
Abstract
A thorough examination of the available literature has revealed a well-established association of obesity and high body mass index (BMI) with an increased risk of various types of cancers, including hematologic malignancies. Specifically, the studies reviewed indicate a clear correlation between obesity and an increased risk of leukemias, lymphomas, multiple myeloma, myelodysplastic syndrome, and myeloproliferative diseases. Despite the established association of obesity and high BMI with hematologic malignancies, the underlying mechanisms remain largely undetermined. The development of hematologic malignancies may be influenced by several mechanisms associated with obesity and high BMI, including chronic inflammation, hormonal imbalances, adiposopathies, and metabolic dysregulation. Furthermore, there is mounting evidence indicating that obesity and high BMI may have a negative impact on the response to treatment and overall survival in patients with hematologic malignancies. This article aims to increase awareness and summarize the current state of research on the impact of obesity on hematologic malignancies, including the mechanisms by which obesity may influence the development and progression of these diseases. In addition, the current review highlights the need for effective weight management strategies in patients with hematologic malignancies to improve outcomes and mitigate the risk of complications.
Introduction
Obesity and high body mass index (BMI) have become major public health issues worldwide, with increasing prevalence and significant impact on morbidity and mortality. 1,2 Obesity is associated with a range of chronic diseases, including cardiovascular disease, type 2 diabetes, nonalcoholic fatty liver disease, and certain types of cancers (Fig. 1.). 2 –5 The modifiability of obesity as a risk factor for cancer makes it a unique target for both the prevention and treatment of cancers. 6
Different diseases and clinical conditions associated with obesity.
The relationship between obesity and cancer has received attention, with evidence suggesting that obesity is associated with an increased risk of cancer incidence and mortality. 7 However, the impact of obesity on hematologic malignancies, including leukemias, lymphomas, multiple myeloma (MM), myelodysplastic syndrome (MDS), and myeloproliferative diseases, remains poorly understood despite the rising global burden of these diseases. 8 Hematologic malignancies represent a significant and growing global burden of cancer, and there is concern about the potential impact of modifiable risk factors, such as obesity, on cancer incidences and outcomes. The mechanisms by which obesity may increase the risk of hematologic malignancies are incompletely elucidated, but chronic inflammation, dysregulation of adipokine secretion, hormonal imbalances, and metabolic dysfunction have been proposed. 9 –11
In addition, studies have shown that obesity and high BMI may negatively impact the response to treatment and increase the likelihood of complications during treatment in patients diagnosed with hematologic malignancies. 12 Due to the lack of attention given to the relationship between obesity and hematologic malignancies, a literature review investigating this relationship is necessary to fill this knowledge gap, and to inform future research and public health interventions.
There is a need for original studies that show the relationship between obesity, high BMI, and hematologic cancers, and that weight loss can have positive results in treatment. This article aims to increase awareness and summarize the current state of research on the impact of obesity on hematologic malignancies, including the mechanisms by which obesity may influence the development and progression of these diseases. This review will also cover the possible positive outcomes of weight reduction in patients who are classified as either obese or overweight and diagnosed with hematologic cancers.
Epidemiology of Obesity and Interaction with Cancer
Obesity is a chronic and complex disease resulting from an imbalance between caloric intake and energy expenditure, leading to excessive adipose tissue accumulation. 13 Over time, this imbalance leads to a buildup of excess body fat. 13 In the scientific literature, body composition is often assessed using the BMI. World Health Organization (WHO) currently defines overweight as having a BMI between 25 and 29.9 kg/m2, and obesity as having a BMI of ≥30 kg/m2. 14
According to the WHO reports in 2016, a significant proportion of the adult population, comprising individuals aged ≥18 years, was classified as overweight, with a substantial number being deemed obese. Specifically, the data revealed that >1.9 billion adults were categorized as overweight, with 650 million individuals fitting the criteria for obesity. In addition, it was found that 39% of adults aged ≥18 years were classified as overweight, while 13% fell under the category of obesity. 14 The current understanding of the function of adipose tissue has evolved from viewing it solely as a means of energy storage to recognizing its role in endocrine and metabolic processes.
Several mechanisms have been identified that contribute to the relationship between obesity and the incidence and mortality of cancer. 15 Obesity contributes to several mechanisms that promote the development and progression of cancer, including glucose and lipid metabolism disturbances, chronic inflammation, oxidative stress, and a higher risk of comorbidities such as diabetes, dyslipidemia, and cardiovascular disease. 15 –18 Obesity is associated with disturbances in lipid and glucose metabolism, chronic inflammation, and oxidative stress, in addition to an elevated risk of various comorbidities such as diabetes, dyslipidemia, and particularly cardiovascular disease. 16 –18
The underlying mechanisms that contribute to the development of these comorbid conditions are also thought to play a role in the emergence of cancer. 11 Obesity is a well-established risk factor for several types of cancers, including colorectal, endometrial, esophageal, kidney, and pancreatic cancers, as well as postmenopausal breast cancer. 11,19 –21 Less common malignancies associated with obesity are malignant melanoma, thyroid cancers, leukemia, non-Hodgkin lymphoma (NHL), and MM. 22
Studies conducted by the American Cancer Society indicate that excessive body weight may account for a significant proportion of cancer cases, specifically 11% in females and 5% in males in the United States, as well as 7% of cancer-associated mortality. A study conducted in 2019 reveals that globally, in 2012, excess body weight was identified as a contributing factor in 3.9% of all cancer cases, equating to a total of 544,300 cases. The research further indicates that the burden of these cancer cases was disproportionately higher among women, with 368,500 cases, as compared with men with 175,800 cases. 7 However, it is worth noting that the exact percentage of cancer cases that are directly related to obesity can vary depending on the type of cancer and the population being studied.
The correlation between obesity and cancer susceptibility is multifaceted, and can be impacted by a plethora of factors, including genetic predisposition, infections, and behavioral patterns such as tobacco use. 23 Furthermore, ongoing research endeavors aim to enhance our comprehension of the underlying mechanisms that mediate the association between obesity and cancer, and formulate efficacious interventions for reducing cancer risk in individuals with obesity. Adhering to a healthy lifestyle regimen comprising regular physical activity, a nutritious diet, and maintenance of a healthy BMI may lower cancer incidence. 6
Obesity-Related Hematologic Malignancies and Outcomes
Studies have revealed that individuals who are obese or overweight have a heightened susceptibility to multiple subtypes of hematologic malignancies. 12,24,25 Obesity is associated with all types of leukemias. 26 –28 A study has found a positive correlation between obesity incidence and mortality among adults with leukemia but not in overweight patients. 29 Numerous studies have demonstrated a statistically significant association between obesity and an increased risk of acute myeloid leukemia (AML) in adults independent of other demographic factors such as age, sex, performance status, race, and ethnicity.
In particular, studies have demonstrated a negative impact of obesity on the survival outcomes of patients with acute promyelocytic leukemia (APL), and a significantly increased risk of relapse and differentiation syndrome after all-trans-retinoic acid/idarubicin treatment. 30,31 On the contrary, some studies have indicated that there is no correlation between obesity and the risk of AML in several studies. 31 –33 According to a study by Wong et al., obesity may even have a protective effect against AML. 34
A study has demonstrated that individuals diagnosed with acute lymphoblastic leukemia (ALL) and classified as obese have poorer survival outcomes in comparison with their nonobese counterparts. Within the subset of patients diagnosed with T-ALL, obesity was found to be correlated with a fivefold increase in overall mortality. 10 Another study has revealed that obesity is associated with a poorer response to treatment and elevated levels of minimal residual disease among patients diagnosed with B-ALL. 35 In addition, a meta-analysis of four studies that reported results by subtypes of leukemia revealed that obesity is associated with a statistically significantly increased risk of all subtypes of leukemias. 29
The GBD study of 2019 identified several risk factors for chronic lymphocytic leukemia (CLL), including high BMI. 7 In addition, an analysis suggests that obesity is associated with shorter progression-free survival and overall survival (OS) in female CLL patients treated with fludarabine, cyclophosphamide, and rituximab therapy. 36 Obesity has also been linked to an increased risk of NHL in adults. 37 A meta-analysis of published studies provides evidence of a statistically significant positive correlation between BMI and the risk of NHL.
The analysis indicates that overweight individuals had a 7% greater risk, and obese individuals had a 20% greater risk of NHL when compared with individuals with a normal weight. 38 Studies have suggested that this association may be strongest for certain subtypes of NHL, such as diffuse large B-cell lymphoma (DLBCL). 39 A meta-analysis of published studies suggests that BMI and weight in early adulthood may have a stronger association with the development of NHL than current BMI and weight. 40
In another study, NHL, DLBCL, and MM have been associated with increased BMI in childhood. These findings underscore the importance of maintaining a healthy weight throughout the life course, particularly in early life, as a potential strategy to prevent hematologic malignancies. 41 In contrast, several studies have reported a positive correlation between increased BMI and improved survival outcomes in patients with various subtypes of lymphoma, including HL, intermediate-grade B-cell NHL, DLBCL, and extranodal natural killer/T cell lymphoma, nasal type. 42 –46
The correlation between obesity and the progression of HL remains a topic of debate in the field. However, a study by Landgren et al. found that BMI was independently and significantly linked to cause-specific survival in HL patients. The study also reported the following 5-year OS rates for the different BMI groups: 100% for the obese group, 79% for the overweight group, and 70% for the normal and underweight groups. They found that among patients with HL treated with chemotherapy, a high BMI was significantly correlated with a favorable prognostic risk profile and an improvement in cause-specific survival. 42 These findings suggest that obesity may positively impact the outcome of HL treatment.
Another study conducted by Willett and Roman found that a high BMI increased the risk of HL more than twofold compared with those in the normal BMI range. 47 In contrast to the previously mentioned study, these results indicate that obesity may have a potential effect on the course of HL, thus further research is essential to comprehend the underlying mechanisms and potential implications for the treatment and management of HL patients with obesity. 47,48
Obesity has also been linked to an increased risk of MM in adults. 49 –51 A study published in 2011 found that a 5 kg/m2 increase in BMI was associated with a 12% and 21% increased risk of MM incidence and mortality, respectively. The risk ratio did not differ significantly between men and women. 49 In addition to the previously mentioned study, a pooled analysis in the International Multiple Myeloma Consortium has reported an increased risk of 11% per 5 kg/m2 increase in BMI for MM. 52
The likelihood of monoclonal gammopathy of unknown significance (MGUS) progressing to MM appears to be significantly influenced by the presence of overweight and obesity. Studies have shown a correlation between increased BMI and an increased risk of progression from MGUS to MM. 53,54 In addition, in a study, the authors screened 1996 black and white women for MGUS, and found that obese individuals were 1.8 times more likely to develop MGUS than those with a normal BMI. 42
Obesity has also been linked to an increased risk of MDSs in adults. 55,56 A new study demonstrated a negative association between obesity and OS outcomes in individuals <65 years of age diagnosed with MDS and with lower risk MDS. 57 This study has also shown that there was a statistically significant difference in the rate of AML transformation between individuals with a BMI of ≥30 and those with a BMI <30. Specifically, the rate of AML transformation was 36% for patients with a BMI of ≥30 compared with 32% for those with a BMI <30 (p: 0.009). No significant difference was observed in response to azacitidine therapy.
A study has reported that obesity 2 years before diagnosis was associated with an increased risk of AML in both males and females. However, the association between obesity and MDS was observed only in females. In addition, the study found that weight change in adulthood was not consistently associated with either AML or MDS outcomes. 55 On the contrary, in a study of 419 MDS patients, being overweight and obese was associated with a favorable survival factor. 58 In addition, despite the limited number of studies conducted, there is evidence suggesting a correlation between obesity and myeloproliferative disorders, specifically regarding chronic myeloid leukemia and essential thrombocytosis. 59 –63
Underlying Mechanisms Mediating Obesity-Related Hematologic Malignancies
As previously discussed, studies have demonstrated a possible association between increased BMI and an increased risk of developing hematologic malignancies, such as leukemias, lymphomas, and myeloma. However, the underlying mechanisms by which obesity may increase the risk of hematologic malignancies are not fully understood; however, several potential mechanisms have been proposed as depicted in Fig. 2. A potential mechanism is the chronic low-grade inflammation that is often associated with obesity.
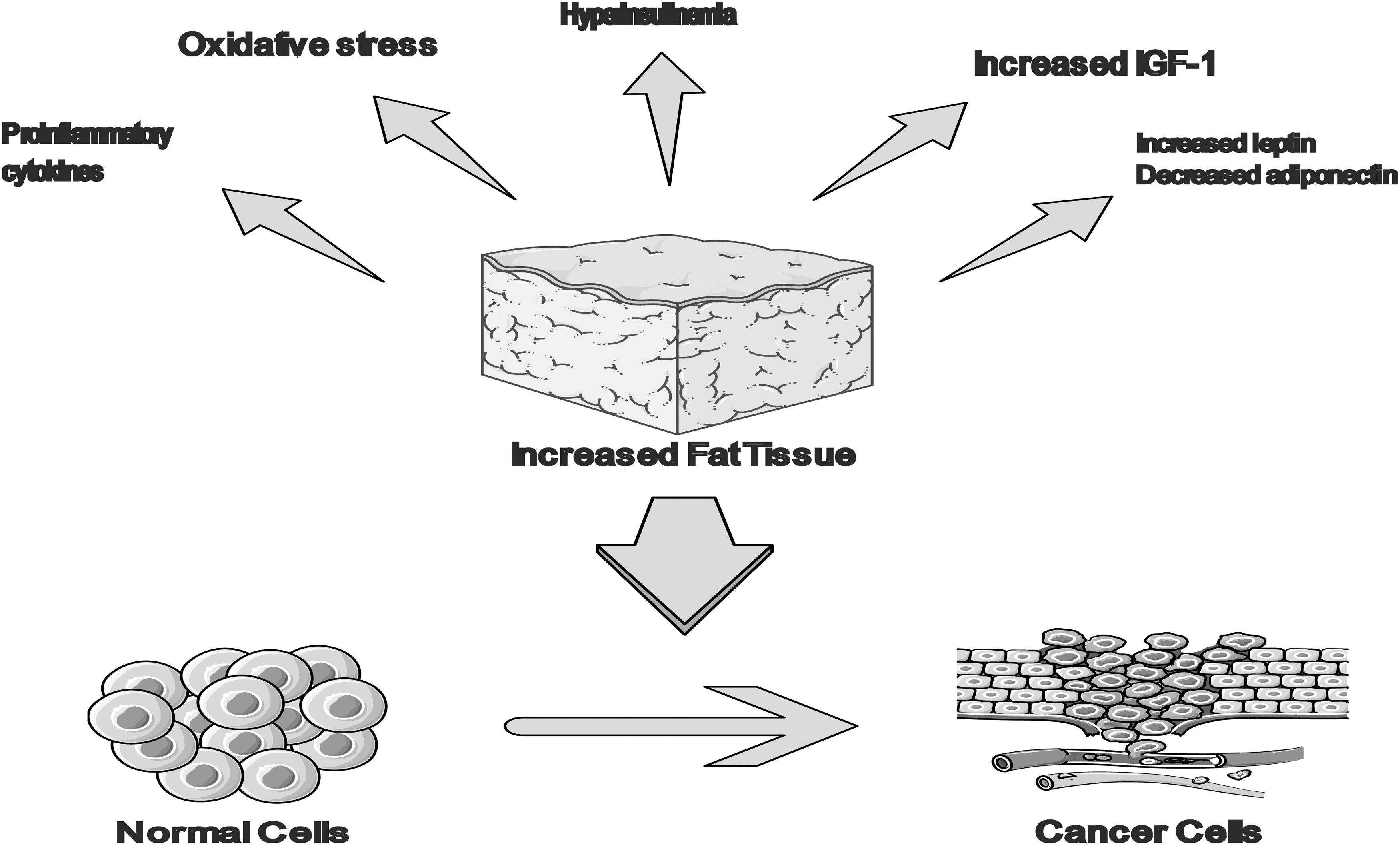
Underlying mechanisms mediating obesity-related hematologic malignancies. IGF-1, insulin-like growth factor 1.
Proinflammatory cytokines, such as interleukin-6 (IL-6), IL-1β, and tumor necrosis factor (TNF-α), which are released by adipocytes, may contribute to this chronic inflammation. These cytokines may also increase the production of C-reactive protein and serum amyloid A, which may further contribute to carcinogenesis. 64 Furthermore, TNF-α and IL-6 are overexpressed in the bone marrow of patients with myeloid malignancies, which have been associated with poor prognosis. 65 IL-6 levels have been correlated with prognosis in DLBCL. 66 It is well established that obesity is a risk factor for the development of insulin resistance and diabetes, and recent studies have also shown a correlation between diabetes and an increased risk of hematologic malignancies. 67
Other mechanisms that have been established to contribute to the increased risk of malignancy in diabetes include hyperinsulinemia, overproduction of insulin-like growth factor (IGF), and upregulation of the IGF-1 receptor. 68 One study conducted in vitro has revealed that the presence of IGF-I in lymphocytes can activate multiple signaling pathways, resulting in prolonged and excessive production of cytokines and inflammation. 69 Diabetes is also associated with several immune-related complications including immunosuppression, chronic inflammation, and lymphocyte dysfunction that can contribute to the development of hematologic malignancies. 70
Obesity is associated with increased levels of estrogen as adipose tissue, particularly in postmenopausal women, is an important source of aromatase, an enzyme that converts androgens to estrogens, and this hormonal change also increases the risk of certain types of hematologic malignancies. 37 Moreover, obesity is associated with increased levels of certain hormones called adipokines, which can promote cancer growth and metastasis. Adipokines are a group of hormones secreted by adipose tissue, and they can have proinflammatory and antiapoptotic properties, which can promote cancer growth and spread. 64
A plethora of research has investigated the correlation between serum leptin levels and the expression of leptin receptors in blast cells of both myeloid and lymphoid malignancies. The literature has also documented the impact of leptin and its receptors on hematologic malignancies and the underlying mechanisms involved. 71 In contrast, it has been established that adiponectin levels are inversely correlated with BMI. Adiponectin is considered to be a protective hormone, due to its demonstrated anti-inflammatory, insulin-sensitizing, antiatherogenic, cardioprotective, and antineoplastic properties. 25
It is noteworthy that numerous adipokines, which are overexpressed by adipose tissue in obese individuals, possess potent proangiogenic properties. This suggests the possibility that these adipokines may mediate the causal link between excessive adiposity and hematologic malignancies, by modulating the process of angiogenesis. 72 In summary, various mechanisms have been proposed to explain the association between obesity and BMI with an increased risk of hematologic malignancy. Further research is needed to gain a more comprehensive understanding of these mechanisms, which may have implications for the prevention and treatment of these diseases in the future.
Management of Obesity and Overweight in Patients with Hematologic Malignancies
The management of obesity and overweight among patients with hematologic malignancies is a crucial component of cancer care. As previously stated, obesity is a risk factor for the development of hematologic malignancies, and may also negatively impact the response to treatment and increase the likelihood of complications during treatment. 9,12,30,31 As such, health care professionals must address weight management in these patients.
The initial step in managing obesity and overweight among patients with hematologic malignancies is to assess the patient's weight status, which can be accomplished through the measurement of BMI and other anthropometric measurements such as waist circumference. Upon determination of an individual patient's weight status, it is essential to develop a customized plan for managing their weight. Such a plan can be tailored to the specific needs and circumstances of the patient, and can facilitate the achievement of their weight management goals. The primary objective of weight management in patients with hematologic malignancies is the attainment and maintenance of a healthy weight. This can be achieved through a combination of a healthy diet and regular physical activity.
A healthy diet should consist of a variety of nutrient-dense foods, such as fruits and vegetables, whole grains, lean proteins, and healthy fats, and should limit the consumption of processed foods, added sugars, and saturated fats. Regular physical activity is also a vital aspect of weight management in patients with hematologic malignancies, as it can enhance cardiovascular fitness, alleviate fatigue, and improve the overall quality of life. 73 Other studies report a significant enhancement in individual physical capabilities, a decrease in feelings of fatigue and depression, and an improvement in overall quality of life. 59,74
According to a study, individuals with DLBCL who engaged in the highest levels of physical activity had a 41% reduced risk of mortality during the follow-up period compared with those with the lowest activity levels. 48 This study also highlighted the importance of prediagnosis physical activity. However, it is important to bear in mind that cancer treatment can lead to fatigue and other side effects, thus it is essential to work with a health care professional to develop an exercise plan that is safe and appropriate for the patient.
In addition to diet and exercise, other strategies can be employed to manage weight in patients with hematologic malignancies, including behavioral therapy, which can aid patients in developing the skills and strategies necessary to maintain a healthy weight, and medications, such as weight-loss drugs and appetite suppressants. Specifically, weight-neutral or weight-loss–promoting interventions, such as metformin, GLP-1 agonists, or sodium-glucose cotransporter 2 inhibitors, which are frequently used to treat insulin resistance and type 2 diabetes, may be beneficial in improving the health and outcomes in cancer survivors. 75
Bariatric surgery can be a viable option for obese individuals with hematologic malignancy, but there is a very limited acknowledgment of this, a study has reported a reduction in the occurrence of NHL among females with obesity who have undergone bariatric surgery. 76 This suggests that weight-loss surgery may have a protective effect against the development of NHL in obese individuals. However, it should be noted that this observation is based on a single study, and more research is needed to confirm the findings and establish the underlying mechanisms.
In addition, it is important to keep in mind that bariatric surgery is a major procedure and should only be considered after all other weight-loss options have been exhausted, and it is deemed medically necessary by a doctor. But it should be approached with caution and under the guidance of a multidisciplinary team of specialists, it is recommended that patients with hematologic malignancy should have their cancer treated, and their disease should be in remission before bariatric surgery.
Also, they should have a good performance status and a low risk of recurrence. It is important to note that weight management in patients with hematologic malignancies necessitates a multidisciplinary approach that involves the patient's hematologist, oncologist, dietitian, and other health care professionals. In conclusion, managing obesity and overweight among patients with hematologic malignancies is a crucial aspect of cancer care. A combination of a healthy diet, regular physical activity, and other strategies, such as behavioral therapy and medications, can assist in achieving and maintaining a healthy weight. Regular follow-up and monitoring are also essential to ensure the effectiveness of the patient's weight management plan and to make any necessary adjustments.
Discussion
The literature reviewed in this study provides a comprehensive examination of the relationship between obesity and BMI and hematologic malignancies. BMI is widely utilized as a metric for determining obesity. The use of BMI to measure obesity may lead to the misclassification of individuals who are metabolically unhealthy as not being obese. Waist circumference may be a more accurate measure of obesity, as it has a stronger correlation with visceral adiposity.
Overall, the studies examined in this review suggest to an association between obesity and hematologic malignancies, although some subtypes, such as APL, MM, and DLBCL, seem to show a stronger association. 31,47,50 However, the evidence for Hodgkin's lymphoma is not as clear, 42,47 and numerous studies have not found any correlation between obesity and AML. 31 –33 Some of these studies have indicated that obesity may have a protective effect against hematologic malignancies. 34 As mentioned earlier, the pathogenic mechanisms by which adiposopathies contribute to the development of hematologic malignancies remain elusive.
Several pathways have been postulated, and a deeper comprehension of these mechanisms could have implications for the prevention and treatment of hematologic cancers in the future. The observed association between obesity and hematologic malignancies underscores the importance of implementing weight management interventions into clinical practice.
Weight-loss interventions, such as bariatric surgery, weight-loss drugs, and lifestyle modifications, may confer substantial benefits in cancer prevention and management by reducing the risk of malignancy in obese individuals, and enhancing the outcomes of cancer survivors. However, the current data on this topic are scarce and limited. Hence, additional research is needed to establish the most efficacious weight-loss strategies for cancer prevention and management across diverse patient cohorts.
The studies included in the review indicate a clear association between obesity and an increased risk of hematologic malignancies. 7,12,30,52,57,60,61 While a significant body of research has established a correlation between obesity and the development of hematologic cancers, it is important to note that the data generated from these studies may not conclusively prove a causal relationship. Other factors such as dietary habits, lifestyle choices, or genetic and environmental factors such as Epstein-Barr virus infection may also contribute to the development of obesity and hematologic cancers. Therefore, further research is needed to establish a definitive causal link and to fully understand the underlying mechanisms involved.
One limitation of the studies reviewed is that most of them are observational in nature and as such, they do not establish a causal relationship between obesity and hematologic malignancies. In addition, the studies reviewed have different methodologies and patient populations, which may limit the generalizability of the findings. In conclusion, the literature reviewed in this study demonstrates a significant association between obesity and hematologic malignancies, highlighting the need for further research and effective interventions for the management of obesity to improve outcomes.
Conclusion
Obesity and high BMI have been linked to an increased risk of developing hematologic malignancies, such as HL, NHL, leukemia, and MM. Studies have shown that obese individuals have a higher risk of developing these diseases, and that obesity can also negatively impact the prognosis for individuals who are already diagnosed with these malignancies. The exact mechanism by which obesity increases the risk of hematologic malignancy is not well understood; further studies are needed, but it is thought to be related to chronic inflammation, hormonal imbalances, and metabolic dysfunction caused by excess body fat.
It is important for individuals who are obese or have a high BMI to be aware of the increased risk of hematologic malignancy and to discuss their risk with their health care provider. It is important to point out that, as with any medical condition, the impact of obesity on hematologic malignancies can be affected by many factors, such as genetics, the age of the patient, exposure to certain chemicals and radiation, and the presence of other comorbidities. Therefore, a health care professional would be the best suited to evaluate the specific impact of obesity on patients with hematologic malignancies.
It has been previously emphasized that the management of body composition is crucial in patients. This information can be used to develop targeted prevention and intervention strategies. For example, weight-loss interventions, such as lifestyle changes, bariatric surgery, and pharmacotherapy, may reduce the risk of hematologic malignancies and improve the outcomes among obese individuals. In addition, regular monitoring and screenings for hematologic malignancies may be beneficial for individuals who are obese or have a high BMI.
Footnotes
Authors' Contributions
R.Ç. contributed to developing surgical and medical practices, concept, and design. M.T.B. assisted with literature search and writing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.