
Abstract
Background:
Chronic inflammation is believed to play a key role in managing cardiovascular disease (CVD) and glycometabolism, but the specific effects remain unclear. The subclinical features of CVD events and hyperglycemia linked to inflammatory status were evaluated in this study. In addition, independent factors associated with inflammatory status were identified.
Methods:
Inflammatory status was measured by high-sensitivity C-reactive protein (hs-CRP), CVD events estimated by carotid intima-media thickness (cIMT), and hyperglycemia determined by glycated hemoglobin (HbA1c). Univariate analysis was performed to identify the characteristics of HbA1c-defined normoglycemia, prediabetes, and diabetes, whereas multivariate linear regression analysis was conducted to identify independent factors that correlated with hs-CRP levels.
Results:
Compared with HbA1c-defined normoglycemia, individuals with prediabetes and diabetes had significantly higher risks of cIMT thickening [risk ratio (RR) was 2.21 and 2.40, respectively], carotid atherosclerosis (RR was 2.29 and 3.04, respectively), and carotid plaque (RR was 2.15 and 2.63, respectively). Diabetes had higher risks of carotid atherosclerosis (RR was 1.33) and carotid plaque (RR was 1.22) than prediabetes. Increasing prevalence of cIMT thickening, atherosclerosis, and plaque was correlated with hs-CRP levels rising. There was a notable linear relationship between HbA1c and hs-CRP levels (R 2 = 0.8685). In addition, both men and women showed an independent correlation of hs-CRP levels with HbA1c and low-density lipoprotein cholesterol, whereas men also had thyroid-stimulating hormone and women had age as an independent factor.
Conclusions:
Chronic inflammation links hyperglycemia to CVD events, and the relevant risk factors would be potential targets for alleviating inflammation and delaying the progression of the atherogenic process.
Introduction
For the past 40 years, the worldwide prevalence of diabetes and prediabetes has been increasing. In 1980, there were an estimated 108 million cases of diabetes globally, but by 2017 this number had risen to 451 million, with an expected increase to 693 million by 2045. 1 In addition, >30% of adults were estimated to have prediabetes, which refers to a dysglycemic state between normal and diabetes. 2 According to the International Diabetes Federation (IDF), the global cost of diabetes was $673 billion in 2015 and is projected to increase to $802 billion by 2040. These numbers do not even include indirect costs due to morbidity, which are also significant. 3
Diabetes is considered an independent risk factor for cardiovascular disease (CVD), a major complication affecting about one-third of people with diabetes. 4,5 CVD is now the leading cause of disability and mortality among those with diabetes and includes premature atherosclerosis that can lead to stroke, coronary artery disease, and peripheral vascular disease. 6 That is, the increased prevalence of hyperglycemia accompanies the progression of atherosclerotic cardiovascular disease (ASCVD).
Emerging evidence shows that atherosclerosis is a chronic inflammatory disease that can develop subclinically over many years, ultimately featuring immune-mediated destruction of endothelial function. 7 Independent of traditional risk factors such as physical inactivity, cigarette smoking, hypertension, obesity, or dyslipidemia, individuals with chronic inflammatory diseases bear an excess ASCVD burden. 8,9 Endothelial dysfunction occurs early in the loss of vascular homeostasis, progressing to vascular intima thickening and forming of atheromatous plaques. This progression is attributed to the production of adhesion molecules and pro-inflammatory cytokines, which promote interaction between endothelial cells and inflammatory cells, involving both innate and adaptive immunity. 10,11 Growing evidence shows a level-dependent relationship between chronic inflammation and accelerated atherosclerosis. 12
Chronic inflammation is considered either a cause or effect in the progression of insulin resistance. 13 Low-grade and long-term exposure to pro-inflammatory cytokines such as interleukin (IL)-6, IL-1, tumor necrosis factor-alpha, and oxidative stress promote β cell apoptosis and dysfunction, altering sensitivity to insulin and ultimately leading to diabetes. 14,15 In return, a state of chronic hyperglycemia promotes the glycation of proteins, lipids, and nucleic acids, and stimulates inflammation-related signaling proteins' activation. 16,17 Metabolic changes are associated with the modification of the biomolecules in diabetes, triggering characteristic macrophage activations in adipose tissue and pancreatic islets, which might elevate the interleukins levels and other chemokines. 18 Similar effects of chronic inflammation on both diabetes and atherosclerosis can be found, and hyperglycemia should either be an effect or cause of inflammation response that accompanies a higher risk of ASCVD. 19
Although a large body of evidence has shown a close relationship between hyperglycemia and atherosclerosis, the precise level-effects between them remain undetermined. In addition, the mediated or causal effects of low-grade inflammation response on both diseases require further exploration. To gain insight into relevant factors associated with inflammatory status, the potential impact factors of subclinical inflammation responses were included for adjustment, with the expectation of providing novel insight into the management of ASCVD and glycometabolism.
Materials and Methods
Study population and design
Informed consent for the human subject protocol was approved by the local ethics committee of Chongqing General Hospital. This was a cross-sectional study and the subjects were included consecutively. This study was conducted at a single center—the Health Management Center of Chongqing General Hospital. The inclusion criteria for participants were complete measurements of carotid intima-media thickness (cIMT) and glycated hemoglobin (HbA1c). The main exclusion criteria were as follows: (1) Subjects with known diseases such as tumors, acute inflammatory diseases, organ failures, or other stress state; (2) those in the presence of drug treatment; (3) those in pregnancy; (4) those with missing data; (5) those with abnormally elevated high-sensitivity C-reactive protein (hs-CRP) levels (>10 mg/L).
This study involved the participation of 9170 subjects who underwent carotid ultrasound and laboratory examinations between September 2016 and May 2021. Upon further analysis of risk factors for chronic inflammation, 5929 individuals were excluded due to missing data on hs-CRP, thyroid-stimulating hormone (TSH), and fasting plasma glucose (FPG). Furthermore, 65 individuals with abnormally elevated hs-CRP levels (>10 mg/L) were excluded to account for any possible acute effects of infection or other acute inflammations. Age information (ranging from 17 to 97 years) and gender was collected from the physical examination database.
Measurements of the serum samples
After an overnight fast, serum samples were collected in tubes sans anticoagulants. Biochemical parameters, including FPG, hs-CRP, and low-density lipoprotein cholesterol (LDL-C), were measured using an automatic biochemical analyzer (BS-2000; Mindray). TSH was gauged through chemiluminescence immunoassay (MAGLUMI X8; Snibe), and the measurement of HbA1c was carried out using high-performance liquid chromatography (H50; Mindray).
Measurements of cIMT
Carotid artery ultrasonography was performed by an experienced radiologist using a Doppler ultrasonography device (DC-80S; Mindray), and cIMT was measured in the supine position and on both sides of the neck. The measurements at 2 cm proximal to the bifurcation were performed from a longitudinal scan plane, and the mean value of multiple measures was calculated for the assessment of cIMT.
Clinical diagnostic criteria
The clinical diagnostic criteria for cIMT events were based on the intima being smooth and complete, with cIMT values <0.9 mm considered normal, values of 0.9 mm as thickened carotid intima, values ranging from 1.0 to 1.4 mm as atherosclerosis, and values exceeding 1.4 mm as an indication of the formation of carotid plaque. According to the American Diabetes Association's (ADA) 2010 criteria, HbA1c concentrations <5.7% were classified as normal, concentrations ranging from 5.7% to 6.4% indicated prediabetes, whereas concentrations >6.4% indicated diabetes. 20
Statistical analysis
The Kolmogorov–Smirnov test was used for testing the normality distribution of continuous data. Individuals' characteristics were summarized as median [interquartile range] for continuous variables and percentages for categorical variables. Potential differences among the normal, prediabetes, and diabetes groups were investigated using the Kruskal–Wallis test for continuous variables and Pearson chi-squared test for categorical variables, utilizing SPSS 20.0 (IBM Statistics). Risk ratios (RRs) and 95% confidence intervals (CIs) for cIMT events across the groups were estimated with stata 11.0 (Stata Corporation).
Because the hs-CRP level was distributed in a skewed manner, normality transformation to the normal score of hs-CRP using Blom's Formula was performed before the multivariate linear regression analysis. The multiple linear regression model was conducted through a “stepwise” method to determine independent factors associated with the normal score of hs-CRP, utilizing SPSS 20.0 (IBM Statistics). The candidate variables relevant to the normal score of hs-CRP were selected based on P < 0.10 and P < 0.05 was considered statistically significant.
Results
Characteristics of the subjects according to the HbA1c level
The study included a total of 9170 subjects with both HbA1c and cIMT measurements (Fig. 1), of which 70.28% were males and 29.72% were females. Among the male subjects 13.7% had prediabetes and 9.1% had diabetes, whereas among the female subjects 15.3% had prediabetes and 6.8% had diabetes (Table 1). In unadjusted models, individuals with prediabetes (14.2%) and diabetes (8.4%) were found to be more likely to have cIMT thickening (RR was 2.21 and 2.40, respectively), atherosclerosis (RR was 2.29 and 3.04, respectively), and plaque (RR was 2.15 and 2.63, respectively) than those with normal HbA1c levels (Fig. 2). Diabetes had a higher prevalence of atherosclerosis (RR was 1.33) and plaque (RR was 1.22) compared with prediabetes (Fig. 3).

Flowchart for the selection of study participants.
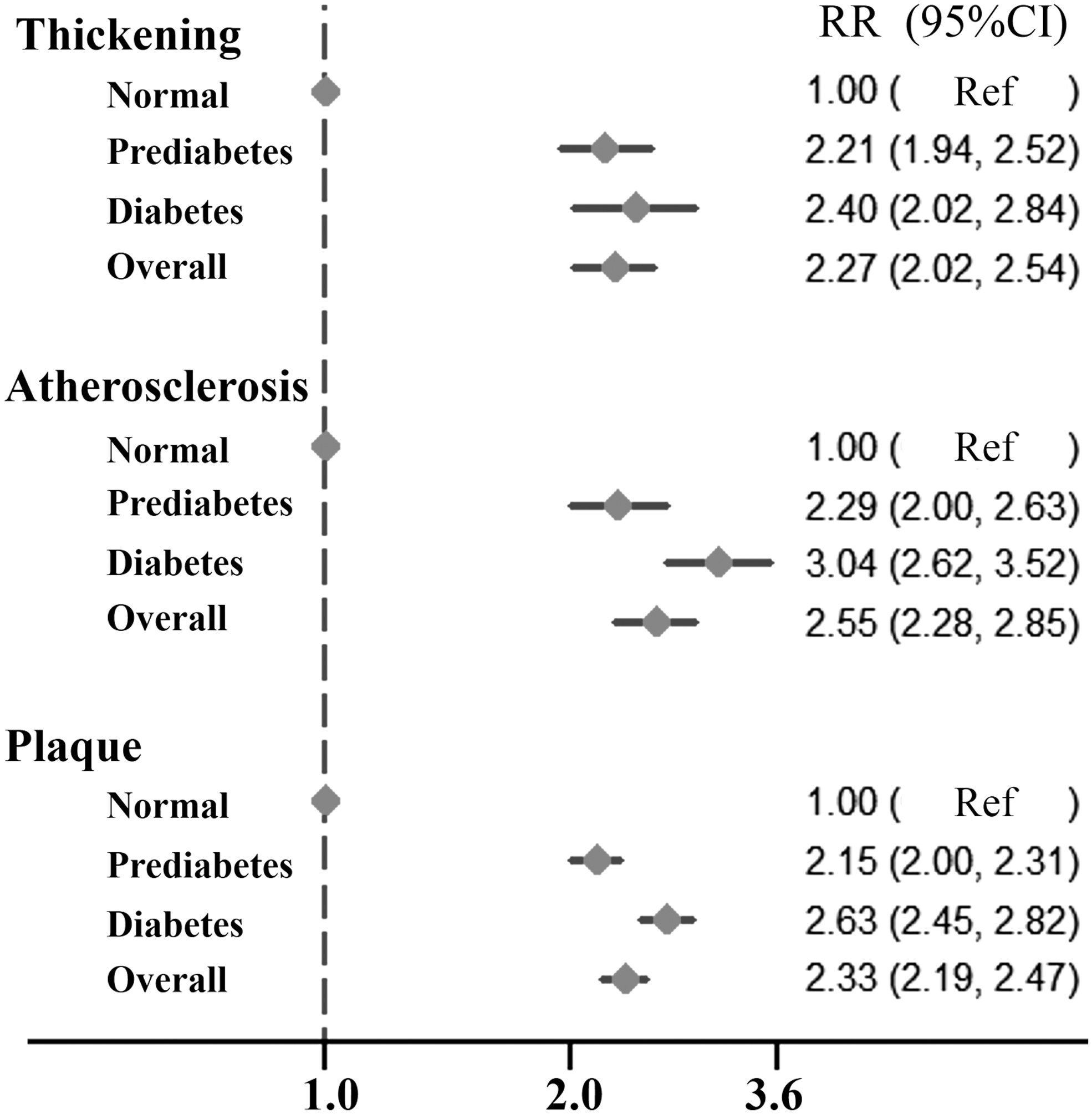
Forest plot for analysis of the incidences of CVD events in subjects with hyper-HbA1c (prediabetes and diabetes) compared with those with normoglycated hemoglobin. The subjects with normoglycated hemoglobin were regarded as references. CVD, cardiovascular disease; HbA1c, glycated hemoglobin.

Forest plot for analysis of the incidences of CVD events in subjects with diabetes compared with prediabetes. Prediabetes was regarded as a reference.
The Total Subjects with Available Data of Glycated Hemoglobin and Carotid Intima-Media Thickness Measurement (n = 9170)
Continuous variable (age) given as median [interquartile range]. Categorical variables (gender and cIMT) described as numbers (%).
cIMT, carotid intima-media thickness.
Association of increasing hs-CRP with cIMT and HbA1c outcomes
A total of 5929 subjects were excluded from the analysis due to missing data, and an additional 65 subjects were removed for having hs-CRP levels exceeding 10 mg/L. This study included 3176 individuals with complete data on covariates, including HbA1c, hs-CRP, TSH, LDL-C, and FPG (Fig. 1 and Table 2). Individuals with hs-CRP >2 mg/L exhibited a higher prevalence of cIMT thickening with an RR of 1.19 (95% CI: 1.00–1.42), atherosclerosis with an RR of 1.25 (95% CI: 1.06–1.49), and plaque formation with an RR of 1.31 (95% CI: 1.19–1.44). As shown in Fig. 4, there was an increasing prevalence of cIMT thickening, atherosclerosis, and plaque formation as hs-CRP levels rose. Furthermore, Fig. 5 demonstrated a strong linear correlation between average HbA1c and average hs-CRP levels with an R 2 value of 0.8685.

Forest plot for analysis of the incidences of CVD events in subjects with different hs-CRP levels. hs-CRP, high-sensitivity C-reactive protein.
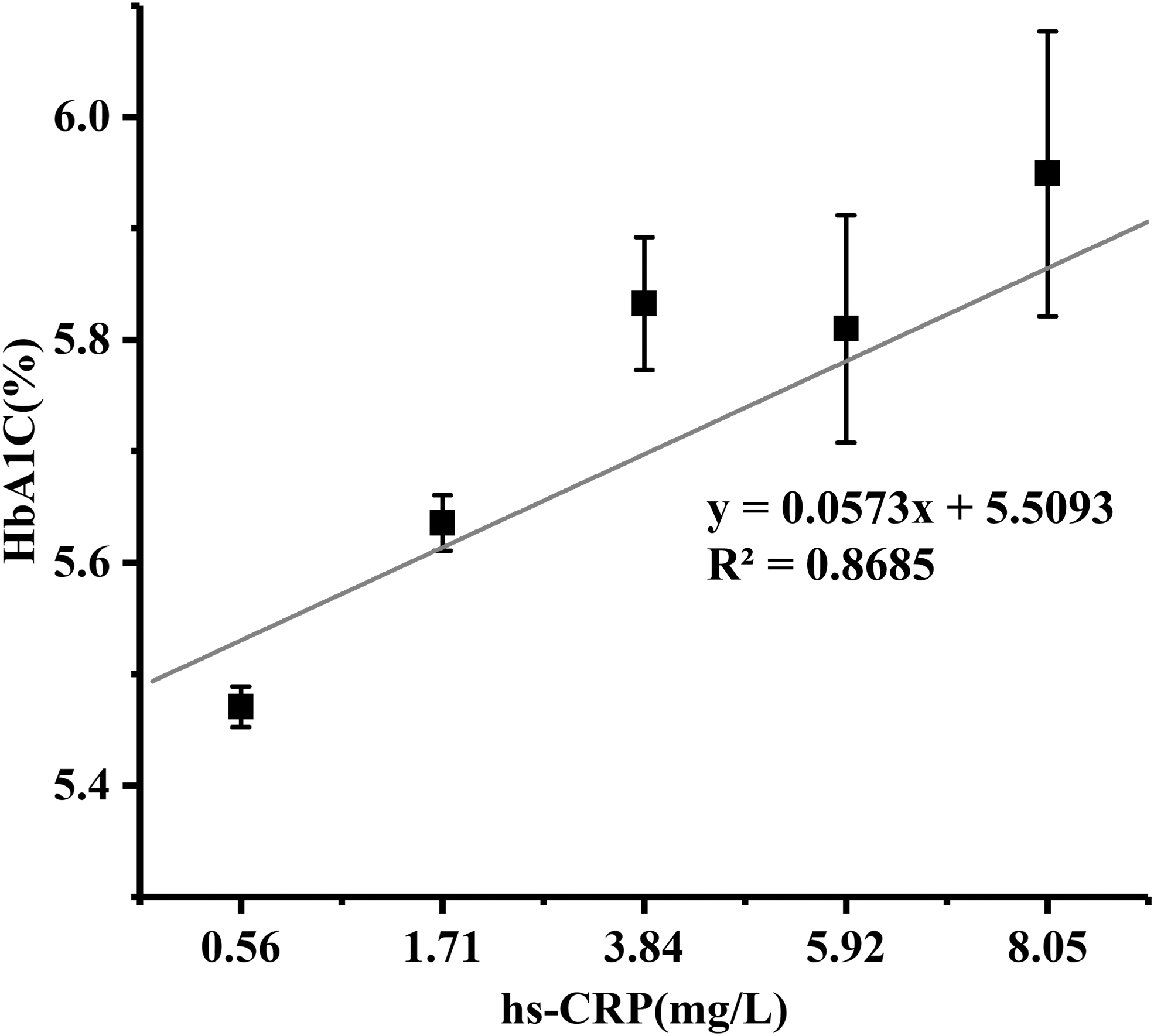
There was a linear regression relationship between average HbA1c and average hs-CRP. Group hs-CRP <1: average hs-CRP 0.56 mg/L versus average HbA1c 5.47%, Group 1 < hs-CRP <3: average hs-CRP 1.71 mg/L versus average HbA1c 5.64%, Group 3 < hs-CRP <5: average hs-CRP 3.84 mg/L versus average HbA1c 5.83%, Group 5 < hs-CRP <7: average hs-CRP 5.92 mg/L versus average HbA1c 5.81%, Group hs-CRP >7: average hs-CRP 8.05 mg/L versus average HbA1c 5.95%.
Characteristics of Participants with Normal Glycated Hemoglobin, Prediabetes, and Diabetes (n = 3176)
Continuous variables (age, TSH, FPG, LDL-C, and hs-CRP) given as median [interquartile range]. Categorical variable (gender) described as numbers (%).
CRP, C-reactive protein; FPG, fasting plasma glucose; hs-CRP, high-sensitivity C-reactive protein; LDL-C, low-density lipoprotein cholesterol; TSH, thyroid-stimulating hormone.
Multivariate analysis of the independent risk factors associated with hs-CRP level
Candidate variables, including HbA1c, LDL-C, TSH, age, and gender, were selected as available covariates. Results indicated that HbA1c, LDL-C, age, and gender were independently correlated with hs-CRP levels in the overall population. These findings revealed gender differences in factors associated with hs-CRP levels. In men, hs-CRP levels were found to be correlated with HbA1c, LDL-C, and TSH, whereas a correlation existed with HbA1c, age, and LDL-C in women (Table 3).
Multivariate Linear Regression Analysis of the Associated Factors with Normal Score of High-Sensitivity C-Reactive Protein Using Blom's Formula
β, the regression coefficients; β′, the standardized regression coefficients.
HbA1c, glycated hemoglobin; SE, standard error.
Discussion
In this study, individuals with prediabetes or diabetes were found to be with significantly higher risks of CVD events than those with HbA1c-defined normoglycemia. Diabetes also had significantly higher risks of carotid atherosclerosis and carotid plaque than prediabetes. There was an almost HbA1c level-dependent change in the risk of developing CVD events. To gain a more reasonable explanation of the relationship between these two diseases, we conducted further analysis on the interconnections of chronic inflammation with hyperglycemia and CVD events. Our findings showed a linear correlation between HbA1c and hs-CRP levels, which indicated a level-dependent correlation between hs-CRP, HbA1c, and CVD events.
Emerging evidence suggests that hyperglycemia increases the incidence of atherosclerosis by triggering early pathological processes, such as endothelial dysfunction. 12,21 Some researchers have argued that prediabetes has a higher risk for CVD events, but this excess risk may be explained by other cardiometabolic factors. 22 Correspondingly, other studies have shown that prediabetes has a significantly higher risk even after adjustment. 23 Our results support the hypothesis that hyperglycemia accelerates the development of CVD events even in the earliest stages of carbohydrate metabolism disturbance.
In addition, available research indicated that chronic inflammation is a common pathological basis of hyperglycemia and atherosclerosis. 24 It is considered to be either a cause or an effect in the progression of hyperglycemia and shows a vicious cycle between the two conditions. 19 Moreover, chronic inflammation is regarded as one of the crucial factors in the progression of atherosclerosis, which may begin at the initial stages of the pathogenic process, 25 making it a key link between hyperglycemia and atherosclerosis. Our results were consistent with previous studies showing that chronic inflammation works as a crucial bridge between the disorders of glucose metabolism and the increased incidences of CVD events. Therefore, there is reason to believe that alleviating chronic inflammation can reduce the occurrence of diabetes and cardiovascular events.
Further analysis showed that HbA1c was independently correlated with hs-CRP levels, even after adjusting for other confounding factors such as age, gender, LDL-C, and TSH. Given the significant role of chronic inflammation in CVD event progression, it might be inferred that hyperglycemia stimulates and promotes chronic inflammation leading to an increase in CVD events, which is consistent with previous studies. 12
These findings revealed gender differences in factors associated with chronic inflammation. Aging was significantly correlated with the elevated hs-CRP level in women but not in men. Previous research has indicated that estrogen exerts anti-inflammatory effects in adipocytes, which may explain why women's hs-CRP serum levels showed an age-related increase, particularly after menopause. 26 Additional factors related to inflammation found in men were LDL-C and TSH. Accumulated evidence suggests that aberrant metabolism alters the pathological microenvironment of immune-metabolic responses as well as the function of innate and adaptive immune cells. 11
This finding also confirmed that dyslipidemia was independently linked to metabolic inflammation both in men and women, which contributes to chronic diseases such as CVD and diabetes. However, there is still controversy regarding the association between thyroid function and CVD events. One study found that free thyroxine and TSH were inversely and positively associated with cIMT. 27 In contrast, another study showed that changes in free thyroxine, but not TSH, were positively associated with the incidence of carotid atherosclerosis. 28 The results of this study showed that TSH was inversely correlated with hs-CRP levels, implying that a slight increase in TSH would reduce CVD incidence by alleviating chronic inflammation.
This cross-sectional study cannot establish a cause-and-effect relationship; thus, further research using a prospective design is necessary for a more in-depth understanding of these relationships. Even though several confounders were included and adjusted based on our knowledge, additional candidate risk factors were not collected. In addition, the subjects included in this study were from a single center, and the limited population size and ethnic diversity may introduce selection bias. Finally, various etiological factors could induce systemic inflammation, and hs-CRP is widely used as a systemic inflammatory biomarker to evaluate acute and chronic inflammatory responses. Although individuals with high hs-CRP levels were excluded from this study, those with acute inflammatory responses should not be completely excluded.
In conclusion, the atherogenic process is initiated by the accumulation of lipoproteins and endothelial dysfunction, which leads to chronic inflammation even in the earliest stages of the pathogenic process. Chronic inflammation, characterized by relatively high hs-CRP levels, serves as the pathological basis for CVD events and could form a vicious cycle with hyperglycemia. Our results show a significant level-dependent correlation among hs-CRP, HbA1c, and the development of CVD events. It seems that chronic inflammation acts as a bridge between hyperglycemia and CVD events. Furthermore, several candidates, such as HbA1c and LDL-C in both men and women, TSH in men, and age (correlated with estrogen levels) in women, were independently correlated with hs-CRP levels. These risk factors would be potential targets for alleviating chronic inflammation and furtherly delaying the progression of the atherogenic process.
Footnotes
Authors' Contributions
Q.Z. supervised the whole project and drafted the article. Chunxi Wu conducted a statistical analysis and drafted the article. Other coauthors participated in drafting and revising the articles, providing suggestions on data analysis.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.