
Abstract
Aim:
Type 2 diabetes mellitus (T2D) patients have an increased risk for cardiovascular disease (CVD). Different algorithms are used for the CVD risk quantification and United Kingdom Prospective Diabetes Study (UKPDS) score was among the most validated. Endocan is a novel endothelial dysfunction marker. The aim was to explore the potential relationship between serum endocan level and UKPDS risk engine score [which enables calculation of the 10-year risk of nonfatal and fatal coronary heart disease (eCHD) and stroke] in T2D patients.
Materials and Methods:
The study included a cohort of 104 patients with T2D (of them 52.8% men), with median age 66 years and body mass index (BMI) = 30.7 kg/m2. Patients were divided into: low (<15%), moderate (≥15% and <30%), and high-risk UKPDS category (≥30%).
Results:
In multivariable regression analysis (when adjusted for sex, BMI and/or hip circumference), endocan was the independent predictor for moderate and high estimated risks (nonfatal eCHD, fatal eCHD, and nonfatal stroke risk). In the Model for high nonfatal eCHD [areas under curve (AUC) = 0.895] and high fatal eCHD (AUC = 0.860) endocan indicated good clinical accuracy, and an excellent accuracy in discriminating patients with high risk for nonfatal stroke risk (AUC = 0.945).
Conclusion:
Endocan was the independent predictor for moderate and high estimated risks (i.e., nonfatal and fatal CHD and nonfatal stroke risk scores) in T2D patients. When included in models with sex and obesity indices endocan demonstrated good clinical accuracy in discriminating T2D patients with high risk for nonfatal and fatal eCHD and nonfatal stroke risk from those patients with low risk.
Introduction
It is well-established that patients with type 2 diabetes mellitus (T2D) have an increased risk for cardiovascular disease (CVD). 1 The timely manner recognition of high CVD risk burden can enable adequate therapeutic strategy and improve the quality of life in these patients. 2
Despite the fact that lot of effort was put into the research of the best quality assessment of CVD risk in T2D patients, there is still a knowledge gap regarding this health concern. 3 Namely, different algorithms are used for the quantification of the CVD risk. 4 –11 Among them, United Kingdom Prospective Diabetes Study (UKPDS) score 4 –7 and Framingham risk score (FRS) 8 –10 were the most validated. UKPDS model was specifically designed for the T2D patients, whereas FRS consisted of only 6% of T2D. Therefore, it is assumed that Framingham risk score may underestimate CVD risk in T2D patients. 11 In comparison with Framingham risk score, the UKPDS risk engine was found to better predict CVD in T2D individuals. 8 –10
On the contrary, although both algorithms demonstrated the capability to identify patients with high CVD risk, a poor agreement between predicted and observed CVD risk was also reported. 3 Hence, it was thought that the predictive ability of these algorithms might be improved with the addition of some particular endothelial biomarkers. 12 –14
Endocan is a recently discovered biomarker that might be a novel indicator of endothelial dysfunction. 15 It is dermatan sulfate (DS) proteoglycan (PG) much smaller (∼50 kDa) than other PGs. Unlike other PGs that are connected with the extracellular matrix or cell membranes, endocan is a soluble PG secreted by endothelium, but its expression is recorded not only in endothelial cells, but also in distant, highly proliferative tissues (i.e., hepatocytes, lungs, cardiomyocytes, and so on). Proinflammatory cytokines such as interleukin-1 and tumor necrosis factor-alpha enhance secretion of endocan. On the contrary, endocan stimulates cellular adhesion molecules expression and its higher levels were recorded even in the early phase of atherosclerosis. 15 It is unclear how endocan is catabolized, but neutrophil proteases are regarded as the main culprits for its degradation. 15
Several studies 16 –19 demonstrated its higher serum levels in the cardiometabolic disorders that are tightly connected with insulin resistance (IR). Impaired signaling pathways of insulin (i.e., IR), inflammation, and endothelial dysfunction are pathophysiological mechanisms that contribute to atherosclerosis, the key manifestation of CVD. 20 The relationship of endocan with inflammation markers 15,21 and carotid intima-media thickness imply its role in atherogenesis onset, 22,23 whereas the decrease in serum endocan level could diminish the activation of the endothelial cells and delay the atherosclerosis progression. 24
Since we previously reported higher endocan levels in patients with T2D compared to diabetes-free individuals, 21,25 we hypothesized that this biomarker might be related to CVD risk and that it might add significant contribution to the CVD risk stratification. If this was a case, CVD risk score might be improved and high CVD risk T2D patients might benefit through better recognition and timely medical treatment. Hence, the aim of this research was to explore the potential relationship between serum endocan level and UKPDS risk engine score in a cohort of patients with T2D.
Materials and Methods
Study population
The study included a cohort of 104 patients with T2D (of them 52.8% men). The patients were recruited consecutively, during their regular laboratory check-up in the Primary Health Care Center in the capital of Montenegro. The study was conducted in a period from May to July 2017, after receiving the approval of the Institutional Review Board for the study design, following the Declaration of Helsinki principles and after all participants had signed the consent that were informed about the research protocol.
The majority of patients reported previously diagnosed T2D. In addition, following the criteria of the American Diabetes Association Standards of Diabetes Care, 26 patients were diagnosed T2D if displayed two fasting glucose levels ≥7.0 mmol/L, or with a randomly measured glucose level of ≥11.1 mmol/L or if had glycated hemoglobin (HbA1c) level ≥6.5% on two different measurements. There were no participants who underwent oral glucose tolerance test.
After answering the questions related to somatic illnesses, lifestyle habits (e.g., medications use, alcohol consumption, cigarette smoking, T2D duration, atrial fibrillation, and other diseases) and demographic data, the patients underwent anthropometric measurements [i.e., body height (cm), weight (kg), hip circumference (HC; cm), waist circumference (WC; cm), and body mass index (BMI; kg/m2)].
Patients were excluded from the research if reported CVD or stroke, with malignant diseases, autoimmune diseases, kidney disease other than diabetic nephropathy, liver disease other than steatosis, pregnancy, high-sensitivity C-reactive protein (hsCRP) >10 mg/L, and ethanol consumption >20 grams/day, if used of anti-inflammatory drugs in the last month.
Biochemical analyses
The blood samples were collected after an overnight fast of at least 8 hr. One sample was collected in tube with serum separator and clot activator, and the other in tube with K2 ethylenediamine tetraacetic acid (EDTA), from each patient. Serum separator samples were left to clot for half an hour, and then were centrifuged according to the instructions of the manufacturer. Thereafter, sera samples were aliquoted and one aliquot was used for the measurement of lipid status [i.e., total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C)] and fasting glucose on Roche Cobas c501 chemistry analyzer (Roche Diagnostics GmbH, Mannheim, Germany). The other aliquot was kept freezed at −80°C for the measurement of endocan and hsCRP.
Whole blood samples collected in tubes with K2 EDTA were used for the measurement of HbA1c levels by the immunoturbidimetric method on the same analyzer as for the glucose and lipid parameters.
Endocan concentrations were obtained with an enzyme-linked immunosorbent commercial assay (ab213776; Human ESM1 ELISA Kit, Abcam, Cambridge, United Kingdom), whereas hsCRP levels were measured by nephelometric assay (Behring Nephelometer Analyzer, Marburg, Germany).
Estimated CVD risk score was determined with UKPDS risk engine (version 2.0) 6,7 which enables the calculation of the 10-year risk of nonfatal and fatal coronary heart disease (eCHD) and stroke. Variables that were included in the UKPDS risk engine calculation were ethnicity, sex, age, HbA1c, T2D duration, systolic blood pressure (SBP), TC, HDL-c, smoking status, and the presence of atrial fibrillation. All patients were divided into three categories: low risk (<15%), moderate risk (≥15% and <30%), and high risk (≥30%). 6,7
Statistical analysis
The statistical analyses were performed on an IBM SPSS 24.0 for Windows platform (SPSS Corp., Chicago, IL, USA). Kolmogorov–Smirnov test was used for testing data distribution. Data with normal distribution were given as mean ± standard deviation. Medians and interquartile ranges (IQR) were used for presenting skewed distributed data and were compared by Kruskal–Wallis (three groups' comparisons) and Mann–Whitney (two groups' comparisons) tests. Categorical data were given as absolute and relative frequencies. Correlation analysis was performed with nonparametric methods. Spearman's correlation analysis and data from these analyses were given as Rho (ρ) values. Associations between endocan and moderate and high estimated risk were tested by univariable and multivariable binary logistic regression analysis. Dependent variables moderate or high risks were coded as 1 and compared to low risk coded as 0.
Obtained data after these analyses were given as coefficient β [Standard Error (SE)] and odds ratio (OR) and 95% confidence interval (CI). The explained variation in estimated risks was presented by Nagelkerke R2. Receiver Operating Characteristic (ROC) curve analysis was performed to test the diagnostic performance of endocan and its Models to distinguish patients with moderate or high risk from those who have low risk. Data from this analysis were given as areas under curve (AUC), 95% CI and SE. According to Sweets, 27 the AUC higher than 0.75 was considered as a good discrimination. The statistical significance was set to two-tailed P ≤ 0.05.
Results
Table 1 shows the main characteristics of the T2D population consisted of 52.8% of men. The median age of the participants was 66 years (IQR 61–72 years) and the mean BMI was 30.7 kg/m2. A total of 30.8% were smokers. When evaluating therapy, 47.1% of patients used hypolipemics, 16.4% antihypertensives, 86.5% antihyperglycemics, and 30.8% insulin. A total of 7.7% patients had atrial fibrillation as a comorbidity. The median for T2D duration was 7 years (IQR 2–4 years).
Demographic, Clinical, and Laboratory Data in Population of Diabetics
Data are presented as arithmetic mean ± SD.
Skewed distributed data are presented as median (IQR).
Categorical data are given as absolute and relative frequencies.
BMI, body mass index; DBP, diastolic blood pressure; HbA1c, glycated hemoglobin; HC, hip circumference; HDL-c, high-density lipoprotein cholesterol; hsCRP, high-sensitivity C-reactive protein; LDL-c, low-density lipoprotein cholesterol; SBP, systolic blood pressure; TC, total cholesterol; TG, triglycerides; WC, waist circumference.
The laboratory data showed high blood glucose and HbA1c levels, median 8.0 mmol/L (IQR 6.7–9.6 mmol/L) and 7.1% (IQR 6.5–8.8%), respectively. Medians for LDL-c and serum TG were above the optimal values. Median hsCRP levels of 1.6 mg/L (IQR 0.8–2.8 mg/L) indicated low grade inflammation in most of T2D patients.
Table 2 summarizes the descriptive statistics of the estimated CHD and stroke risk score. Most patients had moderate and high risk for nonfatal eCHD risk (41.3% and 37.5%, respectively). Most patients had low and moderate risk for fatal eCHD risk (41.3% and 34.6%, respectively). However, the most patients were in the low nonfatal and fatal stroke risk categories (56.8% and 92.63%, respectively). Due to very small number of participants in the moderate and high-risk fatal stroke categories, we have not performed further statistical analysis regarding this risk.
Estimated Risks in Diabetic Population
Data are presented as median (IQR).
Categorical data are given as absolute frequencies.
eCHD, coronary heart disease; IQR, interquartile range.
Endocan levels were statistically different between low [median 22.34 ng/L (IQR 10.87–41.10)], moderate [median 33.93 ng/L (IQR 16.04–42.35)], and high [median 98.27 ng/L (IQR 55.71–124.57)] nonfatal eCHD risk (P < 0.001). Endocan levels were the highest in the high risk than in the moderate risk and the lowest in the low risk for nonfatal eCHD (Fig. 1). Also, endocan levels were statistically different between low [median 27.68 ng/L (IQR 15.85–49.18)], moderate [median 34.16 ng/L (IQR 19.52–94.29)], and high [median 98.57 ng/L (IQR 89.57–116.71)] fatal eCHD risk (P < 0.001). Endocan levels were higher in the high fatal eCHD risk category than in the low (P < 0.001) and moderate group (P < 0.05).
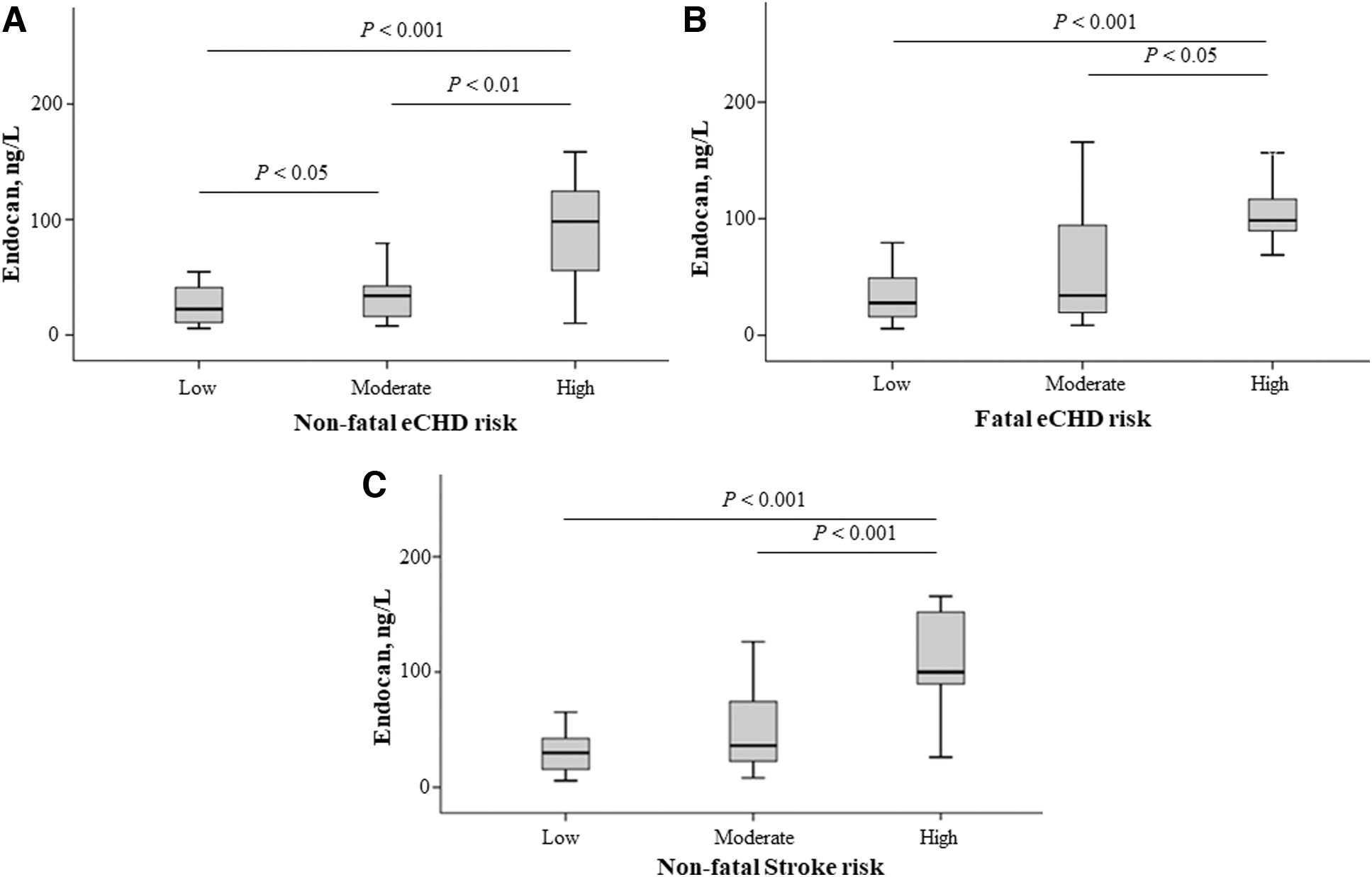
Endocan levels regarding estimated risk scores
Endocan levels were statistically different between low [median 29.85 ng/L (IQR 15.68–42.35)], moderate [median 36.18 ng/L (IQR 22.61–74.29)], and high [median 99.86 ng/L (IQR 89.57–152.00)] nonfatal stroke risk (P < 0.001). Endocan levels were higher in the high nonfatal stroke risk category than in the low (P < 0.001) and moderate risk group (P < 0.001).
Spearman's correlation analysis was used to the determine correlations between the estimated scores and clinical and laboratory markers (Table 3). All estimated scores correlated positively with age, diabetes duration, and endocan levels. Except for nonfatal eCHD, the other three risk scores correlated positively with SBP. Nonfatal and fatal eCHD risk correlated negatively with HC and HDL-c and positively with glucose. Nonfatal eCHD risk correlated positively with TG. Fatal stroke risk correlated positively with diastolic blood pressure.
Associations Between Estimated Risks and Clinical Markers Using Spearman's Correlation Analysis
Data age given as coefficients of correlation Rho (ρ).
P < 0.05; ** P < 0.01; * P < 0.001.
Univariable and multivariable binary regression analysis was assessed to test in-depth associations between endocan levels and estimated risks (Table 4). In Models, endocan was adjusted for sex and the data correlated with estimated risks with P < 0.1. Endocan as a single predictor had significant ORs for all moderate and high estimated risks except for nonfatal stroke risk. Nagelkerke R2 showed that endocan in univariable analysis could explain the variation in high nonfatal and fatal eCHD and high nonfatal stroke risk by 45.3%, 37.9%, and 55.5%, respectively. In multivariable regression analysis, endocan was the independent predictor for all moderate and high estimated risks (Table 4). Nagelkerke R2 showed that endocan could explain the variation in high nonfatal and fatal eCHD and high nonfatal stroke risk by 57.8%, 48.6%, and 68.3%, respectively.
Odds Ratios After Univariable and Multivariable Binary Logistic Regression Analysis with Enter Selection in the Best-Fit Model for Endocan Predicting Abilities Toward Estimated Risks
CI, confidence interval; OR, odds ratio; SE, standard error.
The ROC analysis was used to discriminate T2D patients with moderate and high risk for nonfatal eCHD, fatal eCHD, and nonfatal stroke risk from those with low risk (Table 4). The calculated AUCs for endocan as a single marker and in the Model predicting moderate nonfatal eCHD and moderate nonfatal stroke risks were ranking from 0.600 to 0.700. The similar AUC was for the moderate fatal eCHD risk (AUC = 0.733). These AUCs indicated low clinical accuracy of diagnostic marker and Models. On the contrary, endocan as a single diagnostic marker and in the Model for high nonfatal eCHD, in the Model for high fatal eCHD and a single marker for high nonfatal stroke risk with AUCs 0.829, 0.895, 0.860, and 0.895, respectively, indicated good clinical accuracy of endocan and the Models.
Also, endocan showed good discriminatory ability toward high fatal eCHD risk (AUC = 0.785). The calculated AUC for the Model (endocan, sex and BMI) was 0.945 demonstrating an excellent accuracy in discriminating patients with high risk for nonfatal stroke risk. As a single marker, endocan had the highest specificity (100%) for high nonfatal eCHD risk and the highest sensitivity (87.50%) for high nonfatal stroke risk. In the Models, endocan demonstrated 89.66% specificity for the high nonfatal stroke risk and 96.15% sensitivity for the high fatal eCHD risk (Table 5).
Receiver Operating Characteristic Analysis for Endocan and the Models Discriminatory Abilities Regarding Estimated Risk Scores
Discussion
This is the first study that investigated the relationship between endocan and UKPDS risk engine score in T2D patients. In addition to the independent association between endocan and eCHD risk, we have demonstrated for the first time the independent relationship between endocan and high risk for nonfatal stroke in this vulnerable population group. The calculated AUC = 0.945 for the Model that included endocan, sex, and BMI showed an excellent accuracy in discriminating patients with high risk for nonfatal stroke risk.
Although there are controversy on the utility of CVD risk scores in the cardiovascular event prediction, 3 there is an assumption that the addition of the novel serum biomarkers might improve their predictability. 12 –14 Indeed, several previous studies explored some novel biomarkers of endothelial dysfunction in relationship with UKPDS risk engine score. 28 –31 Unlike, asymmetric dimethylarginine and placental growth factor (PIGF-1), 28 hsCRP, 29 fibroblast growth factor-23, syndecan-1, and angiopoietin-2, 30,31 which did not seem reliable in CVD risk stratification, endothelin-1 (ET-1) was shown to be associated with the risk of stroke, whereas N-terminal pro B-type natriuretic peptide (NT-proBNP) correlated with several CVD risk algorithms in T2D. 28 Also, vascular endothelial growth factor (VEGF) and vascular cell adhesion molecule-1 (VCAM-1) were independently associated with CVD risk as estimated by the UKPDS algorithm and the Framingham risk score in T2D patients. 30
As multivariable regression analysis demonstrated, endocan was the independent predictor for all moderate and high estimated risks (i.e., nonfatal and fatal CHD and stroke risk scores) in our present study. Furthermore, models that included besides endocan variables such sex, HC, and/or BMI showed good clinical accuracy in discriminating T2D patients with high risk for nonfatal eCHD, fatal eCHD, and nonfatal stroke risk from those patients with low risk.
Enhanced expression of endocan was found in endothelial cells even in the first phase of atherogenesis. 15 The role of endocan in increased blood vessels permeability, migration of leukocytes and their adhesion to endothelium, and stimulation of endothelium to secrete other proinflammatory cytokines make this biomarker as a potential promising biomarker of CVD. 15,31 In line with this, endocan was higher in patients with hypertension 17 and T2D, 25 whereas its decrease was recorded after coronary artery by-pass intervention in acute coronary syndrome patients. 32
IR promotes atherogenic dyslipidemia in T2D patients by increased free fatty acids production. 21,33 The latter ones, along with an increased secretion of proinflammatory cytokines and reactive oxygen species further contribute to endothelial dysfunction. 33
We previously demonstrated positive correlation between endocan and inflammation (i.e., hsCRP), glycemic (i.e., fasting glucose and HbA1c) and lipid parameters (i.e., TG and LDL diameter), as well as an inverse correlation with HDL-c and several lipoprotein subclasses. 21 Small dense LDL (sdLDL) particles are regarded to have the most atherogenic properties due to its high susceptibility to oxidation. 34 The inverse correlation between serum endocan level and the proportion of sdLDL particles found in our previous study might be attributed to the enhanced permeability of the endothelium in T2D. 35 This might increase the penetration of sdLDL in subendothelium due to its small size, which might lead to lower serum sdLDL levels. 34,36
We also demonstrated in the previous study that higher levels of serum endocan in diabetes-free subjects with low sdLDL% and impaired glycoregulation, compared with the group with low sdLDL% and good glycoregulation, which also suggest the impact of IR on the higher serum endocan levels. 25 Moreover, a recent study 37 demonstrated an increased serum endocan levels in postprandial lipemia, which is also an independent risk factor for atherosclerotic CVD. 38
The cross-sectional nature of the study limits us to explore the causal association between endocan and UKPDS risk, as well as disables us to examine the prediction ability of endocan and UKPDS risk score for CVD events. Moreover, we were not able to include some other potential biomarkers of endothelial dysfunction in this research, which might add contribution in stratifying T2D patients with high CVD risk. Medications use and self-reported data about cigarette smoking status and duration of diabetes and atrial fibrillation might have caused some biases in this research. Also, our data could not be generalizable since we included only a small cohort of Montenegrins in this research.
Longitudinal studies with large sample size are needed to examine the causality of the relationship between serum endocan levels and UKPDS risk in different ethnic groups. Moreover, multimarker approach of some other potential biomarkers of endothelial dysfunction is recommended to increase the predictability of CVD risk algorithms in population with T2D.
Conclusion
Endocan is closely related to high CVD risk (as determined by UKPDS risk engine score) in patients with T2D. Endocan was the independent predictor for moderate and high estimated risks (i.e., nonfatal and fatal CHD and nonfatal stroke risk scores). Furthermore, when included in the models with sex and obesity indices (i.e., HC and or BMI) endocan demonstrated good clinical accuracy in discriminating T2D patients with high risk for nonfatal eCHD and fatal eCHD, and an excellent clinical accuracy for nonfatal stroke from those patients with low risk.
Footnotes
Authors' Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and laboratory analyses were performed by all authors. Statistical analysis was performed by A.N. The first draft of the article was written by A.K. and all authors commented on previous versions of the article. All authors read and approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was financially supported, in part, by a grant from the Ministry of Science and Technological Development, Montenegro and the Ministry of Education, Science and Technological Development, Republic of Serbia (Project No. 451-03-68/2020–14/200161).