
Abstract
Background:
To explore the associations of the metabolic syndrome (MetS) and individual components with macular thickness and volume among rural-dwelling Chinese older adults.
Methods:
This population-based cross-sectional study included 705 participants (age ≥60 years) derived from the MIND-China study. In 2018–2019, we collected data through face-to-face interview, clinical examination, optical coherence tomography (OCT) examination, and blood test. We measured macular thickness and volume using spectral-domain OCT. MetS was defined following the International Diabetes Federation (IDF) criteria, the IDF/American Heart Association (AHA) criteria, the National Cholesterol Education Program-Adult Treatment Panel III criteria, and the Chinese Diabetes Society (CDS) criteria. Data were analyzed with multivariable general linear models.
Results:
MetS was significantly associated with thinner macula in central (multivariable-adjusted β = −5.29; 95% confidence interval: −9.31 to −1.26), parafoveal (−2.85; −5.73 to 0.04) and perifoveal regions (−4.37; −6.79 to −1.95) when using the IDF criteria, in the perifoveal regions (−3.82; −6.18 to −1.47) when using the IDF/AHA criteria, and in the central region (−5.63; −10.25 to −1.02) when using the CDS criteria, and with reduced macular volume when using the IDF (−0.16; −0.26 to −0.07) and IDF/AHA (−0.13; −0.22 to −0.04) criteria. In the parafoveal region, the IDF-defined MetS was significantly associated with thinner retina in men (β = −6.25; −10.94 to −1.56) but not in women. Abdominal obesity (−2.83; −5.41 to −0.25) and elevated fasting blood glucose (−2.65; −5.08 to −0.21) were associated with thinner macular thickness in the perifoveal region.
Conclusion:
MetS is associated with macular thinning and reduced macular volume among rural-dwelling older adults, and the associations vary by the defining criteria of MetS.
Introduction
The metabolic syndrome (MetS) is a constellation of multiple interrelated cardiometabolic risk factors, such as abdominal obesity, dyslipidemia, elevated blood pressure, and impaired fasting blood glucose (FBG). MetS represents one of the major public health challenges owing to its close association with cardiovascular disease and type 2 diabetes. 1 At present, MetS affects ∼25% of world adult population 2 and global prevalence of MetS has steadily increased in the past decades. 3
The retina is a part of central nervous system, with high metabolic activity and oxygen consumption. 4 The spectral-domain optical coherence tomography (SD-OCT) provides a noninvasive way for cross-sectional images of retinal biological tissues and precise quantification of retinal morphology. 5 For instance, the SD-OCT studies have shown that diabetes is associated with thinning of retinal nerve fiber layer (RNFL) or macular thickness, even before occurrence of diabetic retinopathy. 6 –8 MetS, characterized by increased oxidative stress, has been associated with retinopathy in large population-based studies. 9 –12 The clinical-based OCT studies have reported the association of MetS with peripapillary RNFL thinning in middle-aged adults. 13,14 In addition, the macula has a high density of neurons and is especially vulnerable to oxidative stress. 15,16
However, most of the previous studies have been conducted among middle-aged adults and in the clinical settings, very few population-based studies have investigated the relationship between MetS and macular parameters in elderly people, and relevant population-based studies from China are currently lacking. Furthermore, given that women have a higher prevalence of vision impairment than men, especially in low- and middle-income countries, 17 potential sex difference in the association of MetS with retinal parameters has not yet been explored. Moreover, MetS defined by different criteria has differential associations with atherosclerotic disorders, 18 and thus, the associations of MetS with retinal or macular parameters may differ by MetS definitions, which has yet to be explored.
Therefore, in this population-based cross-sectional study of rural-dwelling Chinese older adults, we sought to explore the associations of MetS and its individual components with macular thickness and macular volume by using different defining criteria for MetS, as well as the potential sex variations in these associations.
Materials and Methods
Study participants
This is a population-based cross-sectional study. The study participants were derived from the Multimodal Interventions to Delay Dementia and Disability in Rural China (MIND-China) study that targeted residents who were aged 60 years or older and living in the rural area of Yanlou Town (52 villages), Yanggu County, Shandong Province, China, as fully described elsewhere. 19 In brief, MIND-China is a participating project of the World-Wide FINGERS Network, a global interdisciplinary network of clinical trials for prevention and risk reduction of cognitive impairment and dementia. 20 In March–September 2018, 5765 participants were examined for MIND-China, during which we collected demographic, epidemiological, clinical, and biochemical data. Of these participants, using cluster (village) sampling approach, 1083 people who were free of self-reported ocular disease (e.g., diabetic retinopathy and glaucoma), ocular surgery, and ocular trauma were invited to undertake SD-OCT scans from March 2018 to June 2018 in Yanlou Town Hospital.
Of these, 378 persons were excluded owing to suboptimal image quality (e.g., signal strength less than six, segmentation errors, movement artifacts or decentration of the scanning center over the fovea) (n = 252), retinal disorders (e.g., epiretinal membrane, macular edema, and macular hole) (n = 125), and missing data on blood pressure (n = 1), leaving 705 subjects for this analysis. Figure 1 provides flowchart of the study participants.

Flowchart of the study participants. MIND-China, Multimodal Interventions to Delay Dementia and Disability in Rural China; OCT, optical coherence tomography.
Data collection
Data on demographics (e.g., age, sex, and education), lifestyles (e.g., smoking and alcohol consumption), medical history (e.g., diabetes, hypertension, and hyperlipidemia), and use of medications (e.g., hypoglycemic, antihypertensive, and hypolipidemic agents) were collected by trained medical staff following a structured questionnaire through face-to-face interviews and clinical examinations. After an overnight fast, peripheral blood samples were taken for biochemical analysis at the laboratory of local town hospital (e.g., FBG, total serum cholesterol, high-density lipoprotein cholesterol [HDL-C], and triglycerides). Height and weight were measured with participants wearing light clothes and no shoes. Body mass index (BMI) was calculated as weight (in kilograms) divided by height (in meters) squared. Waist circumference was measured at the midpoint between the lower margin of the rib cage and the iliac crest. 21,22 Arterial blood pressure was measured on the right arm with participants in the sitting position after at least a 5-min rest.
Definition of MetS
MetS was defined according to four sets of criteria that are commonly used in the literature, that is, the National Cholesterol Education Program—Adult Treatment Panel III (NCEP ATP III) criteria, 23 the International Diabetes Federation (IDF) criteria, 24 the International Diabetes Federation/American Heart Association (IDF/AHA) criteria, 25 and the Chinese Diabetes Society (CDS) criteria. 26 The commonality among the four sets of criteria for defining MetS is requiring the presence of at least three of the following five metabolic risk factors: (1) high waist circumference or high BMI; (2) high blood pressure; (3) high FBG; (4) high triglycerides; and (5) low HDL-C. The main difference among the four sets of MetS criteria is based on specific definitions of each of the five component factors.
In addition, the IDF/AHA criteria consider abdominal obesity as a prerequisite, and the CDS criteria consider HDL-C and triglycerides as one risk factor. Details of the four sets of defining criteria for MetS are summarized in Supplementary Table S1.
Ocular examination and SD-OCT image processing
Following the routine ocular examination (e.g., visual acuity and slit-lamp examination), the SD-OCT imaging scan was performed using Primus 200 (Carl Zeiss Meditec, Germany) by an experienced ophthalmic technician in Yanlou Town Hospital. This device utilizes a super luminescence diode with an 870 nm bandwidth, an acquisition rate of 12,000 A-scans/s, a tissue axial resolution of 5 μm and a transversal resolution of <20 μm. Only one eye of each participant was imaged, and the right eye was the first choice. The macular scan was performed in a dark room without pupil dilation, following the macular cube 512 × 32 scan protocol, which covers an area of 6 × 6 mm centered on the fovea. The macular thickness was computed as the distance between the internal limiting membrane and retinal pigment epithelium (RPE).
The built-in OCT software provides the macular thickness readings for nine subfields (i.e., central, inner superior, inner temporal, inner inferior, inner nasal, outer superior, outer temporal, outer inferior, and outer nasal) defined by Early Treatment Diabetic Retinopathy Study (ETDRS), 27 as well as the average macular thickness and volume over the entire ETDRS 6-mm circle. The area within the entire 6-mm circle was defined as global region. The center circle, inner ring, and outer ring bound by 1, 3, and 6-mm diameter circle were defined as central, parafoveal, and perifoveal subfields, respectively (Fig. 2).
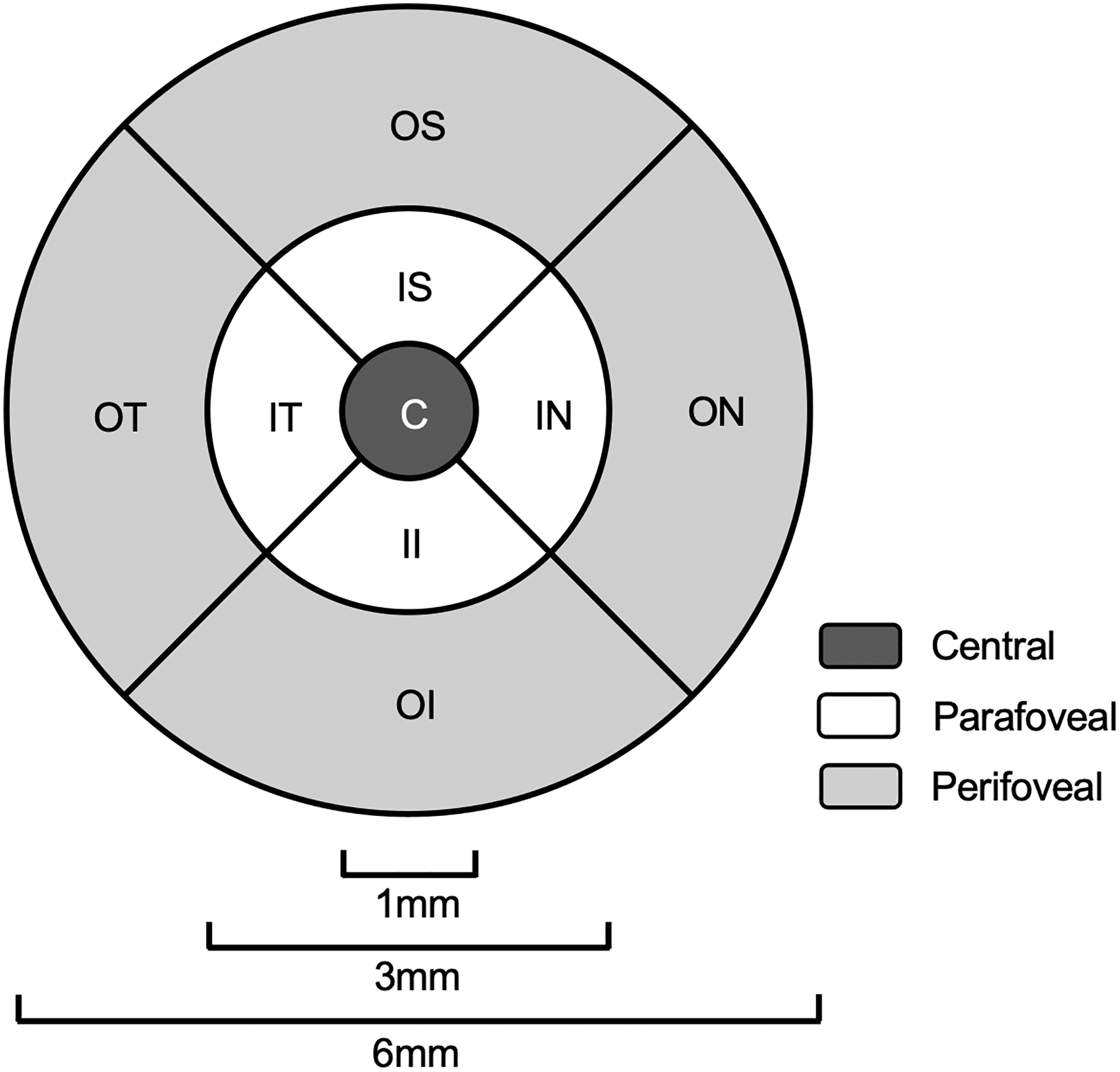
Illustration of the Early Treatment Diabetic Retinopathy Study (ETDRS) subfields. The central, parafoveal, and perifoveal subfields are shaded in blue, yellow, and green, separately. C, central; IS, inner superior; IT, inner temporal; II, inner inferior; IN, inner nasal; OS, outer superior; OT, outer temporal; OI, outer inferior; ON, outer nasal.
Statistical analysis
Characteristics of the study participants by sex were compared using Mann–Whitney U-test for continues variables with non-normal distribution, t-test for continues variables with normal distribution, and chi-square tests for categorical variables. Multivariable general linear regression analysis was performed to estimate β coefficients and 95% confidence interval of macular thickness in different regions and macular volume associated with the presence of MetS defined by the IDF, the IDF/AHA, the CDS, and the NCEP ATP III criteria and individual components (i.e., obesity, high blood pressure, high FBG, low HDL-C, and high triglycerides) defined using the IDF criteria. We performed stratified analysis by sex to examine the association of MetS with macular thickness and macular volume separately in women and men. The statistical interaction was tested by simultaneously including the independent variables and their cross-product term in the same model. We reported the main results from the models that were controlled for age, sex, education, current smoking, and current alcohol consumption.
R version 4.2.1 (R Core Team, R Foundation for Statistical Computing, Vienna, Austria) was used for all statistical analyses. A two-tailed P < 0.05 was considered statistically significant.
Results
Characteristics of study participants
Among the initial 1083 persons who were invited to undertake the SD-OCT scans in Yanlou town hospital, 378 participants were excluded owing to suboptimal image quality, retinal disorders, and missing data. Compared with those excluded participants (n = 378), participants included in the analytical sample (n = 705) were younger (mean age, 70.4 vs. 73.1 years, P < 0.001), less likely to be women (54.2% vs. 61.9%, P < 0.05), received more years of education (mean years of school education, 3.2 vs. 2.7 years, P < 0.05), and had lower systolic blood pressure (mean systolic pressure, 143.3 vs. 147.8 mmHg, P < 0.01), but the two groups did not differ significantly in the distributions of current smoking, alcohol consumption, use of medication, MetS, and other clinical data (Supplementary Table S2).
The characteristics of participants in the analytical sample by sex are given in Table 1. Depending on the defining criteria, the prevalence of MetS ranged from 21.3% by the CDS criteria and 23.3% by the NCEP ATP III criteria to 35.6% by the IDF criteria, and 38.9% by the IDF/AHA criteria. Compared with men, women were less educated (P < 0.001), less likely to smoke or drink alcohol (P < 0.001), had lower diastolic blood pressure (P < 0.001), had higher BMI (P < 0.05), triglycerides (P < 0.001), and HDL-C (P < 0.01), had a higher prevalence of MetS defined by three sets of criteria (i.e., the NCEP ATP III criteria, IDF criteria, and IDF/AHA criteria) (P < 0.001), and had a higher prevalence of obesity, low HDL-C, and high triglycerides defined by the IDF criteria. In addition, women had lower macular volume and thinner retina in all four subfields of the macula (P < 0.001). There was no significant sex difference in mean age, waist circumference, systolic blood pressure, FBG, diabetes, hypertension, the NCEP ATP III-defined MetS, and use of antihypertensive agents, antidiabetic agents, and hypolipidemic agents.
Characteristics of Study Participants by Sex
Data are given as mean (SD), unless otherwise specified.
P value is for test of difference between men and women.
IQR, interquartile range; HDL-C, high-density lipoprotein cholesterol; IDF, International Diabetes Federation; AHA, American Heart Association; CDS, Chinese Diabetes Society, NCEP ATP III, National Cholesterol Education Program—Adult Treatment Panel III.
Associations of MetS with macular thickness and volume
After controlling for age, sex, education, current smoking, and alcohol consumption, the IDF-defined MetS was significantly associated with thinner macula in the global (P < 0.001), central (P = 0.010), and perifoveal subfields (P < 0.001), and the IDF/AHA-defined MetS was significantly associated with thinner macula in the global (P = 0.004) and perifoveal subfields (P = 0.001), whereas the CDS-defined MetS was only significantly associated with thinner macula in the central subfield (P = 0.015) (Table 2). There was no significant association of any macular parameters with the NCEP ATP III-defined MetS. Moreover, MetS defined by the IDF (P < 0.001) and IDF/AHA (P = 0.004) criteria was significantly associated with reduced macular volume. In addition, there was no significant association between MetS and visual acuity (P > 0.05).
β Coefficient (95% Confidence Interval) of Macular Thickness and Macular Volume Associated with the Metabolic Syndrome
β coefficient (95% confidence interval) was adjusted for age, sex, education, current alcohol drinking, and current smoking.
0.01 ≤ P < 0.05.
0.001 ≤ P < 0.01.
P < 0.001.
MetS, metabolic syndrome.
We assessed the statistical interactions of MetS defined by all four sets of criteria with sex on macular parameters, and we only detected a statistical interaction of the IDF-defined MetS with sex on macular thickness in the parafoveal subfield (Pinteraction = 0.044). Further analyses stratified by sex suggested that the IDF-defined MetS was significantly associated with thinner parafoveal retinal thickness in men (multivariable-adjusted β = −6.25; 95% CI: −10.94 to −1.56; P = 0.009), but not in women (multivariable-adjusted β = −1.01; 95% CI: −4.65 to 2.62; P = 0.583) (Fig. 3).

Association of the metabolic syndrome with parafoveal retinal thickness by sex. The metabolic syndrome was defined according to the International Diabetes Federation criteria. β coefficient (95% confidence interval) was controlled for age, education, current smoking, and current alcohol drinking, and if applicable, for sex. **P < 0.05. MetS, metabolic syndrome; CI, confidence interval.
Associations of individual MetS components with macular thickness and volume
We defined individual components of MetS using the IDF criteria. After controlling for age, sex, education, current smoking, and alcohol consumption, obesity (P = 0.031) and high FBG (P = 0.033) were both significantly associated with thinner macula in the perifoveal region, and high FBG was also significantly associated with thinner macula in the global region (P = 0.023) and reduced macular volume (P = 0.024) (Table 3).
Association of Macular Thickness and Macular Volume with Individual Components of the Metabolic Syndrome Defined by the IDF Criteria (n = 705)
β coefficient (95% confidence interval) was controlled for age, sex, education, current smoking, and current alcohol drinking.
P < 0.05.
FBG, fasting blood glucose.
Discussion
In this population-based study of rural-dwelling Chinese older adults, we found that (1) MetS was associated with thinner macular thickness and reduced macular volume, but the associations varied by the MetS-defining criteria, (2) the association of the IDF-defined MetS with parafoveal retinal thickness varied by sex, such that MetS was associated with thinner parafoveal retinal thickness in men, but not in women, and (3) of the five MetS components defined by the IDF criteria, abdominal obesity and high FBG were associated with thinner perifoveal retinal thickness.
Our data showed that MetS was associated with thinner macular thickness in different subfields, depending on the MetS-defining criteria (i.e., the IDF, IDF/AHA, and CDS criteria). To the best of our knowledge, no population-based studies have thus far examined the association of MetS with retinal thickness parameters by using different diagnostic criteria to define MetS. Previously, the clinical-based studies of middle-aged adults showed an association of MetS with thinner macular thickness in the central and parafoveal subfields, in which MetS was defined using the NCEP ATP III criteria. 28,29 Our population-based study showed no association of the NCEP ATP III-defined MetS with retinal thickness parameters and the discrepant results may be attributed, in part, to differences in the study settings (clinical vs. the general population setting), demographic and clinical characteristics of study participants, and relatively high cutoff value of waist circumference in the NCEP ATP III criteria for Chinese adult population.
Another clinical-based study of middle-aged adults suggested that the IDF-defined MetS was associated with macular thinning in the central and inferior parafoveal subfields, 13 which is partly consistent with our results. Our population-based study revealed the associations of the IDF-defined MetS with widespread macular thinning in the central and perifoveal regions. This suggests that MetS defined using the IDF criteria may be more sensitive than other defining criteria with regard to its association with macular markers in Chinese rural elderly people. In addition, we found that MetS was associated with thinner macula in perifoveal and global regions when using the IDF/AHA criteria, and only in central region when using the CDS criteria. Abdominal obesity is a prerequisite for defining MetS in the IDF criteria, but not in the IDF/AHA and CDS criteria. It is possible that abdominal obesity could exacerbate retinal thinning, depending on other coexisting metabolic abnormalities.
Furthermore, the strict cutoffs for high blood pressure and high blood glucose in the CDS criteria may increase diagnostic specificity but decrease the sensitivity for identifying retinal alterations. The various degrees of macular thinning across different subfields might be attributable to different cellular composition in these subfields. For instance, central fovea has a high concentration of cone photoreceptors and a low density of ganglion cells, whereas parafovea has a higher density of ganglion cells and perifovea has a higher concentration of rod photoreceptors. 30 However, we were unable to further examine specific retinal layers or cell types owing to lack of data on different retinal layers.
The mechanisms underlying the association of MetS with macular thinning are not fully understood and can only be speculated. First, the chronic oxidative stress in MetS may lead to retinal inflammation, especially in macular region, which is one of the most metabolized parts of human body, 4 with a high density of photoreceptors that are polyunsaturated fatty acid-rich and are susceptible to oxidative damage. 15 Elevated oxidative stress is mainly caused by mitochondrial dysfunction, proinflammatory state, and impaired antioxidant system. 31 Second, MetS is known to be correlated with endothelial dysfunction, 32,33 partly owing to oxidative stress, hyperglycemia, hypertension, and dyslipidemia. These conditions may cause retinal microvascular alterations and blood–retinal barrier dysfunction. Indeed, MetS was associated with retinal microvascular changes, independent of diabetes, among middle-aged population. 9,10 Subsequently, experimental research has detected impaired blood–retinal barrier permeability and neuronal impairment in the retina of mouse model of MetS. 34
Third, hyperglycemia- and obesity-related insulin resistance plays an important role in pathophysiology of MetS. 35 Deficiency in insulin signaling pathway impairs the regulation of synaptic plasticity and neuronal survival, 36 which may contribute to retinal neurodegeneration. Finally, it has been hypothesized that the abnormal metabolic conditions may induce retinal neuronal loss, 34 thereby leading to macular thinning in people with MetS.
Previous studies have reported that women, older age, and Asians tend to have thinner macular thickness. 37 Our data showed that women had thinner macular thickness than men in all subfields, which is in line with previous studies. 37 –40 Furthermore, we identified a potential interactive effect between sex and the IDF-defined MetS on parafoveal retinal thickness, such that the association of the IDF-defined MetS with thinner parafoveal retinal thickness was evident only in men but not in women. Previous studies have not reported the sex difference in the association of MetS with retinal thickness. Indeed, sex hormones affect the regulation of retinal physiopathology through sex hormone receptors in the retina for both genomic and nongenomic pathways. 41,42
In addition, it has been well documented that women are less susceptible to oxidative stress than men, which might be owing partly to antioxidative properties of estrogen, sex differences in the expression and activities of antioxidant enzymes, or other yet undefined mechanisms. 43 Whereas female participants in our study were mostly postmenopausal with low levels of estrogen, we hypothesized that this sex difference in late life might have resulted from a complex interplay of lifelong sex hormones with sex differences in oxidative stress mechanisms and retinal physiopathology. 41 –45 Further prospective cohort studies are needed to explore the potential role of age-related alteration in sex hormones of both estrogen and androgens in pathophysiology of MetS. However, women were more likely to be excluded from the final analyses than men mainly owing to suboptimal image quality and retinal disorders, which might potentially lead to an underestimation of association between MetS and macular thickness in women.
We also examined the associations of the MetS components with macular thickness and volume. Our study showed that of the five MetS components, reduced macular thickness and volume were mostly associated with obesity and high FBG. Accumulation of visceral fat, which is thought to be involved in abdominal obesity, 46 has been associated with thinner RNFL thickness in a clinical-based study. 47 Our study showed that abdominal obesity (defined as waist circumference ≥90 cm for men and ≥80 cm for women) is associated with thinner perifoveal retinal thickness. We did not find evidence supporting an association of macular thickness with elevated triglycerides, reduced HDL-C, or elevated blood pressure, which is similar to the findings from previous studies. 38,48 –50
Long-term diabetes is known to cause retinopathy, and may have an impact on early retinal neurodegeneration, thus causing thinning of the RNFL, ganglion cell complex, and ganglion cell-inner plexiform layer. 7,8,51 The Maastricht study from the Netherlands suggested that macular thickness was reduced in people with prediabetes or diabetes, even before the development of clinical diabetic retinopathy. 8 In line with this report, our study observed an association of high FBG (≥5.6 mM) with thinner macular thickness in global and perifoveal subfields.
Our study is the first population-based study to explore the association of MetS with macular parameters among rural-dwelling Chinese older adults. In addition, we used four different sets of criteria to define MetS; thus, we were able to compare different definitions and identify the MetS defined by which criteria is most strongly associated with macular thickness and volume in Chinese elderly population. Our study also has some limitations. First, this was a cross-sectional study, which cannot establish any causal relationship and the cross-sectional association might be subject to selective survival bias. Second, owing to lack of data on the thickness of retinal layers, we were unable to assess which specific retinal layers or retinal cell types were associated with MetS.
Third, we did not have OCT angiography data or quantitative assessments of drusen and RPE thickness; thus, we were not able to evaluate the association of MetS with parameters of microvascular structural and oxidative stress-related retinal alterations, which would shed more light on the neurodegenerative mechanisms underlying the association between MetS and macular thinning. Fourth, the control group in the analysis included individuals with one or two MetS components, which might lead to the underestimation of the association between MetS and health outcomes (e.g., macular parameters), as previously reported. 52 Finally, our study sample was derived from one rural area of western Shandong province, where older adults had limited education and relatively low income. Thus, caution is needed when generalizing our study findings to other populations.
Conclusion
In conclusion, we found that MetS, especially the IDF-defined MetS, was associated with thinner macular thickness and reduced macular volume among older adults living in rural China, and that the association of the IDF-defined MetS with parafoveal retinal thickness was evident only in men. These findings suggest that MetS may be involved in the development of retinal neurodegeneration. Retinal examination among local rural-dwelling older adults with MetS may have a potential implication for early detection and precision prevention of retinal neurodegeneration. Further longitudinal studies are needed to explore the potential causal role of MetS and its components in retinal neurodegeneration in older adults as well as the underlying inflammatory mechanism and potential effect of anti-inflammatory therapy on the MetS-induced retinal neurodegeneration.
Footnotes
Acknowledgments
The authors thank all the participants of the MIND-China OCT subproject as well as clinical and research staff in MIND-China Study Group for their collaboration in data collection and management. In addition, the authors thank Dr Heather Snyder for valuable comments to help improve the article.
Authors' Contributions
C.Z., Q.Z., Y.W., Y.Du, and C.Q. contributed to the study design. C.Z., Q.Z., Y.W., R.L., Y.Dong, Z.S., and Y.S. contributed to the data collection and assessments. C.Z. and R.L. conducted the data analysis. C.Z. drafted the first version of the article. Y.Du and C.Q. supervised this study. All authors contributed to the critical revision and approved the final version of the article.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee at Shandong Provincial Hospital affiliated to Shandong University, Jinan, Shandong, China (LCYJ: NO. 2018–014). Written informed consent was obtained from all participants or, in the case of cognitively impaired persons and illiterate persons, from a proxy (usually a family member). MIND-China was registered in the Chinese Clinical Trial Registry (Registration No.: ChiCTR1800017758, 13/08/2018).
Availability of Data and Materials
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request and approval by the MIND-China Steering Committee at Shandong Provincial Hospital, Jinan, Shandong, China.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This study was supported in part by grants from the National Key Research and Development Program of China (Grant No. 2017YFC1310100), the Academic Promotion Program of Shandong First Medical University, and the Taishan Scholar Program of Shandong Province, China, Shandong Province postdoctoral innovation research program. C Qiu received grants from the Swedish Research Council (VR, Grant Nos. 2017–05819 and 2020–01574), the Swedish Foundation for International Cooperation in Research and Higher Education (STINT, Grant No. CH2019–8320) for the Joint China-Sweden Mobility Program, and Karolinska Institutet (Grant Nos. 2018–01854 and 2020–01456), Stockholm, Sweden. The funding agency had no role in the study design, data collection and analysis, writing of this article, or decision on publishing.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.