters. We identified the study qualities by the Newcastle–Ottawa Scale. We conducted a publication bias analysis.
Results:
A total of six studies involving 7089 participants fulfilled the inclusion criteria. Our meta-analysis revealed that patients with NAFLD have larger prostate volume [0.553 (0.303–0.802), P ˂ 0.001; Q = 97.41; P-value for heterogeneity = P < 0.0001; I 2 = 94.86%]. However, the summary effect size of the other parameters of BPH/LUTS (prostate-specific antigen and international prostate symptom score) computed in our meta-analysis did not yield significant results.
Conclusions:
The prostate size was larger in patients with NAFLD, but the meta-analysis did not reach a significant result for LUTS among the studies. These results should be tested with well-designed studies, in particular, to clarify the association of LUTS with NAFLD.
Introduction
Benign prostate hyperplasia and associated lower urinary tract symptoms (BPH/LUTS) is one of the most frequent disorders in the aging population. Men higher than 50 years old are likely to have prostate enlargement. 1 A histologically enlarged prostate does not always lead to symptoms, but LUTS might be bothersome for aging men.
BPH symptoms are related to the storage and voiding phase of the lower urinary tract. Several surgical and medical therapies for alleviating BPH symptoms have been in clinical use in recent years. However, the exact cause-and-effect relationship for the underlying etiology of prostate enlargement is yet to be clarified. Androgens, estrogens, stromal–epithelial interactions, growth factors, and neurotransmitters may play a role in the etiology of the hyperplastic process. 2 –4 An additional source of growth factors might be the inflammatory cells. 5 Accordingly, metabolic syndrome (MetS), in which chronic inflammation is the joint entity, might be closely related to the etiopathogenesis of BPH/LUTS.
Many studies have been conducted on the association between BPH/LUTS and MetS. These studies indicated that patients with MetS have increased prostate volume and international prostate symptom score (IPSS) scores and need surgery for BPH. 6 –8 Non-alcoholic fatty liver disease (NAFLD), the fat accumulation in the liver without excessive alcohol intake, is the hepatic manifestation of MetS. 9 NAFLD reflects metabolic derangements, including insulin resistance, dyslipidemia, diabetes, and obesity. Furthermore, BPH/LUTS and NAFLD are more prevalent in the aging population. This knowledge has led investigators to search for the possible relationship between BPH/LUTS and NAFLD. Several studies have been conducted on this issue, but these studies yielded conflicting findings. In this meta-analysis, we sought to gather these studies' results to reach a more decisive conclusion.
Methods
Search strategy
We searched PubMed-Medline, Embase (notably Science Direct), and Cochrane databases (Search Trials) to find the related articles from inception until June 2022. The search terms used are as follows: benign prostate enlargement, benign prostate hyperplasia, LUTS, NAFLD, and hepatosteatosis. The search was restricted to the English language. The meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guideline. 10 The PRISMA 2020 checklist was filled and demonstrated as a Supplementary File S1.
Study inclusion and evaluation
We evaluated the articles regarding the association between NAFLD and BPH/LUTS. Among the articles, those presenting the BPH/LUTS parameters [prostate volume, IPSS, prostate specific antigen (PSA)] with the mean and standard deviation were included in the meta-analysis. The articles which do not have the relevant data for pooling analysis were excluded. Some studies which provided the BPH/LUTS parameters with different effect sizes (such as linear regression or correlation analysis) were also excluded since we did not find it suitable to convert these effect sizes to standard mean differences (SMDs). We also excluded the articles of reviews or meta-analyses, comments, editorials, case reports, letters, meeting/congress abstracts, animal experiments, and those published in the non-English language.
After an extensive review of each study, we extracted the data as follows: first author's last name, publication period and country of the population, type of study design, cohort size, age range, NAFLD assessment method, and BPH/LUTS parameters. Among the parameters, LUTS was evaluated by IPSS. It is an eight-item questionnaire comprising seven symptom questions and one quality of life question. The IPSS is categorized as “asymptomatic” (0 points), “mildly symptomatic” (1–7 points), “moderately symptomatic” (8–19 points), and “severely symptomatic” (20–35 points). The studies included in our meta-analysis used the IPSS to identify the LUTS. We pooled their scores to compare the difference between the NAFLD and control groups.
Quality assessment
The included studies were assessed by the Newcastle–Ottawa Scale (NOS). 11 The NOS is judged on three broad subscales using a star to identify high-quality choices: the study groups' selection, the groups' comparability, and the ascertainment of the exposure. The NOS score of ≤5 was regarded as low quality.
Statistical analysis
This meta-analysis was conducted using Comprehensive Meta-analysis Version.3 (Biostat, Englewood, NJ). We used the SMD for the effect size. SMDs and 95% confidence intervals (CIs) were calculated for all eligible studies included in the meta-analyses and combined using a random-effects model.
Statistical heterogeneity among trials was assessed using Cochran's Q and I 2 statistic, which estimates the percentage of total variation across studies due to heterogeneity rather than chance. We considered I 2 values of 25%–49%, 50%–74%, and 75% or greater to represent low, moderate, and high heterogeneity. We assessed the publication bias through funnel plots (plots of study results against precision) and with the Begg and Egger tests. 12,13 For the robustness of the summarized effect size, we conducted a sensitivity analysis by omitting each study in turn and recalculating the remaining ones.
Results
Literature search and study characteristics
We identified 304 studies in full publications or abstract forms using the methodology above and the search terms. Of the studies, 47 were reviews and short communications; 84 were book chapters, 25 were conference literature, 5 were animal studies, 3 were editorials, 93 were meetings and book indexes, and 38 had no relevant outcomes to the subject. Nine publications were retrieved for further evaluation. Of these, three were eliminated because they needed more data for calculation. Finally, six studies were included in the meta-analysis. The details of the literature search are depicted in Fig. 1.

Flow diagram for literature search.
The six selected studies 14 –19 included 7089 participants ranging from 132 to 3508. They were published between 2013 and 2020. All of these studies were designed as observational studies. Two of these studies were from Turkey, two from Italy, and two from South Korea. The detailed characteristics of the included studies are presented in Table 1.
Characteristics of the Studies Included in the Meta-Analysis
BOO, bladder outlet obstruction; BPH/LUTS, Benign prostate hyperplasia/lower urinary tract symptoms; FLI, fatty liver index; IPSS, international prostate symptom score; NAFLD, non-alcoholic fatty liver disease; NASH, non-alcoholic steatohepatitis; PSA, prostate specific antigen; PVR, postvoided residual urine volume; TURP, transurethral resection of the prostate.
Prostate size and NAFLD
The pooled analysis of six studies 14 –19 revealed that patients with NAFLD have larger prostate volume [0.553 (0.303–0.802), P ˂ 0.001; Q = 97.41; P-value for heterogeneity = P < 0.0001; I 2 = 94.86%]. Figure 2 depicted the details of the individual studies and pooled analysis, including the SMD and CI calculations.
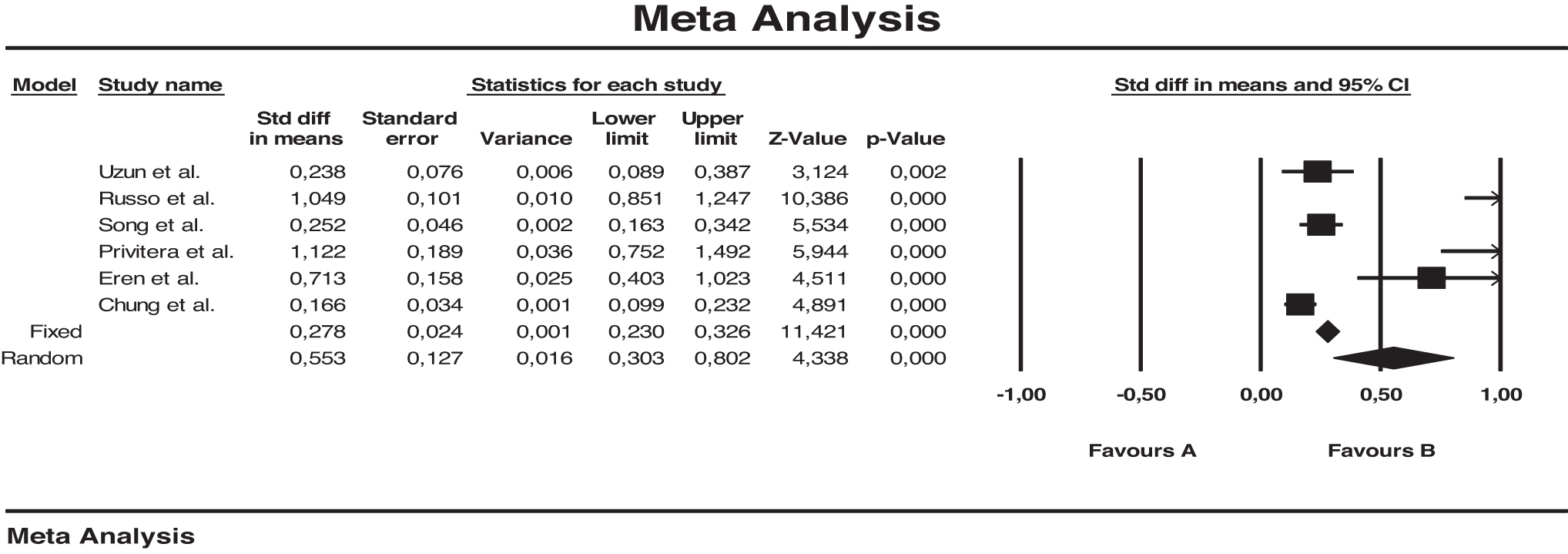
Meta-analysis plot for prostate volume among patients with and without NAFLD. NAFLD, non-alcoholic fatty liver disease.
IPSS and NAFLD
The pooled analysis of six studies 14 –19 demonstrated no significant difference in IPSS value among the patients with NAFLD and non-NAFLD [0.142 (−0.254 to 0.538), P = 0.25; Q = 251.52; P-value for heterogeneity = P < 0.0001; I 2 = 98.02%]. Figure 3 depicted the details of the individual studies and pooled analysis, including the SMD and CI calculations.
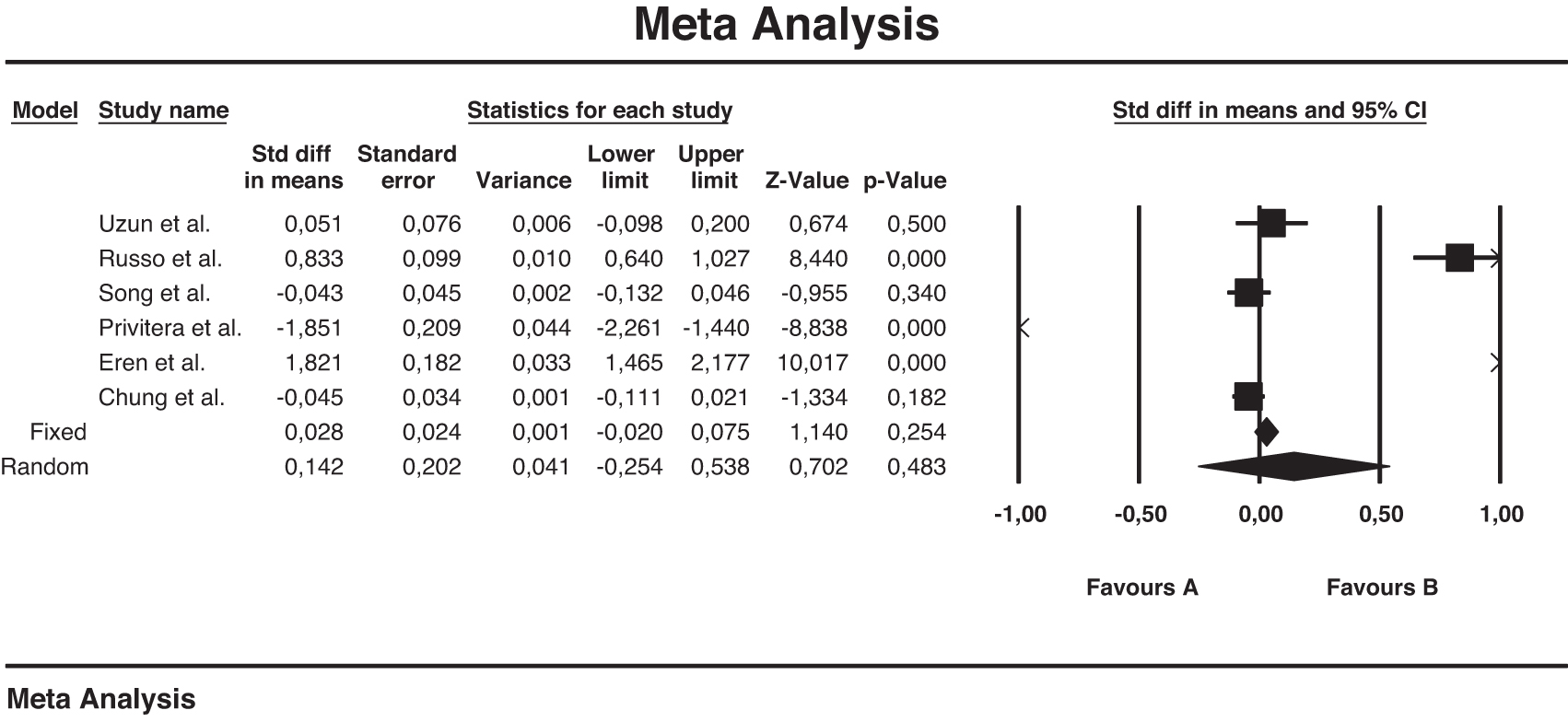
Meta-analysis plot for IPSS among patients with and without NAFLD. IPSS, international prostate symptom score.
PSA and NAFLD
The pooled analysis of six studies 14 –19 demonstrated no significant difference in PSA value among the patients with NAFLD and non-NAFLD [0.001 (−0.047 to 0.048), P = 0.97; Q = 97.41; P-value for heterogeneity P = 0.54; I 2 = 0.0%]. Figure 4 depicts the details of the individual studies and pooled analysis, including the SMD and CI calculations.

Meta-analysis plot for PSA value among patients with and without NAFLD. PSA, prostate-specific antigen.
Sensitivity analysis and publication bias
A sensitivity analysis for prostate volume was carried out. Each study was excluded in turn to recalculate the pooled SMD of the remaining studies. Omitting six studies was similar to the original pooled summary effect size. The sensitivity analysis for prostate volume is depicted in Table 2.
Sensitivity Analysis for the Prostate Volume After Each Study Was Excluded in Turn
CI, confidence interval; SMD, standard mean difference.
Similarly, a sensitivity analysis for the IPSS was performed. Omitting any of the six studies did not produce a significant difference in the original pooled summary effect size except for the study by Privitera et al. We conducted a second-step sensitivity analysis among the remaining five studies, omitting each and recalculating the remaining four studies (data not shown). The sensitivity analysis for the IPSS value is depicted in Table 3.
Sensitivity Analysis for the International Prostate Symptom Score Value After Each Study Was Excluded in Turn
We performed a Funnel plot test to analyze the publication bias. The shape of the funnel plot was asymmetric. This visual impression was confirmed by Begg and Mazumdar rank correlation test and Egger's regression tests which yielded a significant P-value (0.03 for both tests). Figure 5 illustrates the funnel plot of publication bias for the prostate volume.
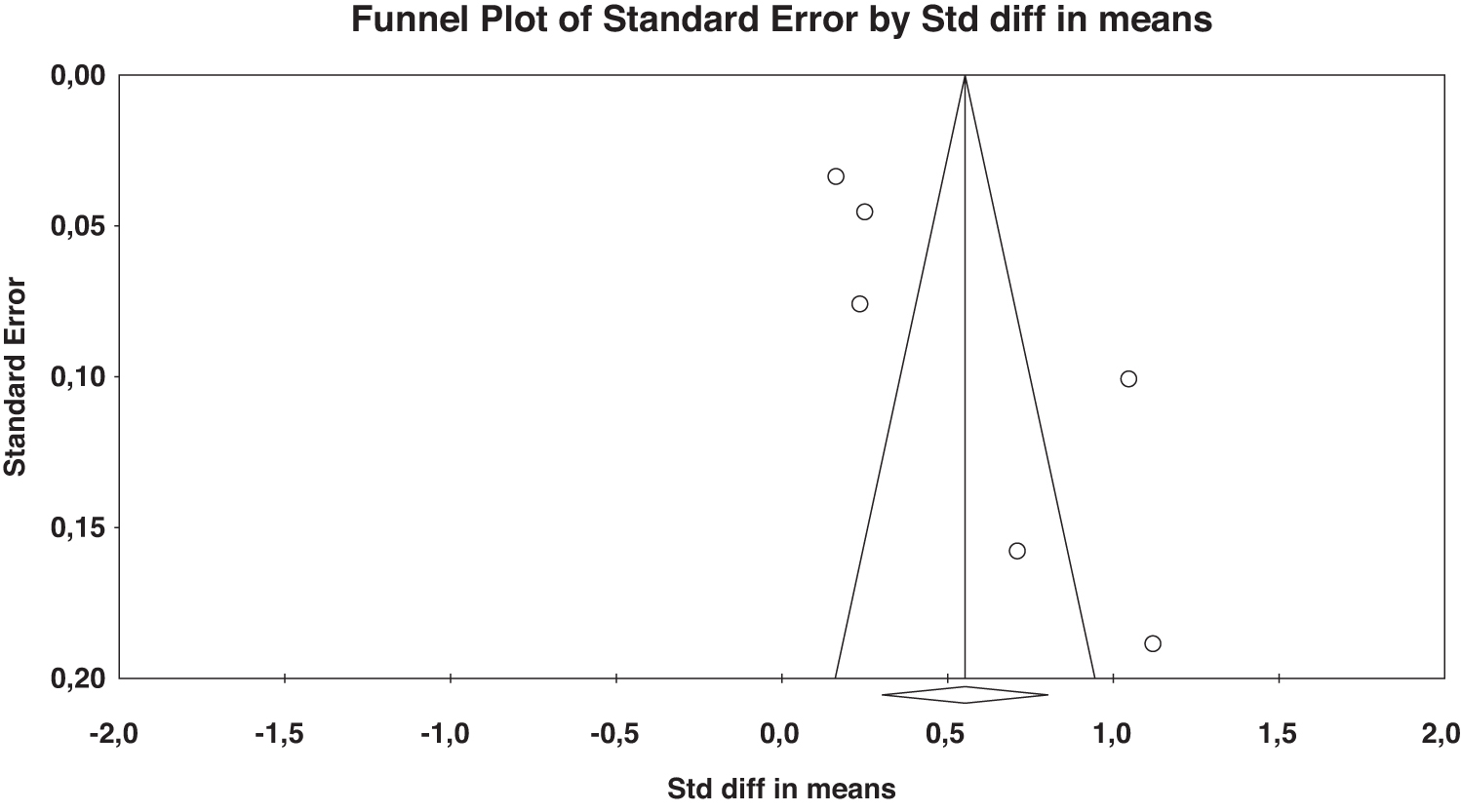
Funnel plot of publication bias for prostate volume.
Quality assessment
According to NOS assessment, the mean quality score of all studies was 8.3. The thorough evaluation of the study qualities is demonstrated in Table 4.
Newcastle–Ottawa Scale for Quality Assessment
Discussion
This is the first meta-analysis pooling the studies on the association between NAFLD and BPH/LUTS in a systematic review process. The literature included several reports about MetS and the BPH/LUTS association. 7,20 As a liver manifestation of MetS, NAFLD is an attractive issue that led the investigators to search for a possible link between these entities.
The hyperplastic process of BPH is still under debate despite intense research, which has been ongoing for many years. The androgens, particularly testosterone, are essential for prostate enlargement. However, the process is not easy to understand because serum testosterone level is not correlated with prostate volume. As testosterone levels decrease with aging, the prostate enlarges. Studies have shown that many growth factors are implicated in the pathogenesis of prostate enlargement. 21,22 Interactions between these growth factors and steroid hormones (estradiol, testosterone, dihydrotestosterone, and their ratios) might arrange the balance of cell proliferation versus cell death to produce prostate hyperplasia. 2,3
MetS is a constellation of various disorders, including obesity, impaired fasting glucose, hypertension, and dyslipidemia. Patients with Mets are generally overweight or obese. Adipose tissue is the primary source of aromatization of testosterone to estrogen. In addition, patients with obesity or MetS have low-grade chronic inflammation throughout the body. This inflammation led to the release of various growth factors. 6 Based on these pathophysiologic mechanisms, it is reasonable that patients with NAFLD have larger prostate volumes.
Previous meta-analyses have also found a positive correlation between prostate volume and MetS. 23,24 The summary of our pooled analysis demonstrated that patients with NAFLD have larger prostate volumes than non-NAFLD patients. However, this conclusion should be interpreted with caution. Although the summary effect size among studies was significant, the mean difference between the two groups was only 0.553 mL. At this point, we should consider that statistical significance (P-value) does not necessarily mean clinical significance. To uncover the clinical reflection of prostate enlargement with NAFLD, well-designed further studies with larger sample sizes are warranted.
The summary effect size of our meta-analysis presented a nonsignificant association between LUTS and NAFLD. However, when we excluded the study of Privitera et al. as a part of the sensitivity analysis, the recalculation of the remaining five studies' data yielded a significant result between IPSS and NAFLD. Perhaps, this is the side of our meta-analysis that should be interpreted most carefully. We conducted a second-step sensitivity analysis among the five studies. This calculation yielded inconclusive results, which did not produce a clear association between LUTS and NAFLD (data not shown).
The results of our cumulative analysis of six studies are consistent with previous meta-analyses on the association between MetS and LUTS. 24,25 Some cross-sectional studies even demonstrated that MetS has a favorable effect on LUTS. 26 –28 However, the data of these should be interpreted with caution. Because different patient populations with varying age ranges were included in the analysis of these studies, many confounding factors such as socioeconomic status, lifestyle, smoking, and ethnicity (these studies were from Asia) might also affect the results. Therefore, we cannot generalize these studies' findings to the whole population.
Large prostate is a strong indicator of LUTS, but all patients with increased prostate volume do not necessarily complain of the lower urinary tract. The findings of our meta-analysis might also be interpreted in this regard. In addition, we could not pool subdomain IPSSs (voiding and storage subscores) since more information was needed in the studies pooled for meta-analysis. We should also be aware that the studies included in this meta-analysis are observational. Patients with high NAFLD may have comparable symptom scores with non-NAFLD participants when they were analyzed, but they may develop LUTS when followed up appropriately. This might be an issue of well-designed longitudinal prospective studies.
Prostate-specific antigen is one of the most critical clinical elements for patients with prostatic diseases. Although we commonly use PSA in diagnosing and following up on patients with prostate cancer, it is not a disease-specific marker. It is also released in the presence of BPH and prostatic infections. According to some studies, there is an association between PSA and prostate volume. 29,30 Therefore, we also evaluated the pooled analysis of PSA in our meta-analysis. No significant association was found between NAFLD and the control group. This finding can be interpreted as the consequence of a significant but slight increase in prostate volume found in the NAFLD group. Therefore, that slight enhancement in prostate volume may not have been sufficient to increase the PSA level significantly.
The strengths and limitations of the meta-analysis
All studies included in our meta-analysis were evaluated rigorously regarding study quality, publication bias, and the confounding factors that lead to heterogeneity. Since this is a systematic review and meta-analysis, not a narrative review, we sought to be careful in gaining the data of the studies to reach a reliable conclusion. From this point of view, the present research can address some issues that a narrative review cannot. In addition, the quality of the studies included in the meta-analysis was relatively high according to a comprehensive assessment method of NOS. This might be a favorable factor for enhancing the quality of the meta-analysis.
Some limitations of this meta-analysis should be addressed. First, the limited number of studies may diminish the meta-analysis's power. Second, significant heterogeneity was detected in the association of prostate volume between NAFLD and non-NAFLD patients. Different evaluation criteria of NAFLD, a substantial difference between the number of participants in each study which ranges from 132 to 3508, and different population characteristics included in each study might be the sources of heterogeneity. Third, publication bias was available for the prostate volume analysis. Finally, this meta-analysis included observational studies, not longitudinal studies. Hence we cannot provide a direct causal relationship among the entities examined.
Consequently, the present meta-analysis demonstrated that patients with NAFLD have larger prostate sizes than non-NAFLD participants. However, no significant association was found for LUTS. This meta-analysis should be considered an intermediate station, not a final stop for searching BPH/LUTS and NAFLD association. From this point of view, the results drawn from our meta-analysis may shed light on well-designed—if possible—longitudinal studies to determine the relationship between BPH symptoms and NAFLD.
Footnotes
Authors' Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by H.B. and M.K. The first draft of the article was written by H.B., and all authors commented on previous versions of the article. All authors read and approved the final article.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary File S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.