
Abstract
Objective:
It is well established that melanocortin-4 receptor (MC4R) rs17782313 locus polymorphism is associated with increased obesity risk and that obesity is strongly associated with an enhanced risk of all metabolic syndrome (MS) components. Thus, in this study, we examined the association between the MC4R rs17782313 locus polymorphism and the risk of the remaining MS components, namely, diabetes, hypertension, low high-density lipoprotein (HDL), and hypertriglyceridemia.
Methods:
We performed an extensive literature screening across six scientific databases, namely, PubMed, Embase, Web of Science, Medline, ScienceDirect, CNKI, and WanFang employing a specific search strategy. Eligible studies were selected for inclusion in our meta-analysis, and odds ratio (OR) values and 95% confidence interval (CI) were computed through fixed- or random-effects models to examine correlation strength. In addition, we performed subgroup analyses involving adjustment factors (unadjusted body mass index [BMI], adjusted BMI), race (Caucasian, Asian), and source of controls (population, hospital).
Results:
Twenty-two eligible studies were selected from 846 articles, involving 28,018 patients and 98,994 normal participants. Based on this meta-analysis, the MC4R rs17782313 locus polymorphism was associated with an augmented risk of diabetes (allele contrast model T vs. C: OR = 1.05, 95% CI = 1.03–1.08; dominant model TT vs. TC + CC: OR = 1.07, 95% CI = 1.03–1.11) and hypertension (dominant model TT vs. TC + CC: OR = 1.16, 95% CI = 1.03–1.31) risk. However, based on this analysis, the MC4R rs17782313 locus polymorphism was not associated with low HDL and hypertriglyceridemia risk.
Conclusions:
Based on this analysis, the MC4R rs17782313 locus polymorphism is associated with enhanced risks of diabetes and hypertension, while the associations with low HDL and hypertriglyceridemia require further exploration.
Introduction
Metabolic syndrome (MS) is characterized by a dysregulated metabolism, and it often manifests as overweight and obesity, hypertension, hyperglycemia, and dyslipidemia. 1 Recent investigations have confirmed a strong genetic role in the occurrence and development of the components of MS. Overweight and obesity induce hyperinsulinemia, activation of the renin–angiotensin–aldosterone system, stimulation of the sympathetic nervous system, abnormalities of adipokines such as leptin, atherosclerosis, and insulin resistance (IR), which can ultimately contribute to hyperlipidemia, hypertension, and diabetes. 2 –5 Therefore, obesity-related genes might be potential candidates for triggering diabetes, hypertension, and dyslipidemia.
The melanocortin-4 receptor (MC4R) is a hypothalamic G protein-coupled receptor, 6 and it is associated with nutrient absorption, lipid metabolism, energy expenditure, insulin secretion, food intake, and so on. 7 In 2008, based on a report by the Genome-Wide Association Study, the rs17782313 single nucleotide polymorphism (SNP) at 188 kb, downstream of the MC4R gene, is associated with the enhanced body mass index (BMI) and obesity risk. 8 In a previous meta-analysis, different model results showed an association between MC4R rs17782313 locus polymorphism and obesity (allele contrast model odds ratio [OR] = 1.325, 95% confidence interval (CI): 1.219–1.439; dominant model OR = 1.320, 95% CI: 1.184–1.472). 9 However, the results of correlation evaluations between MC4R rs17782313 and other MS components remain inconsistent. Sull et al. 10 and Hammad et al. 11 demonstrated that the MC4R rs17782313 locus polymorphism is markedly associated with an augmented risk of diabetes and hypertension. However, both Han et al. 12 and Szkup et al. 13 reported the opposite conclusion in their studies.
Therefore, in this study, we conducted an extensive review and meta-analysis of the association of MC4R rs17782313 locus polymorphism with diabetes, hypertension, and dyslipidemia, and assessed the risk for each MS component.
Methods
Literature search
We performed an extensive screening of scientific online databases, such as PubMed, Embase, Web of Science, Medline, ScienceDirect, CNKI, and WanFang, to search for articles published in English and Chinese on the association between MC4R rs17782313 locus polymorphism and the risk of MS components. We screened for articles from the establishment of each database until August 2, 2023.
The search strategy was as follows, diabetes: “MC4R rs17782313” OR “melanocortin 4 receptor rs17782313” AND “polymorphism” OR “variant” OR “genotype” AND “T2DM” OR “diabetes” OR “diabetes mellitus” OR “diabetic.” Hypertension: “MC4R rs17782313” OR “melanocortin 4 receptor rs17782313” AND “polymorphism” OR “variant” OR “genotype” AND “hypertension” OR “hypertensions” OR “hypertensive”. Low high-density lipoprotein (HDL): “MC4R rs17782313” OR “melanocortin 4 receptor rs17782313” AND “polymorphism” OR “variant” OR “genotype” AND “HDL-C” OR “high-density lipoprotein.” Hypertriglyceridemia: “MC4R rs17782313” OR “melanocortin 4 receptor rs17782313” AND “polymorphism” OR “variant” OR “genotype” AND “High triglyceridemia” OR “triglyceridemia” OR “TG” OR “triglyceride.”
In addition, we manually searched the references of the literature included in the meta-analysis to identify additional potentially eligible studies. When multiple studies used the same or overlapping datasets, the study with the larger sample size was selected. The present research was conducted, based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA statement). The protocol for the review was registered on the International Prospective Register of Systematic Reviews (PROSPERO) database under the number CRD42021292062.
Inclusion and exclusion criteria
Two authors separately reviewed the literature for study eligibility. Our inclusion criteria were as follows: (1) assessment of the MC4R rs17782313 locus polymorphism and its associated risk for each MS component; (2) provision of OR with 95% CI, under allele contrast model, dominant model, or availability of sufficient data to calculate OR; (3) the total number of subjects and cases were reported. The exclusion criteria were used as follows: (1) meta-analysis or review; (2) duplicate material; (3) animal research; and (4) missing relevant data.
Data extraction
We retrieved the following information from each selected article: (1) first author; (2) year of publication; (3) race; (4) source of controls; (5) number of cases and controls; (6) Hardy–Weinberg; (7) adjustment factors; (8) genotyping methods; (9) OR values and corresponding 95% CIs for the association strength of MC4R rs17782313 locus polymorphism with each MS component. Data were extracted separately by two authors, and any disagreements were settled through discussion.
Quality assessment of the studies
To assess study quality, two independent authors assessed each article according to the Newcastle–Ottawa Scale. Any disagreement was resolved through discussion. Ultimately, we included studies with scores of 6 and above. 9
Statistical analyses
All data analyses employed STATA software version 17.0 (StataCorp LP, College Station, TX, USA). In the case of multiple ORs in a single study, estimates of multivariate-adjusted risk were preferentially pooled. We employed meta-regression analysis, Cochrane's Q test, and I2 statistics to evaluate heterogeneity among studies. The heterogeneity source was analyzed through the random-effects model, and I2 > 50% and/or P value <0.05 was deemed significant. Otherwise, a fixed model was used. 14 The subgroup analyses of the MC4R rs17782313 locus polymorphism and diabetes-related data were performed based on the following characteristics: adjustment factors (unadjusted BMI, adjusted BMI), race (Caucasian, Asian), and source of controls (population, hospital). Our data stability was assessed based on a sensitivity analysis, which removed one study at a time. Lastly, funnel plots, as well as the Begg's and Egger's tests were employed to evaluate potential publication bias. 15 When the results from Begg's and Egger's tests contradict each other, the results from Egger's tests prevail. 16
Results
Characteristics and quality assessment of the eligible studies
Overall, 844 eligible articles were identified through screening of various databases, and 2 articles were obtained through other means. After screening, 22 qualified articles were selected for our meta-analysis, which were published between 2008 and 2020. The entire process of article selection is illustrated in Fig. 1. The study by Cauchi et al. 17 covered data from two different populations in Morocco and Tunisia. In the subsequent analysis of the data, these two groups were considered independent studies.
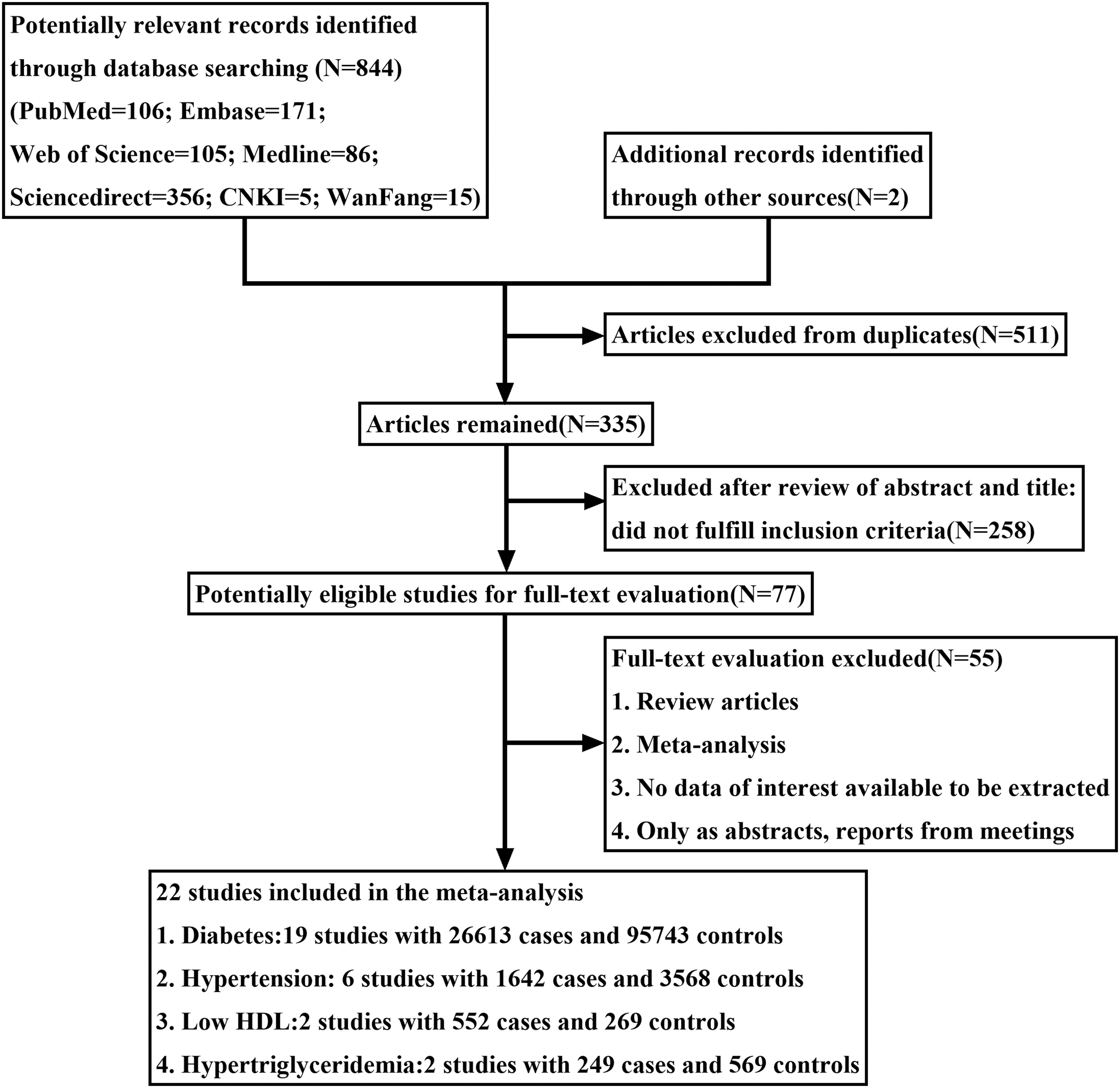
A schematic of the publication screening process. HDL, high-density lipoprotein.
In terms of race, 12 studies were conducted among Caucasians and 11 among Asians. The genotyping methods included TaqMan, MALDI-TOF-MS, sequences retrieval, iPLEX, MassARRAY technology, SNPlex™ technology, and OpenArray™ SNP Genotyping System. In terms of the source of control subjects, 12 studies included controls from the general population and 11 included controls from the hospital itself. All studies exhibited quality assessment scores of 6 and above, with a maximum score of 8. The characteristics of our eligible studies are summarized in Table 1.
Characteristics of the Eligible Studies
BMI, body mass index; HWE, Hardy–Weinberg equilibrium; Low HDL, low high-density lipoprotein; MALDI-TOF-MS, Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry; SNP, single nucleotide polymorphism.
Association between the MC4R rs17782313 locus polymorphism and the risk of diabetes
Based on fixed-effects model, the MC4R rs17782313 locus polymorphism was associated with diabetes risk (allele contrast model: OR = 1.05, 95% CI = 1.03–1.08, P < 0.001; dominant model: OR = 1.07, 95% CI = 1.03–1.11, P < 0.001). In terms of the sensitivity analysis, eliminating single studies did not significantly influence the pooled ORs (Fig. 2).
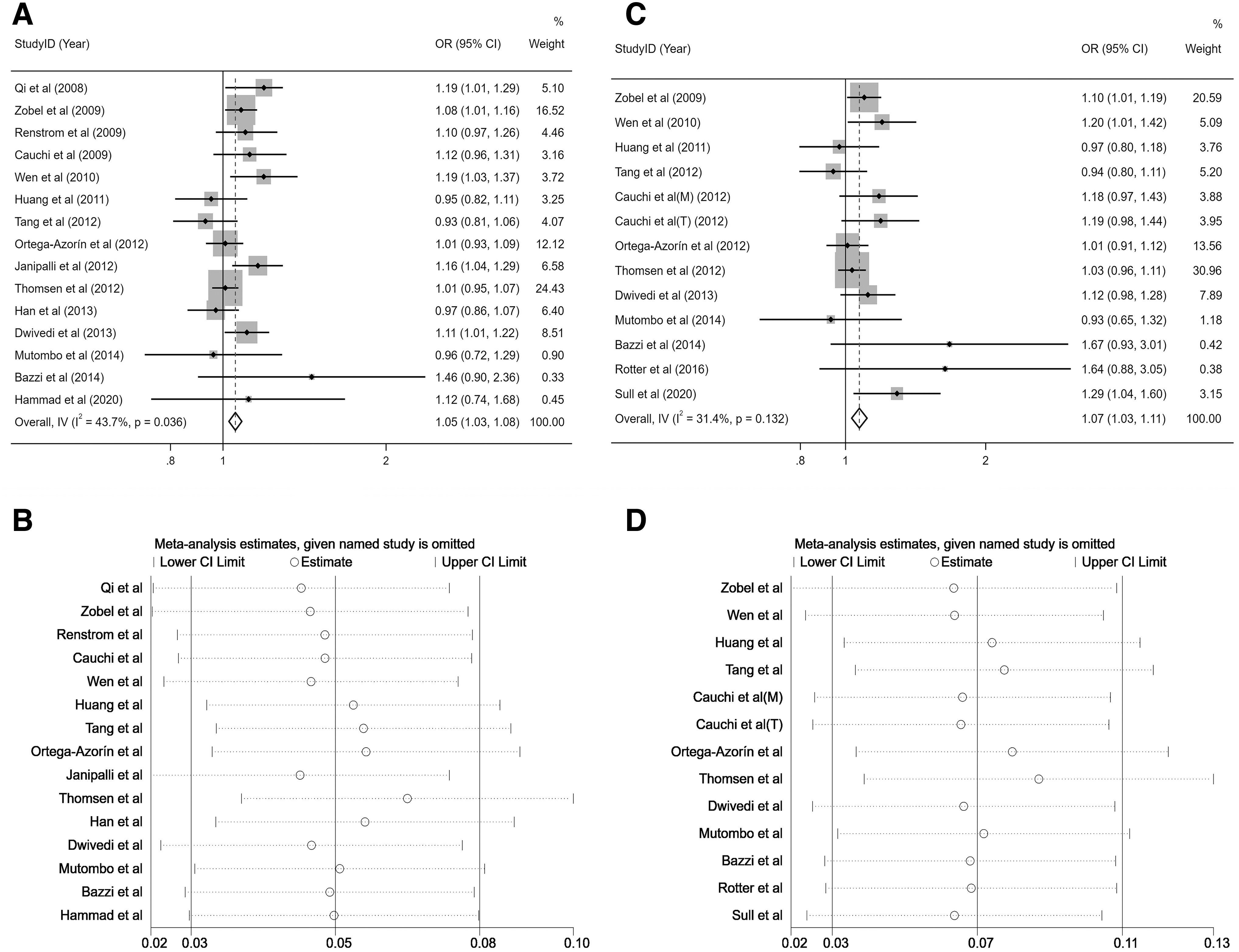
Forest plot and sensitivity analysis for MC4R variant rs17782313 and diabetes.
Based on the subgroup analyses, our results revealed that the overall OR for the allele contrast model was 1.05 (95% CI = 1.03–1.08). Upon further stratification analyses, the association persisted when grouped by adjustment factors, race, and source of controls (all P < 0.05). For the dominant model, the overall OR was 1.07 (95% CI = 1.03–1.11). Upon further stratification analyses, it was found that the MC4R rs17782313 locus polymorphism was associated with the risk of diabetes when unadjusted for BMI, but this association disappeared when adjusted for BMI. When controls originated from hospitals, the MC4R rs17782313 locus polymorphism was associated with diabetes risk, but this association disappeared when controls originated from the population. The specific data are summarized in Table 2.
Subgroup Analysis of the MC4R Variant rs17782313 and Diabetes
CI, confidence interval; OR, odds ratio.
Association between the MC4R rs17782313 locus polymorphism and the risk of hypertension
Based on fixed-effects model, the MC4R rs17782313 locus polymorphism was associated with hypertension risk (dominant model: OR = 1.16, 95% CI = 1.03–1.31, P = 0.014). In terms of the sensitivity analysis, eliminating single studies did not significantly influence the pooled ORs (Fig. 3).
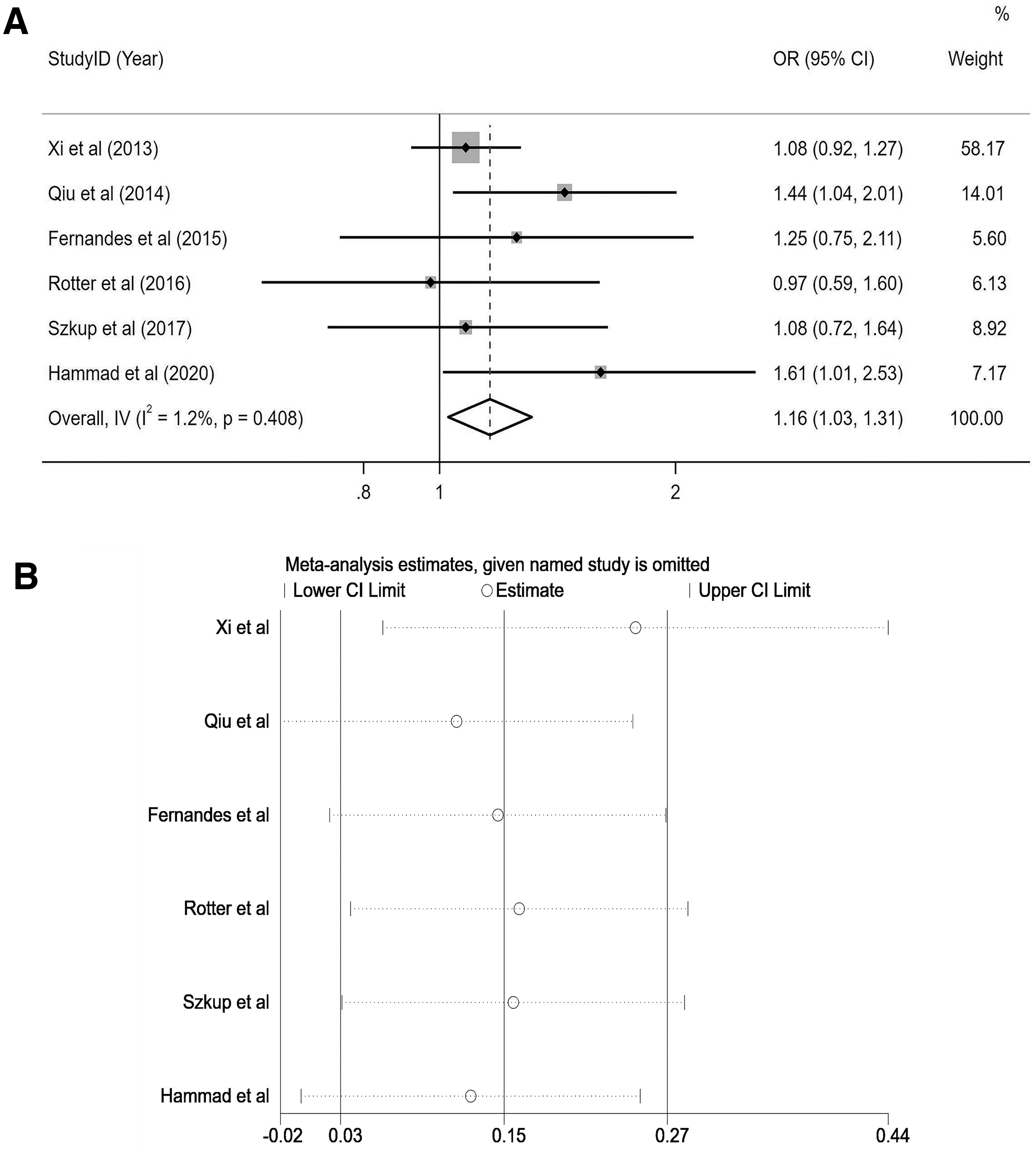
Forest plot and sensitivity analysis of the relationship between the MC4R variant rs17782313 and hypertension.
Association between the MC4R rs17782313 locus polymorphism and the risk of low HDL
Based on fixed-effects model, the MC4R rs17782313 locus polymorphism was not associated with low HDL risk (dominant model: OR = 0.95, 95% CI = 0.70–1.29, P = 0.757) (Supplemetnary Fig. S1).
Association between the MC4R rs17782313 locus polymorphism and the risk of hypertriglyceridemia
Based on random-effects model, the MC4R rs17782313 locus polymorphism was not associated with hypertriglyceridemia risk (dominant model: OR = 1.53, 95% CI = 0.91–2.57, P = 0.107) (Supplementary Fig. S2).
Evaluation of heterogeneity, publication bias
The meta-regression analysis indicated that the P values were all >0.05, and the differences were not statistically significant (Table 3). Our initial observations through funnel plots (Fig. 4) showed a symmetrical distribution within the region, which enhanced the confidence in our results. The Begg's and Egger's tests were employed for the purpose of examining publication bias. The results suggested no publication bias in terms of the association between the MC4R variant rs17782313 and diabetes (allele contrast model: Egger's test: P = 0.357, Begg's test: P = 0.621; dominant model Egger's test: P = 0.101, Begg's test: P = 0.044) and hypertension (Egger's test: P = 0.378, Begg's test: P = 0.707).

The funnel plots of the relationship between the MC4R variant rs17782313 and diabetes and hypertension risks.
The Meta-Regression Analysis of the Association Between the MC4R Variant rs17782313 and Diabetes Risk
Discussion
With the rapid rise in MS incidences worldwide, it is now a global disease that seriously affects human health, particularly, due to its association with cardiovascular disease. Early studies revealed that MS is associated with a 2-fold increase in the risk of cardiovascular disease, cardiovascular disease mortality, myocardial infarction, and stroke, as well as a 1.5-fold increase in all-cause mortality. 33 Due to the complexity of its pathogenesis, MS has been the focus of numerous scientific reports over the past few years. Factors, such as IR constitute the main pathophysiological pillar of MS pathogenesis, 34 and any 3 of its components may manifest as IR. 35 Among them, obesity is one of the typical diseases that plays an important role in MS prevalence, 36 and it is closely related to other components.
Much research has recently focused on genetic obesity, with the association between the MC4R gene and obesity prevalence being one of the most common cases. 37 MC4R is ubiquitously expressed in the hypothalamus, 38 and it is involved in the modulation of food selection, food intake, and energy expenditure. One study indicated that 44% of the variance in meal frequency and 65% of the variance in meal size is genetically determined. 39 MC4R gene mutations often diminish the ability of MC4R to interact with the α-melanocyte-stimulating hormone or/and agouti-related peptide, which can have detrimental energy intake outcomes. 40 The C allele carrying MC4R rs17782313 is correlated with uncontrolled eating, elevated energy intake, and binge eating behavior in adults, 41,42 which, in turn, contributes to obesity and other related diseases. 10 In addition, a study showed that the polymorphism of rs17782313 is associated with MS prevalence in postmenopausal women. 43 However, the association between MC4R rs17782313 locus polymorphism and other MS components remains unclear and controversial.
This study found that the MC4R rs17782313 locus polymorphism was associated with enhanced diabetes risk. Further subgroup analysis showed that in the allele contrast model, there was a marked association between the MC4R rs17782313 locus polymorphism and diabetes in all groups. In the dominant model, the MC4R rs17782313 locus polymorphism was found to be associated with the risk of diabetes when unadjusted for BMI, but this association disappeared after adjustment for BMI. This may imply that the association of the MC4R rs17782313 locus polymorphism with diabetes risk is actually realized through its influence on BMI. 19 It may also be because the relevant literature is more limited, containing only 2 articles involving BMI adjustment, and the statistical efficacy is insufficient, and further studies are needed to complement it.
When the source of the control group was different (hospitals or populations), the findings showed differences, so further research is needed to validate this association by considering the effects of factors such as study design, sample size, and setting. 44 There are significant differences in the prevalence of diabetes across geographic regions and races. In the United States, for example, the prevalence of diabetes is higher among people of African descent, at 14%, compared with 9% among the white population of European ancestry. 45 Despite different genetic backgrounds among the Caucasian and Asian populations, we observed no heterogeneity within the overall population. Moreover, we demonstrated associations between the MC4R rs17782313 locus polymorphism and diabetes risk, with effect sizes comparable between the Caucasian and Asian populations.
The MC4R gene may cause diabetes through obesity. Numerous studies suggested that obesity increases diabetes risk. 46 Obese patients often exhibit increased plasma renin activity and plasma angiotensin II concentrations, as well as augmented catecholamine-induced lipolysis. The resulting rise in serum-free fatty acid levels can, in turn, enhance the risk of developing type 2 diabetes mellitus (T2DM). 47 In addition, MC4R modulates glucose metabolism through sympathetic nerve regulation. 48 Some studies suggested that the correlations between the MC4R rs17782313 polymorphisms and T2DM and obesity are partially dependent on dietary intake. This indicates that both T2DM and obesity have a common genetic etiology. 25 Finally, Chambers et al. 49 demonstrated that MC4R polymorphisms are also correlated with IR, which is a major pathophysiological factor that leads to diabetes.
In this study, the MC4R rs17782313 locus polymorphism was associated with an increased risk of hypertension. Studies show that 60%–70% of primary hypertension is attributed to obesity and the prevalence of hypertension increases by 20%–30% as the weight increases by 5%. 50 The MC4R gene may indirectly cause hypertension through an obesity-related pathway. Obese conditions generally reduce levels of vasodilators, such as lipocalin and nitric oxide, while increasing vasoconstrictors such as resistin and endolipin. This, in turn, induces a rise in blood pressure. 47 Greenfield et al. 51 used both genetic and pharmacological investigations to demonstrate that MC4R is associated with hypertension. They revealed that MC4R modulates hypertension development through a central melanocortin signaling pathway, an effect achieved independent of obesity-induced hyperinsulinemia.
In addition, the product of the MC4R gene, melanocortin receptor-4, exerts bidirectional regulation of the sympathetic and parasympathetic preganglionic neurons, which, in turn, affects alterations in insulin levels and blood pressure. 52 Lastly, the rs17782313 locus has the potential to indirectly promote hypertension by accelerating atherosclerosis and vascular remodeling through changes in serum total cholesterol. 2
In this study, the MC4R rs17782313 locus polymorphism was not associated with the risk of low HDL and hypertriglyceridemia. On the contrary, the research of Fernandes et al. 7 found that the MC4R rs17782313 locus polymorphism was associated with hypertriglyceridemia risk. Therefore, more high-quality studies are needed to verify this association.
We encountered the following limitations in this article. First, our study searched restricted databases, and there may exist articles that meet our inclusion criteria, which were not included. Second, in terms of obtaining multivariate-adjusted ORs where possible, some ORs were acquired without adjustment, which may potentially affect the accuracy of our results. Third, the impact of intergenic and gene–environment interactions on the accuracy of the current results was not evaluated in our study.
In summary, this meta-analysis supports the association between the MC4R rs17782313 polymorphism and diabetes and hypertension risk within the study population. Individuals with the MC4R rs17782313 TC/CC genotype were more susceptible to diabetes and hypertension. In contrast, associations with hypertriglyceridemia and low HDL risk remained unknown, and require more high-quality studies to confirm the relationship. Further research is recommended to clarify the association and potential mechanism between the MC4R rs17782313 locus polymorphism and MS components.
Footnotes
Authors' Contributions
H.Y.: Conceptualization, data curation, formal analysis, investigation, methodology, software, validation, writing––original draft, and writing––review and editing. Q.H.: Conceptualization, data curation, formal analysis, investigation, methodology, validation, and writing––review and editing. H.Y.: Methodology, investigation, and validation. Z.Q.: Conceptualization, validation, and writing––review and editing. All authors contributed to the study design and article preparation.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This work was supported by the National Natural Science Foundation of China (Grant No. 81660562).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.