
Abstract
Objective:
We assessed whether alanine aminotransferase/aspartate aminotransferase (ALT/AST), a marker of hepatic steatosis, may be associated with adipose tissue dysfunction more closely than hepatic and muscle insulin resistance (IR).
Methods:
Associations with adipose tissue IR index (AT-IR) calculated as a product of fasting insulin and free fatty acids, leptin/adiponectin ratio, a proxy of adipocyte dysfunction, homeostasis model assessment IR (HOMA-IR), hepatic and muscle IR inferred from plasma insulin kinetics during a 75 grams oral glucose tolerance test (OGTT) were studied in nondiabetic 307 young and 148 middle-aged Japanese women, whose body mass index averaged 20 and 22 kilograms/m2, respectively.
Results:
On multivariate linear regression analysis in young women, ALT/AST was associated with trunk/leg fat ratio (standardized β = 0.202, P = 0.007), a marker of abdominal fat accumulation, and AT-IR (standardized β = 0.185, P = 0.003) independently of HOMA-IR and Matsuda index (R 2 = 0.07). In middle-aged women, leptin/adiponectin ratio (standardized β = 0.446, P < 0.001) and AT-IR (standardized β = 0.292, P = 0.009) emerged as determinants of ALT/AST independently of trunk/leg fat ratio, OGTT-derived hepatic IR, leptin, and adiponectin (R 2 = 0.34).
Conclusions:
ALT/AST was associated with AT-IR and adipocyte dysfunction more closely than hepatic and muscle IR even in nondiabetic lean Japanese women.
Introduction
Insulin resistance (IR) plays a key role in nonalcoholic fatty liver disease (NAFLD), 1 defined by the excess accumulation of fat in the liver, in the absence of excessive alcohol consumption and other causes of hepatic steatosis. Although NAFLD is closely associated with obesity, it is increasingly being identified in nonobese individuals. 2 This may be explained by the adipose tissue expandability and lipotoxicity hypothesis. 3 It is proposed that impaired expansion of subcutaneous adipose tissue, the largest and best storage site as triglycerides, may lead to increased free fatty acid (FFA) flux from dysfunctional adipose tissue to the liver, and to ectopic lipid accumulation in the liver, which consequently results in NAFLD in nonobese people. 4,5 It is reported that lean/nonobese NAFLD is mainly prevalent in Asian populations 5 and that have a reduced ability to expand the subcutaneous adipose tissue. 6 For example, a study on Japanese and non-Hispanic White men showed that liver fat content was higher among Japanese men despite a lower mean body mass index (BMI). 7 This ethnic difference became more robust with a small increase in BMI, suggesting that fatty liver may be a sensitive marker for the failure of the adipose tissue to expand in Japanese. 7
Gold standard to measure liver fat content and multitissue IR is proton magnetic resonance spectroscopy and a euglycemic-hyperinsulinemic clamp procedure and stable isotopically labeled tracer infusions, respectively. Multiple studies employing gold standard methods in overweight/obese nondiabetic adolescents and adults 8 –12 showed that increased liver fat was associated with IR in liver, skeletal muscle, and adipose tissue. A study employing gold standard methods in nonobese Japanese men revealed that fatty liver was associated with IR in adipose tissue, the liver, and muscle and suggests that fatty liver may be a useful clinical marker to predict IR in nonobese Japanese men. 13 Bril et al. 11 carefully evaluated a cohort of 352 adults, in whom obesity and type 2 diabetic were found in 71% and 61%, respectively. They employed gold standard to measure liver fat content and multitissue IR, and a liver biopsy. They found that adipose insulin sensitivity showed a continuous worsening across the spectrum of liver fat accumulation. In contrast, liver insulin sensitivity was affected early on after liver fat content was ∼1.5% and remained uniformly impaired, regardless of further liver fat accumulation. Muscle insulin sensitivity showed a gradual impairment at low degrees of liver fat accumulation, but remained unchanged after liver fat content reached the ∼6 ± 2% threshold. They conclude that liver fat accumulation is strongly associated with adipose IR, supporting the current theory of lipotoxicity as a driver of liver fat accumulation. 11
We tested whether alanine aminotransferase/aspartate aminotransferase (ALT/AST), a proxy of hepatic steatosis, 14 –19 may be associated with adipose IR and adipocyte dysfunction more closely than hepatic and muscle IR even in nondiabetic, nonobese Japanese women, in whom we have recently shown associations of ALT/AST with IR and β-cell function. 20
Methods
We examined 311 young and 148 middle-aged women as previously reported. 20 –22 Young women were female Japanese students of Department of Food Sciences and Nutrition, Mukogawa Women's University, and middle-aged women were their biological mothers of 148 students who participated in the study. Of 148 middle-aged women, 11 women (11.4%) reported that they were menopausal. Subjects with clinically diagnosed acute or chronic inflammatory diseases, endocrine, cardiovascular, hepatic and renal diseases and those on hormonal contraception and on a diet were excluded from the study. The study was approved by the Ethics Committees of the Mukogawa Women's University (No. 07-28 on 19/02/2008). This research followed the tenets of the Declaration of Helsinki. All participants gave written informed consent after the experimental procedure had been explained.
Blood samples were obtained in the morning after 12-hr overnight fast. Oral glucose tolerance test (OGTT) was performed with 75 grams glucose administration in 118 female students and 65 mothers. Blood samples were taken at min 0 (fasting), 30, 60, and 120 for glucose and insulin analysis. Plasma glucose was determined by the hexokinase/glucose-6-phosphate dehydrogenase method [interassay coefficient of variation (CV) <2%]. Serum insulin was measured by an ELISA method with a narrow specificity excluding des-31, des-32, and intact proinsulin (interassay CV <6%). Serum liver enzymes were measured using an autoanalyzer (AU5232; Olympus, Tokyo, Japan). Serum concentrations of leptin and adiponectin were measured as previously reported in detail. 21
Liver IR and muscle insulin sensitivity were determined by homeostasis model assessment IR (HOMA-IR), the product of fasting concentrations of insulin and glucose, 23 and Matsuda index using glucose and insulin levels during OGTT, 24 respectively. OGTT-derived liver IR was calculated as previously described. 25 The product of fasting concentrations of insulin and FFA is a validated index of the adipose tissue IR (AT-IR). 26 We showed that this index may be useful in assessing adipose IR even in women without diabetes and obesity. 27 The ratio of serum leptin to adiponectin ratio (LAR) was used as a marker of compromised adipose tissue function. 28
Anthropometric indices were measured after an overnight fast. Whole-body dual-energy X-ray absorptiometry (DXA) (Hologic QDR-2000, software version 7.20D, Waltham, MA) was used to measure lean tissue mass, fat mass, and bone mineral mass for arms, trunk (upper-body), legs (lower-body), and the total body. 21 The leg includes gluteal and femoral region. The ratio of trunk/leg (gluteofemoral) fat was considered as a marker of abdominal fat accumulation. 29
Data were presented as mean ± SD unless otherwise stated. Bivariate correlations of ALT/AST with anthropometric and metabolic parameters were evaluated by Pearson's correlation analysis. Stepwise multivariate linear regression analyses were performed to further identify the most significant variables contributing to the variation of ALT/AST. Variables which showed significant associations with the ratio were included as independent variables. Comparisons between two groups were made with two-sample t-test. Differences among three groups were analyzed using analysis of variance and then Bonferroni's multiple comparison procedure. A two-tailed P < 0.05 was considered statistically significant. All calculations were performed with SPSS system 23 (SPSS, Inc., Chicago, IL).
Results
Although middle-aged mothers and their daughters were nonobese rather slim and had normal mean serum ALT and AST (Table 1), middle-aged mothers had higher BMI, percentage body fat, waist circumference, and trunk/leg fat ratio and hence, higher serum ALT, AST, and ALT/AST. However, their BMI, waist, and ALT averaged 22 kilograms/m2, 79 cm, and 20 U/L, respectively.
Anthropometric, Clinical, and Metabolic Features of Young and Middle-Aged Japanese Women
Mean ± SD.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; AT-IR, adipose tissue insulin resistance; BMI, body mass index; HOMA-IR, homeostasis model assessment-insulin resistance; FFA, free fatty acid; OGTT, oral glucose tolerance test.
OGTT revealed that 7 of 118 young women 30 and 11 of 66 middle-aged women 31 had prediabetes, whereas none had diabetes. Middle-aged women had higher fasting glucose but lower insulin and hence HOMA-IR did not differ between two groups (Table 1). There was no difference in fasting FFA, Matsuda index, AT-IR, and OGTT-derived hepatic IR between two groups of women. Although serum leptin was lower in middle-aged mothers, adiponectin and LAR did not differ.
In young and middle-aged women, ALT/AST showed positive associations with BMI, trunk/leg fat ratio, fasting insulin, HOMA-IR, and AT-IR and inversely with Matsuda index (Table 2). In middle-aged women but not in young women, ALT/AST showed positive associations with waist, percentage body fat, fasting glucose, hepatic IR, leptin, and LAR and inversely with adiponectin.
Simple Linear Correlation Analyses of Alanine Aminotransferase/Aspartate Aminotransferase in Young and Middle-Aged Japanese Women
Data are correlation coefficients (r). Significant correlations are indicated by bold figures.
Middle-aged women were grouped according to tertile of ALT/AST (Table 3 and Fig. 1). Significant differences were found in all variables that showed significant associations with ALT/AST, except for fasting glucose and OGTT-derived hepatic IR.
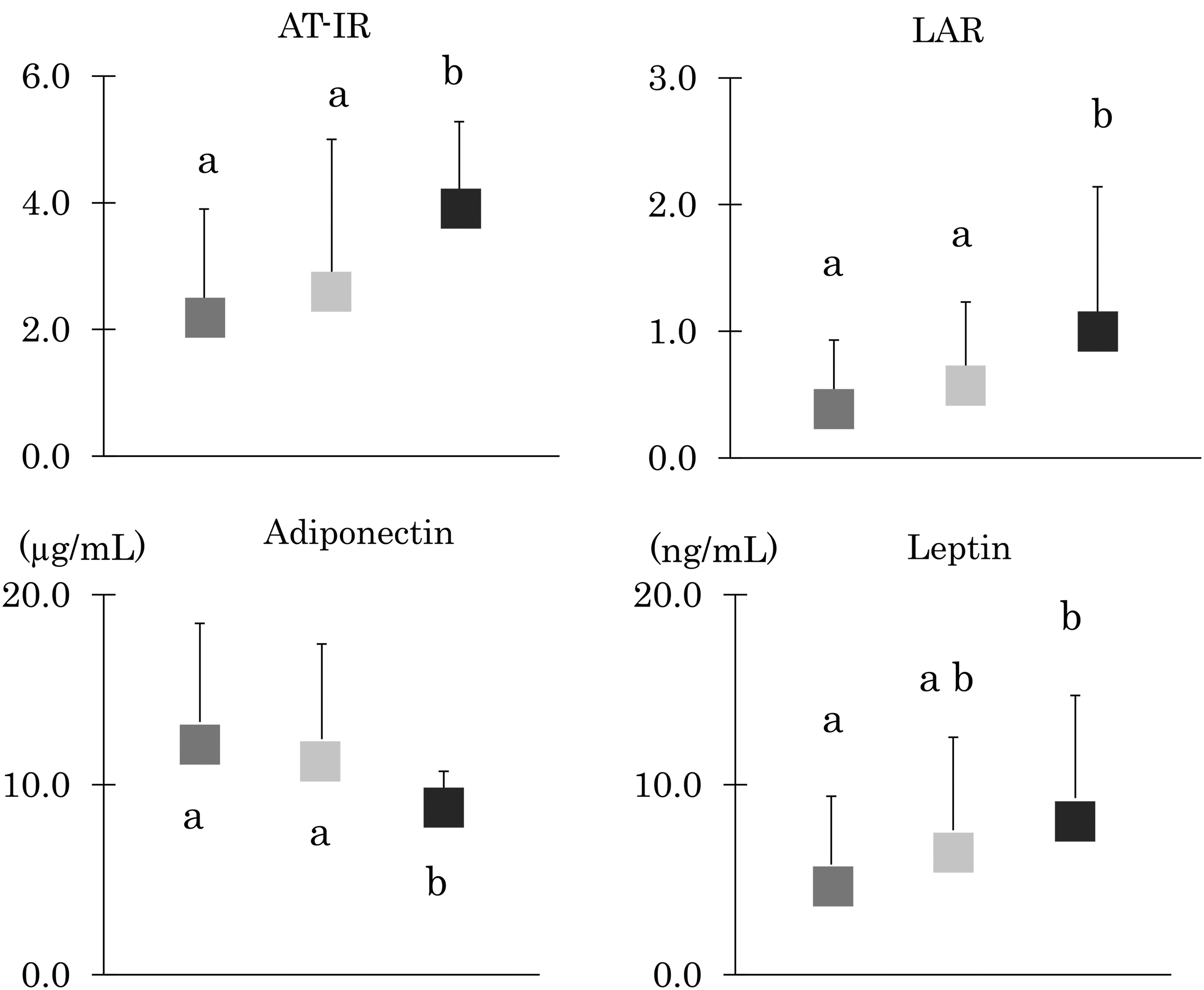
AT-IR, LAR, serum leptin, and adiponectin in middle-aged Japanese women grouped according to tertile of alanine aminotransferase/aspartate aminotransferase. Mean ± SD. Means not sharing common letter are significantly different with each other at P < 0.05 or less by Bonferroni's multiple comparison procedure. Right, middle, and left symbols in each variable represent the low, median, and high tertile, respectively. AT-IR, adipose tissue insulin resistance index; LAR, leptin to adiponectin ratio.
Middle-Aged Japanese Women Grouped According to Tertile of Alanine Aminotransferase/Aspartate Aminotransferase
Mean ± SD of n = 49 or 50.
#, P < 0.05 or less by Bonferroni's multiple comparison procedure; a, low versus median; b, low versus high; c, median versus high.
% Body fat, percentage body fat; LAR, leptin to adiponectin ratio.
We have done multivariate linear regression analysis for ALT/AST as a dependent variable (Table 4). In young women, we included trunk/leg fat ratio, AT-IR, HOMA-IR, and Matsuda index as independent variables. Trunk/leg fat ratio and AT-IR emerged as independent determinants of ALT/AST but explained only 7.5% of its variability. In middle-aged women, OGTT-derived hepatic IR, leptin, adiponectin, and LAR in addition to trunk/leg fat ratio, AT-IR, HOMA-IR, and Matsuda index were included as independent variables. LAR and AT-IR emerged as independent determinants of ALT/AST and explained 35.0% of its variability. When LAR was removed from the model, adiponectin (standardized β = 0.283, P = 0.011) and leptin (standardized β = 0.283, P = 0.015) as well as AT-IR (standardized β = 0.255, P = 0.03) emerged as determinants of ALT/AST and explained 30.5% of its variability.
Multivariate Linear Regression Analysis for Alanine Aminotransferase/Aspartate Aminotransferase as a Dependent Variable in Young and Middle-Aged Japanese Women
Independent variables included in both young and middle-aged women: trunk/leg fat ratio, adipose tissue insulin resistance index, homeostasis model assessment-insulin resistance, and Matsuda index. In addition to these variables, OGTT-derived hepatic insulin resistance, leptin, adiponectin, and leptin/adiponectin ratio were further included in middle-aged women.
Discussion
As previously reported in overweight/obese nondiabetic individuals using the gold-standard techniques to measure liver fat content and multitissue IR, 8 –12 the current study showed that a marker of hepatosteatosis (ALT/AST) 14 –19 was associated with markers of IR in the liver, adipose, and muscle tissue (HOMA-IR, 23 AT-IR, 26 and Matsuda index, 24 respectively) in nonobese nondiabetic Japanese young and middle-aged women. In addition, ALT/AST was also associated with trunk/leg fat ratio, a marker of abdominal fat accumulation, 29 in young and middle-aged women. Further, the ratio was associated with serum adiponectin, leptin, LAR, a proxy of adipose tissue dysfunction, 28 and OGTT-derived hepatic IR in middle-aged women. Among these variables, AT-IR and trunk/leg fat ratio emerged as independent determinants for ALT/AST in young women and AT-IR and LAR in middle-aged women.
Studies showed that adipose IR plays a key role in the development of metabolic and histological abnormalities in obese patients with NAFLD. 10,11 In this study, the association of ALT/AST, a proxy of NAFLD, with a marker of adipose IR was independent of, and stronger than that with markers of hepatic and muscle IR even in young Japanese women, whose waist averaged 71 cm and ALT 13 U/L, suggesting minimum abdominal and hepatic lipid accumulation, respectively. These findings may be related to a study which showed that in patients with NAFLD adipose IR (but not hepatic IR) and liver triglyceride content are major factors in the elevation of circulating ALT levels 32 and suggest an importance of adipose IR as an early player in the development of metabolic abnormalities in NAFLD. As previously reported in Japanese, Chinese, and Korean general populations, 33 –35 an association of ALT/AST with HOMA-IR was confirmed in young Japanese women.
Ruhl and Everhart 36 examined the contributions of body composition measured by DXA to increased serum ALT activity among 11,821 adults without viral hepatitis. They found that among women greater trunk fat and lesser leg fat were independently associated with increased ALT, a marker of NAFLD. These findings may be associated with the current finding of an independent association of ALT/AST with trunk/leg fat ratio in Japanese women.
Associations of LAR, a proxy of adipose tissue dysfunction, 28,37 with hepatic steatosis or NAFLD were reported in obese adolescents, 38 in Japanese adults who participated in a health survey 39 and in patients with lean NAFLD. 40 An association of LAR with ALT/AST in middle-aged Japanese women in this study may support an importance of adipose tissue dysfunction as an early key player in the development of NAFLD.
The strength of this study includes homogeneous study population with scarce confounding factors. 20 –22 Another strength is accurate and reliable measures of DXA-derived body composition. Several limitations of this study include the cross-sectional design, relatively small sample size, and a single measurement of biochemical variables. We used many surrogates in this study, which may be less accurate. Finally, as we studied Japanese women only, results may not be generalized to other sex, races, or ethnicities.
In conclusions, ALT/AST, a marker of hepatosteatosis, was associated with adipose IR and adipocyte dysfunction more closely than hepatic and muscle IR even in nondiabetic lean Japanese women. These findings suggest an importance of adipose IR as an early player in the development of hepatosteatosis.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Footnotes
Acknowledgments
The authors thank all participants for their dedicated and conscientious collaboration.
Authors' Contributions
S.M.-I., A.T.-K., M.H. and M.T. collected data and prepared tables. K.K., M.K. and B.W. analyzed data and prepared ![]() . T.K. wrote the article, and K.F. reviewed and edited it. All authors approved the final version of the article to be published. T.K. supervised the study, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
. T.K. wrote the article, and K.F. reviewed and edited it. All authors approved the final version of the article to be published. T.K. supervised the study, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Author Disclosure Statement
None of the authors have any potential conflicts of interest to declare associated with this research.
Funding Information
No funding was received for this article.