
Abstract
Thyroid hormone (TH) imbalances, particularly subclinical hypothyroidism (SCHT), are associated with chronic kidney disease (CKD) and end-stage kidney disease (ESKD). SCHT is more prevalent in CKD and ESKD patients than in the general population, and this condition increases the risk of cardiovascular disease (CVD) morbidity and mortality. The risk of CVD is higher in CKD and ESKD patients compared with the general population. Traditional and nontraditional risk factors, including TH abnormalities, contribute to the high CVD burden in CKD and ESKD patients. The review discusses the link between CKD and hypothyroidism, with a focus on SCHT, and the mechanisms that lead to CVD burden.
Introduction
According to epidemiological studies, the prevalence of subclinical hypothyroidism (SCHT), ∼18%, is significantly higher in each stage of chronic kidney disease (CKD) compared with the general population. 1 –4 Reduced cardiac muscle contractility, atherosclerosis, endothelial dysfunction (ED), and systemic vascular resistance all explain why hypothyroidism is linked to more heart disease and death in the general population. 5 –7 On the other hand, in CKD and end-stage kidney disease (ESKD) patients, along with traditional risk factors, nontraditional factors additionally contribute to the high cardiovascular disease (CVD) burden, with thyroid hormone (TH) abnormalities being one of them. 8,9 Many data link TH abnormalities with cardiovascular (CV) morbidity and mortality in CKD and ESKD patients. THs are an essential regulator in the metabolism and function of many organs. Observational studies indicate a bidirectional association between SCHT and kidney disease, with hypothyroidism potentially causing kidney disease by altering renal structure and hemodynamics. 10,11
On the other hand, kidney disease, being a state of chronic low-grade inflammation, malnutrition, and metabolic acidosis, besides the exposure to dialytic procedures and medication, can indirectly alter TH levels. 12,13 Although being considerably prevalent in CKD/ESKD and linked to high CV morbidity and mortality, hypothyroidism is yet not sufficiently recognized.
Prevalence of SCHT and Association with Kidney Disease
A clinical-based classification of hypothyroidism defines overt hypothyroidism and SCHT. The last is portrayed by a lack of clinical symptoms, increased thyroid-stimulating hormone (TSH), and normal levels of thyroxine (T4) and triiodothyronine (T3). Based on the level of TSH, SCHT is proposed to be classified into two grades: grade 1 with TSH levels between 4.5 and 9.9 mIU/L and grade 2 with TSH levels higher than 10 mIU/L. Grade 2 SCHT is reported to be linked with a higher risk of CVD. 14
The prevalence of primary SCHT in the general population is reported to be 5%–10% based on the biochemical criteria of elevated serum TSH and normal T4 levels. At the same time, the wide range is due to definition, the amount of iodine in the diet, age, and how men and women are spread out. 15 –17 In the Third National Health and Nutrition Examination Survey (NHANES III), the prevalence of SCHT was 4.3%, 16 while in the Colorado Thyroid Disease Prevalence Study, conducted in 25,862 subjects by Canaris et al., SCHT was the most prevalent TH derangement found, with a prevalence of 9%. 17 Studies in the general population have shown an association between higher TSH and a lower estimated glomerular filtration rate (eGFR) independent of age, gender, or comorbidities. 18 –20
In nondialysis CKD patients, primary SCHT was found in almost 18% and showed the same trend of independent association with progressively decreasing eGFR. 1 Using data from NHANES III to evaluate the overt hypothyroidism and SCHT prevalence at various stages of CKD, Lo et al. demonstrated an incremental increase in the prevalence of hypothyroidism through CKD stages, reaching 23.1% in eGFR of 30 mL/min/1.73 m2, with SCHT accounting for 56% of overall hypothyroidism cases. 2 Between 15% to 25% of subjects with end-stage CKD who are on dialysis are referred to have SCHT. 21,22 As for renal transplantation, in a recently published study, 3.5% of subjects developed SCHT in the period 12–24 months post-transplantation. 23 In a small study, the prevalence of SCHT was 17.5%, varying from 7.69% to 35.7% depending on the duration of pretransplant hemodialysis (up to and over 72 months). 24
Reciprocal Mechanistic/Causal Link Between SCHT and CKD
Thyroid structural and functional changes found in CKD
Compared with subjects with normal kidney function, those with uremia are likelier to have a more prominent thyroid gland, thyroid nodules, and thyroid carcinomas. 25 CKD also affects how well the thyroid functions because the kidney controls how much TH is released, taken in, used, and degraded. 26 Uremia has been linked to pituitary and intrathyroidal dysfunctions, 27,28 which is supported by evidence that the hypothalamic–pituitary–thyroid axis regulation may be altered in kidney disease. 7 Due to pituitary receptors' blunted and delayed response to TSH, the uremic state decreases the release of thyrotropin-releasing hormone (TRH). Serum TSH is generally normal or elevated in CKD, but the response to TRH is low. 29 –31 Relative tissue hypoxia caused by anemia in CKD may help explain why the pituitary gland does not respond as well to TRH. 7 In ESKD, the average serum TSH pulsatile release and diurnal rhythm are also altered. 30 Even though TSH clearance is reduced by 43% in CKD, making the plasma half-life of TSH longer, the bioactivity of TSH in vivo is reduced due to changes in glycosylation. 31
Aside from the effect on the hypothalamic–pituitary–thyroid axis, changes in TH in CKD and ESKD can be driven by a drought of plasma proteins that bind T4, the presence of inhibitors that prevent T4 from binding to plasma proteins (like heparin and furosemide), the retention of 25 iodine, the effects of metabolic acidosis, and changes in how T4 is broken down at the periphery. 7,25 In kidney diseases with urinary protein loss, total body TH depletion may be partially explained by the loss of the protein-bound circulating TH. In nephrotic subjects, SCHT was six times more frequently found than the age and gender-matched controls. 32 Iodine retention through the Wolff–Chaikoff effect is also suggested as a possible mechanism for hypothyroidism in subjects with impaired kidney function. 33 TSH levels were found to be elevated in metabolic acidosis patients, and T4 and T3 levels were found to be reduced. 13 Uptake and action of TH are also disturbed in CKD. Diffusion or transport across the cell membrane is the responsible mechanism by which circulating THs enter the peripheral cell, metabolizing the intracellular T4 into T3. 25
Hormone activation is controlled through extraglandular tissues, and the TH action at the cellular level is relatively independent of its serum concentration. 34 T3 is generated by peripheral deiodination of T4 by deiodinase enzymes and bound immediately to its nuclear receptors for consecutive binding to DNA to modify gene transcription. 34,35 The process of deiodination accounts for 80% of peripheral (extrathyroidal) T3 produced from T4 and is decreased in states of uremia, inflammation, starvation, certain medications, and other clinical conditions. 7 Thus, kidney diseases affect both the peripheral transport of TH and its intracellular nuclear action. 7,35 Furthermore, in dialysis patients, selenium deficiency influences deiodinase activity. 7,35 Whether these changes reflect a physiological compensatory or pathological state remains a scientific debate. Structural and functional thyroid changes in CKD are presented in Figure 1.
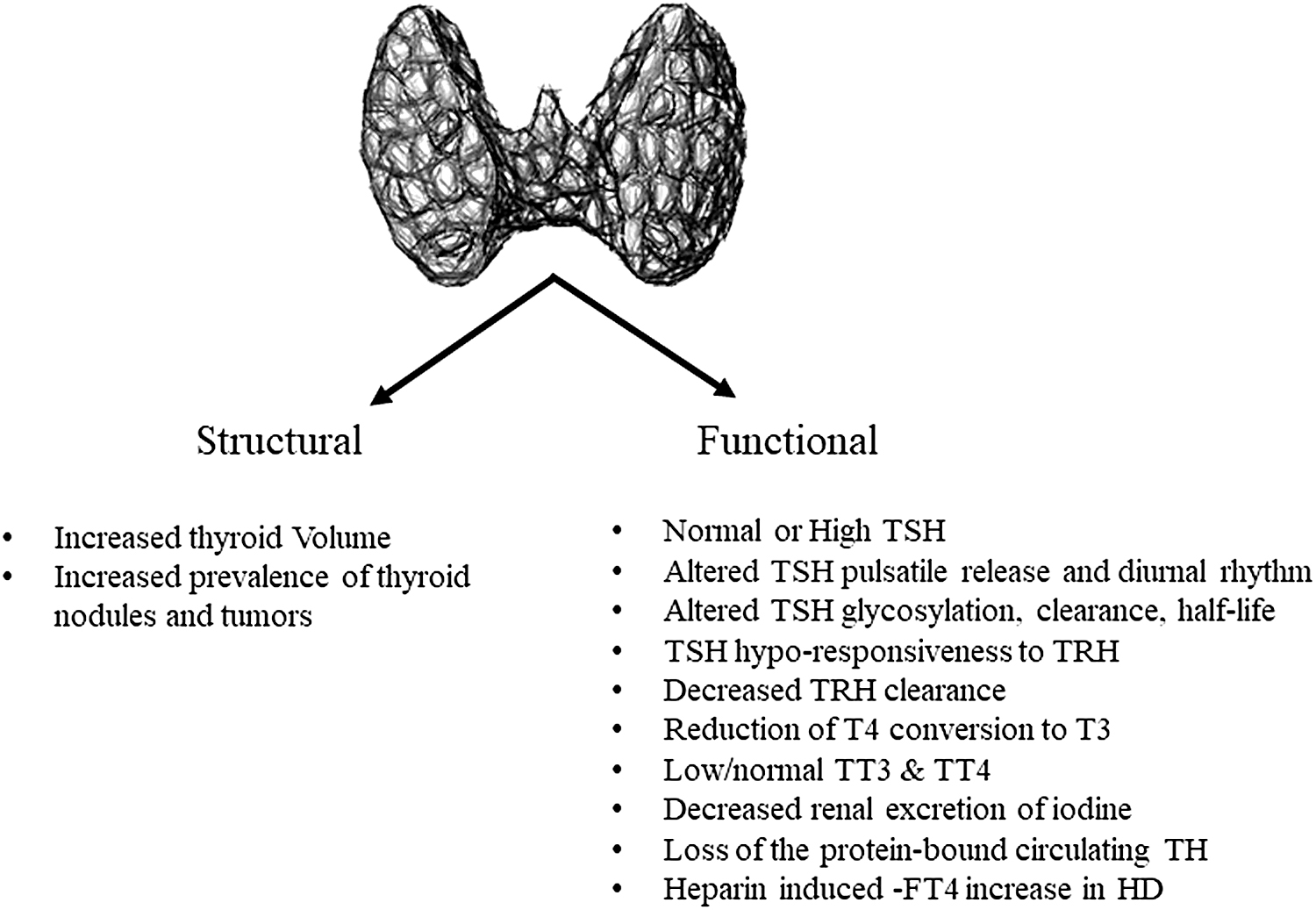
Structural and functional thyroid changes in chronic kidney disease. FT4, free thyroxine; HD, hemodialysis; T3, triiodothyronine; T4, thyroxine; TRH, thyrotropin-releasing hormone; TSH, thyroid-stimulating hormone.
Renal changes in hypothyroidism
Salt and water handling disturbances are common in people with hypothyroidism. This shows up as a decline in GFR, a decrease in the ability to concentrate and dilute, and an increase in natriuresis after volume changes (caused by salt and water loading or others).
Although human studies are scarce, experimental animal studies have shown that TH affects the way the kidneys mature, grow, and operate. Considering structural changes, hypothyroidism in animal neonates decreases the size and weight of the kidneys. When hypothyroidism is present, renal hypertrophy in kidney models was seen as insufficient after a single nephrectomy. 17,34 Even though the idea is vague, it is thought that some part of the renin–angiotensin–aldosterone system acts directly or indirectly as a TH–adaptable growth factor outside of the hemodynamic effect. 36 In this way, the tubules get shorter and thinner, as seen in histological studies of the proximal tubule, the medullary thick ascending limb, and the convoluted tubule. 11,37 Reasonably, these structural changes are reflected in tubular function, affecting the expression and activity of ionic transporters, cotransporters, exchangers, and channels. 10
The animal studies have demonstrated decreased transporting functions (Na+-K+ ATPase and H+-ATPase, Na+-HCO3- exchanger, Na+-H+ exchanger, Na+-Pi IIa exchanger, Na+-sulfate exchanger, Na+-K+-2Cl- cotransporter, Na+-Ca2+ exchanger, Cl- channel), except for aquaporins, whose function is increased. 11,34,35,37
Research has shown that rats with hypothyroidism show increased urinary sodium excretion and fractional excretion. Additionally, these rats were found to have a reduced ability to tolerate sodium restriction. 38,39 One human study found that individuals with hypothyroidism had a decreased ability to acidify their urine after an acid load. 40 However, hypothyroidism also leads to structural and functional changes in the glomerulus, including a decrease in glomerular volume and histological changes, such as an expanded mesangial matrix and thickening of the glomerular basement membrane. 7,11,26,41,42 Animal studies have also shown increased permeability of glomerular capillaries to proteins, resulting in proteinuria. 43 While evidence in humans is limited, a biopsy study in patients with hypothyroidism reported various types of glomerulonephritis. These glomerular changes contribute partially to the decreased GFR and the previously discussed hemodynamic changes. 44
A reduction in the renin-angiotensin-aldosterone system activity, seen in hypothyroidism as a direct effect of decreased renin gene expression, negatively impacts renal autoregulation and perfusion, 7,10,11 decreases cardiac output, and increases peripheral and intrarenal vascular resistances predisposing to prerenal kidney injury. 10,11
It is important to emphasize that structural and functional changes happen during development and adulthood. 16 In children with congenital hypothyroidism, there is an impact of hypothyroidism on the reduction of kidney mass and the high prevalence of urologic and renal anomalies. 45
Several cross-sectional studies have revealed that thyroid and kidney function are interrelated, with only a couple of consistent findings of the relationship between thyroid function and the development of CKD. 46 –48 Recently, a cohort in the Japanese General Population indicated that higher TSH concentrations positively correlated with CKD prevalence and that a high TSH concentration may be a risk factor for the development of CKD. 49
SCHT as a CV Risk Factor in the General Population
Concerning the CV system, all identified changes in SCHT patients are identical to those seen in overt hypothyroidism, implying that the only difference between moderate, asymptomatic, and overt hypothyroidism is simply a quantitative variation that poses a serious CV risk. 50 The effects of SCHT on CVD risk factors are presented in Figure 2.

The effects of subclinical hypothyroidism on cardiovascular disease risk factors. ↑, increase; ↓, decrease; ApoB, apolipoprotein B; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol.
Cardiac functional and structural changes
The TH plays a crucial role in regulating the CV system in adults, affecting myocardial contractility, stroke volume, heart rate, vascular function, and other factors. These effects are achieved through both genomic and nongenomic pathways, which induce cardiac structure and function adaptations. 51 However, suboptimal TH levels can lead to systolic and diastolic dysfunction and impaired exercise performance. 52
One of the most common signs of SCHT in the heart are changes in left ventricular (LV) diastolic function, which are marked by a longer isovolumetric relaxation time and an abnormal time-to-peak filling rate compared with control subjects. These alterations are linked to increased morbidity, exercise intolerance, and diastolic heart failure (HF). 53,54
The effect of T3, the active form of TH, is essential for cardiac myocyte relaxation and contraction. T3 affects the heart by positively regulating specific genes while negatively regulating the transcription of others. T3 binding promotes the activation of nuclear receptor proteins, leading to upregulating T3-responsive genes in cardiac tissue. The thyroid receptor (TR) isoform is the predominant form of TR in the human heart, impacting contractile and electrophysiological effects on the heart.
Cardiac myocyte contractility is conditional on myosin heavy chains α and β, which are inversely regulated. Besides, sarcoplasmic reticulum calcium ATPase (SERCA2) is the essential target of T3. SERCA2 sequesters calcium back into the sarcoplasmic reticulum during the myofilament contraction/relaxation phase, and T3 positively regulates it. While SERCA2 is positively held by T3, phospholamban, its inhibitory partner, is negatively regulated. Efficient calcium kinetics is critical for optimal cardiac myocyte relaxation and contraction. 55
Additionally, specific genes and nuclear receptors mediate the effects of T3 on the heart, and they impact contractile and electrophysiological properties. TH increases the gene expression of β-adrenergic receptors, enhancing the response to catecholamines. Hypothyroidism raises cardiomyocyte inducible nitric oxide synthase expression, which may contribute to decreased contractile properties, Ca2+ transient, and β-adrenergic hyporesponsiveness, leading to progressive cardiac dysfunction. 5,7,56,57 In addition to its genomic effects through nuclear receptors, TH can exert nongenomic actions by interacting with membrane integrin receptors and signal transduction pathways in the cytoplasm. 55,58 Nongenomic effects include rapid recruitment of slowly inactivating sodium channels, stimulation of Ca2+-ATPase, and augmentation of the activity of Na+/K+ ATPase.
Furthermore, TH also has a proangiogenic effect, generating rapid vascular relaxation mediated by nitric oxide (NO), promoting arteriolar growth in the normal heart and after myocardial infarction. 59 The effect of TH on the heart is based on the cardioprotection of the ischemic heart that is not limited to the cardiomyocytes but to fibroblasts and endothelial cells. TH is suggested to regulate the membrane Na+/H+ antiport, through which the myocardial function is preserved. 60
Hypothyroid status is associated with an increased risk of collagen deposition and cardiac fibrosis, which further negatively impacts diastolic functional changes. 61 According to a recent systematic analysis, both overt hypothyroidism and SCHT are linked to greater levels of diffuse cardiac fibrosis compared with euthyroidism. 62 This suggests that mechanisms such as changes in collagen gene expression, collagen deposition, mitochondrial dysfunction activity of fibrogenic cytokines, and redox balance may be involved.
Interestingly, a significant evidence of impairment of LV long-axis systolic function (the most sensitive index of systolic function) is greatly determining the overall cavity diastolic performance, as revealed by spectral Doppler studies. 51,53 In addition, the LV systolic function (assessed by 3D strain echocardiography) in SCHT patients with an average ejection fraction was significantly improved after levothyroxine (L-T4) therapy. 53 In general, patients with SCHT have a higher susceptibility to atherosclerosis, which can ultimately result in HF. This condition is often characterized by changes in cardiac contractility, which are typically reflected in echocardiographic strain values. 5,7,52,63 –65
There is reported a link between various aspects of LV mechanical function and specific CV events in patients with SCHT. Lower global longitudinal strain was associated with an increased risk of chronic heart disease, while reduced global circumferential strain was a predictor of HF 66 and congestive heart failure (CHF). 64 A significant decrease in cardiac output was attributed to several factors, including decreased peripheral oxygen consumption, cardiac preload, cardiac contractility, and increased systemic vascular resistance. 64
Notably, some researchers have pointed out that myocardial fibrosis and myocardial perfusion/metabolism mismatch may be more severe due to hypothyroidism when HF is mixed with hypothyroidism. This situation could guide to a severe myocardial damage, cardiac dysfunction, and a poor long-term prognosis. 64
SCHT is related to LV end-diastolic dysfunction, which is associated with impaired exercise capacity and predicts HF. 66,67 An underlying factor of systolic dysfunction during effort among patients with SCHT may be impaired LV diastolic function at rest. Impaired diastolic cardiac function is essential in determining exercise capacity in HF patients with diastolic dysfunction.
TH affects the heart rate and conduction and exerts its electrophysiological effect through sodium pump channels. Hypothyroidism patients exhibit a lower heart rate than hyperthyroid patients and altered chronotropy through changes in cardiac ion channels, which predispose to increased ventricular irritability, prolonged time from the start of the Q wave to the end of the T wave (QT interval), augmented risk of Torsades de Pointes, and sudden cardiac death. 5,68 Varying degrees of atrioventricular block and low QRS complexes are also viewed in patients with hypothyroidism. 51
A deficiency in TH can lead to a range of adverse effects on the heart, such as a reduced heart rate, weakened myocardial contraction and relaxation, prolonged systolic and early diastolic periods, reduced cardiac preload due to impaired diastolic function, increased cardiac afterload, and diminished chronotropic and inotropic functions. 68 Moreover, patients with SCHT may be more susceptible to atrial fibrillation due to an abnormal diastolic function of the left ventricle, an increased risk of coronary heart disease (CHD), and stiff arteries, all known risk factors for this condition. 69
TH effects on the vasculature
The effects of TH on the vasculature involve both genomic and nongenomic mechanisms that act at the level of vascular smooth muscle and endothelial cells. 53,56 Recent research has found TSH-R in microvascular endothelial cells. TH can affect these cells regardless of the peripheral TH levels. This finding has provided a new perspective on understanding the association between TH and vascular function. 70 Endothelial-dependent vasodilation is lower in SCHT patients due to the lower NO availability. ED has been identified as a contributor to increased vascular resistance, leading to increased LV afterload in SCHT. 71
Furthermore, ED in SCHT is partially associated with low-grade inflammation, oxidative stress regulation, and serum lipid levels, all of which increase the risk of atherosclerosis. SCHT patients have been found to exhibit elevated serum levels of high-sensitive C-reactive protein (CRP), interleukin-6 (IL-6), and tumor necrosis factor alpha, indicating a continuous inflammatory process. 72,73 Another potential mechanism for the impairment of endothelial function in the hypothyroid state is an increase in arginase levels in endothelial cells, which promotes oxidative stress. 74
In addition, SCHT can decrease the expression of hepatic low-density lipoprotein (LDL) receptors and the activity of cholesterol-α-monooxygenase, leading to reduced LDL clearance. This can cause dyslipidemia, which leads to higher levels of asymmetrical dimethylarginine and lessens the activity of the enzyme dimethylarginine dimethylaminohydrolase, which lowers NO production. 73,74 In this way, ED in SCHT may be an early sign of atherosclerosis and significantly affect CVD. Flow-mediated dilatation and carotid intima-media thickness (IMT) can be used to measure the risk of ED in patients with SCHT. These measures assess ED and predict the occurrence and progression of CVD. 73,75
An expanded risk of vascular calcification has been reported linked to SCHT. A significant association has been observed between low-normal free T4 (FT4) levels and a higher occurrence of subclinical coronary artery disease and raised levels of coronary calcification in a significant cohort of young and middle-aged individuals with normal thyroid function. 75 Several studies have shown that high TSH levels and low FT4 are linked to coronary artery calcification and calcification of the valves. 76
The effects of SCHT in kidney and cardiovasculature are presented in Figure 3.

Effect of subclinical hypothyroidism in kidney and cardiovasculature. ↑, increase; ↓, decrease; GBM, glomerular basement membrane; GFR, glomerular filtration rate; RAAS, renin–angiotensin–aldosterone system.
Lipid changes and atherosclerosis risk
Dyslipidemia is a significant risk factor for the development of atherosclerosis. In particular, individuals with hypothyroidism are at increased risk of developing secondary dyslipidemia. The presence of diastolic hypertension may further compound this risk. 7 In hypothyroidism, there is an increase in atherogenic lipoproteins, including total cholesterol, LDL cholesterol, and triglycerides, and a decrease in high-density lipoprotein. 74,77 Additionally, reduced LDL cell surface receptors, diminished LDL secretion into the bile, increased cholesterol absorption, and decreased cholesterol ester transferase and lipoprotein lipase activities can further contribute to lipid accumulation and hypertriglyceridemia. Even though the data are unclear, epidemiological studies have found that SCHT patients have a higher risk of atherosclerosis, coronary events, and death from CHD. 77 Regularly monitoring lipid profiles and addressing the underlying cause of dyslipidemia are essential to reducing the risk of adverse outcomes. While T4 has been suggested as a treatment option, its effectiveness remains controversial. 78
SCHT as a CV Risk Factor in CKD Population
While in the general population with hypothyroidism, the above mechanisms are responsible for CVD, in CKD, they may be further extended and amplified through activation of nontraditional pathways, such as inflammation, vascular calcification, anemia, erythropoiesis-stimulating agent (ESA) resistance, altered coagulation, and platelet activation added to impaired kidney function per se (Table 1).
Pathophysiological Mechanisms Linking Subclinical Hypothyroidism to Amplified Cardiovascular Risk in Chronic Kidney Disease Patients
BMPs, bone morphogenetic proteins; EPO, erythropoietin; Hcy, homocysteine.
Inflammation
Chronic low-grade inflammation has been shown over and over again by many studies to be a key feature of CKD. 79 The relationship between inflammation and hypothyroidism may represent an adaptive response, given that decreased concentrations of T3 are often viewed as a compensatory mechanism aimed at preserving energy stores by reducing metabolic rates. 80 However, persistently low levels of serum T3 may prompt a maladaptive response, resulting in negative prognoses in various severe illnesses, including ESKD. Unfortunately, studies investigating the association between inflammation and SCHT have yielded mixed results. 81,82 While inflammation is known to cause derangement of TH metabolism, 83 the impact of hypothyroidism on inflammation is less clearly defined. 81,82
Only a limited number of studies examining inflammation and hypothyroidism in CKD patients have established a correlation between inflammation and T3, and a weaker one with TSH. 84,85 Moreover, low T3 levels have been linked to elevated levels of inflammatory markers, such as IL-6 and CRP, and are thus considered predictors of mortality in dialysis patients. 84
Vascular and valvular calcifications
CV calcifications, which affect the valves and blood vessels, are common in CKD patients and are linked to a higher risk of death. 86
Several studies show that the link between hypothyroidism and vascular calcifications in this group of patients extends the CKD risk. In a specific group of younger people with ESKD, where free T3 (fT3) was used to show the nonthyroidal disease spectrum, there was an inverse relationship between the coronary artery calcium score and arterial stiffness. 87
These results support the idea that TH affect matrix-gla protein and klotho synthesis, as evidenced by reported positive associations between fT3 and both markers and suggest a link between nonthyroidal illness and changes in calcification inhibitor levels. Experimental studies have shown that Klotho gene expression and mRNA levels of matrix GLA, which function as inhibitors of soft tissue and vascular calcification, are downregulated. 87
Clinical studies have also shown that osteoprotegerin, a calcification marker of the arteries, atherosclerosis, and heart problems, is higher in hypothyroidism. 88
Therefore, it is essential to consider the association of hypothyroidism with CV calcification. In addition, the mechanism may involve ED, vasoconstriction, and lipid alterations due to the systemic low TH state. 77 These observations highlight the importance of monitoring and managing hormonal derangements to mitigate the risk of CVD, particularly in CKD patients, and develop effective interventions to reduce its risk.
Anemia
Anemia is found in as much as 39% of patients with SCHT, 7 that in addition may deteriorate anemia of CKD patients, 89 potentiating the CV risks. However, TH is shown to increase the production of erythropoietin by the kidneys, 90 but the mechanisms through which hypothyroidism causes anemia, although not fully understood, are more complex.
Therefore, hypothyroidism may decrease erythropoietin production and ESA responsiveness, resulting in adverse effects on iron transport and utilization. This is due to the impact of hypothyroidism on intestinal absorption of iron and its incorporation into erythrocytes, as well as a potential effect in vitamin B12 deficiency. Additionally, impaired hemostasis may lead to an increased risk of bleeding, potentially causing blood loss and anemia. These factors should be considered when managing and monitoring SCHT to avoid adverse health outcomes. 91 The coexistence of anemia and hypothyroidism might also be expected in chronic diseases characterized by inflammation, protein-energy wasting, and malabsorption. 92
Malnutrition is associated with deficiencies of crucial erythropoiesis microelements such as iron, folate, vitamin B12, as well as iodine. Iron deficiency was also linked to hypothyroidism through a decreased thyroid peroxidase activity, an iron-containing enzyme. 93 THs influence peripheral tissue oxygen consumption indirectly affecting hypoxia-inducible factor 1, which in turn induces anemia. 90
Platelet activation and thromboembolism
Extensive research has been done on the link between hypothyroidism and increased platelet reactivity, a key part of thrombosis and thromboembolic events in CVD. 94,95 A general population study revealed that hypothyroid patients had increased platelet aggregation induced by adenosine diphosphate and collagen, which normalized following TH administration. 95 However, observational studies have produced conflicting results regarding platelet aggregation in hypothyroid patients. 96 Patients with SCHT have been found to have higher mean platelet volume (MPV) and platelet distribution width (PDW) values, which are implicated in the natural history of vascular disease and can generate significant amounts of vasoactive and prothrombotic factors. MPV and PDW have emerged as risk factors for myocardial infarction, stroke, death in the general population, and CHD in dialysis patients. These findings highlight the need for close monitoring and management of hypothyroidism to prevent the development of adverse CV events. 97
Hyperhomocysteinemia
Hyperhomocysteinemia is a well-established, independent risk factor for atherosclerosis and CHD. 98 In patients with SCHT and hypothyroidism, several studies have shown increased blood homocysteine (Hcy) levels, although the mechanisms behind this remain unclear. 99,100 A negative correlation has been observed between blood Hcy levels and renal function in the general population, which may partly explain the decrease in eGFR observed in hypothyroidism and its association with Hcy elevation. According to the Framingham Offspring Study, there is evidence to suggest that Hcy is an independent risk factor for the development of future CKD or microalbuminuria. Recent research by Pan et al. suggests that there may be a feedback loop between Hcy elevation and renal function impairment, resulting in a stronger correlation between blood Hcy and eGFR, particularly in patients with SCHT and hypothyroidism. 101
Outcome and Potential Strategies of Treatment
Several studies have examined the association between SCHT and mortality in high-risk populations, including those with recent cardiac and CHD. While these studies have reported greater all-cause and CV mortality in these populations, the same has not been consistently observed in groups at average-risk levels. 102,103 A retrospective analysis of participants in NHANES III found that SCHT was associated with a greater risk of death in individuals with CHF compared with those without. 104 Furthermore, heightened levels of T3 have been identified as a prognostic indicator for mortality in the short and long term among individuals with ischemic heart disease. 105,106 A recent study of 9020 participants in the U.S. general population found a clear association between SCHT and high-normal TSH concentrations with CVD and all-cause mortality. 7 Due to the high number of people with CKD and ESKD who have structural and functional heart problems, these findings may be essential for this group. ESKD and SCHT are independent risk factors for CVD mortality, and patients with both conditions may face an even greater risk of CVD. 7
By this review we tried to bring attention to SCHT in CKD patients by portraying the physiopathology and clinical relationship between SCHT, and kidney and CV risk in CKD.
There has not been a complete biology study that looks into the link between thyroid dysfunction and the development of CVD and finds new biomarkers of the action of TH in CV tissue and how they relate to other risk factors in CKD. Importantly, no randomized controlled trials have been done to look at how well treating thyroid dysfunction affects CV health. Innovative methods like genome and whole-exome/genome sequencing, epigenetics, mRNA expression, metabolomics, omics, and other data are needed to set up a hypothalamic–pituitary–thyroid axis set-point projection model for personalized thyroid dysfunction treatment. This model can give more in-depth information about this condition and determine a patient's CV risk in CKD. 7,53 However, clinical trials that explored the possible benefits of TH supplementation on CV events in people with SCHT and CKD did not have enough power. Current data primarily stem from population-based cohort studies and meta-analyses, which suffer from inconsistent thyroid function testing across cohorts.
Furthermore, limited animal studies have investigated the effects of TH on atherosclerotic CVD, and these offer restricted data for analyzing the variations in TH impact on the vasculature by gender or ethnicity. Moreover, despite the notable changes in modifiable atherosclerotic risk factors that often accompany SCHT, such as hypercholesterolemia, diastolic hypertension, increased IMT, and reduced endothelial NO, the role of TH supplementation in mitigating ischemic reperfusion injury in humans remains uncertain, and there is currently no consensus on the optimal L-T4 dose that can potentially reverse these clinical features.
Conclusions
The prevalence of SCHT is significant among CKD/ESKD patients, and it is linked to increased CV morbidity and mortality. This review emphasizes the importance of recognizing the potential risk of SCHT in CKD and CVD. While some studies have indicated a potential association between TH levels and CV outcomes, our understanding of the underlying mechanisms and potential clinical implications remains limited. Further investigation is needed to determine the most effective approach to managing thyroid dysfunction in patients with kidney disease and to develop personalized treatment strategies that consider individual patient characteristics and risk factors. Ultimately, developing new and improved biomarkers and treatment options will be crucial in addressing the complex relationship between SCHT and CVD in this vulnerable patient population.
Ethics Statement
Ethics approval was not required for this study.
Footnotes
Authors' Contributions
The authors' contributions to this article were as follows: N.S. and M.R. conceptualized the study and drafted the original article, while M.B. and G.S. reviewed and edited it. N.S., M.R., M.B., and G.S. contributed to the visualization, and M.B. and G.S. provided supervision throughout the process. All authors have reviewed and approved the final version of the article for publication.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any external funding.