
Abstract
Background:
Despite recent evidence of remaining possibility that early initiation of xanthine oxidase inhibitors (XOIs) is beneficial in renoprognosis for patients with stage 2 or less chronic kidney disease (CKD), no evidence is available regarding the difference in renoprognosis based on serum uric acid (sUA) levels at the initiation of XOIs among patients with preserved kidney function.
Methods:
New XOI initiators were divided into quartiles based on baseline sUA. Primary outcome was the composite incidence of a significant estimated glomerular filtration rate (eGFR) decline (≥40% decline in eGFR from baseline or development of eGFR <30 mL/1.73 m2/min) or all-cause death within 5 years.
Results:
After excluding inapplicable patients, 1170 XOI initiators were analyzed (mean ± standard deviation age: 68 ± 14.3 years; sUA: 10.6 ± 1.15 mg/dL). On overall median [interquartile range (IQR)] follow-up of 824 (342, 1576) days, incidence rate of the primary outcome was 287 per 1000 person-years for 5 years. Although the nonadjusted model showed a dose–response association between baseline sUA level and the outcome, the adjusted model showed no significant association. Adjusted hazard ratios (95% confidence interval) of the second, third, and fourth quartiles of baseline sUA with the composite outcome within 5 years compared to the first quartile were 1.00 (0.78, 1.29), 1.00 (0.80, 1.30), and 1.02 (0.80, 1.32), respectively.
Conclusions:
Early initiation of XOIs did not predict a significant benefit on renoprognosis even among the population with preserved kidney function. The validity of initiating XOIs with the aim of improving renoprognosis based on sUA is questionable.
Introduction
C
Many previous studies revealed a significant association between hyperuricemia and CKD progression, 5,6 and some countries, including Japan, have long considered that early initiation of uric acid lowering treatment (ULT) slows CKD progression and reduces the risk of incidence of new-onset CKD. 7 In Japan, serum uric acid (sUA) levels >9 and >8 mg/dL in patients with co-morbidities are still widely treated using xanthine oxidase inhibitors (XOIs) regardless of a history of gout and kidney function, in compliance with the guideline published by Japanese Society of Gout and Uric & Nucleic Acids. 8
However, more recent evidence has narrowed the potential indications for ULT in treating asymptomatic hyperuricemia. Several recent large randomized control trials (RCTs) found no significant benefit of ULT using XOIs in reducing estimated glomerular filtration rate (eGFR) decline among patients with stage 3 and 4 CKD, 9,10 or in patients with Type 1 diabetes. 11 Thus, some experts now accordingly argue that XOIs for hyperuricemia might be beneficial in renoprognosis only among patients with preserved kidney function. 9,10,12 To date, however, no study has investigated the benefit or otherwise of early initiation of XOIs based on sUA level in renoprognosis in patients with preserved kidney function, for whom ULT is still expected to be beneficial.
In this study, we longitudinally investigated the association between sUA level at the initiation of XOIs and eGFR progression among the patients with preserved kidney function for 3 and 5 years.
Methods
Study design and setting
This new-user, longitudinal study used the Real-World Data Database from July 2002 to May 2022. As of 2022, this database held the health records of ∼26 million patients from 229 medical institutions across Japan. The database was provided by the Health, Clinic and Education Information Evaluation Institute (Kyoto, Japan), and data collection and management were supported by Real World Data Co., Ltd. (Kyoto, Japan). The data were collected automatically from out- and in-patients' electronic health records, claims data, and hospital administrative data: Diagnosis Procedure Combination/Per-Diem Payment System (DPC/PDPS). 13 The data contain information on demographics, diagnoses, prescriptions, procedures, and laboratory data. Individual patients can be tracked as long as they are treated in the same facility. This study was approved by the Ethics Committee of Kyoto University Graduate School and Faculty of Medicine (approval No. R3494) and was conducted in accordance with ethical guidelines in Japan.
Participants
We selected patients aged 18 to 99 years who initiated allopurinol, febuxostat, or topiroxostat for hyperuricemia or gout before developing stage 3 CKD from July 2002 to May 2022 and having more than 180 days of continuous enrollment in the database. We selected patients who had eGFR ≥60 mL/min/1.73 m2 and sUA ≥8 or ≤16 mg/dL, in the nearest neighbor value of the index date within180 days before the index date. This is because a guideline published by Japanese Society of Gout and Uric & Nucleic Acids recommends that medication therapy for hyperuricemia be started from sUA ≥8 mg/dL in patients with hypertension, diabetes, metabolic syndrome, or renal dysfunction regardless of symptoms of gout. We excluded patients with sUA >16 mg/dL on the basis that such levels, more than double the therapeutic threshold, are extremely high and that these patients may accordingly have a genetic disease, such as familial juvenile hyperuricemic nephropathy, Lesch-Nyhan syndrome, von Gierke disease, phosphoribosylpyrophosphate synthetase superactivity, and phosphofructokinase deficiency. The underlying association between these diseases and sUA may qualitatively differ.
Furthermore, we excluded patients with concomitant use of other uric acid-lowering drugs (UALDs) within 180 days before and at the index date, as well as those with poor renoprognotic conditions, such as urinary protein at presentation, or concomitant renal, liver, cardiovascular, or cerebrovascular disease, or malignancy. Baseline data were defined as the nearest neighbor value from the index date within 180 days. Inclusion and exclusion criteria are described in detail in Supplementary Table S1 and Supplementary Fig. S1.
Exposures
The exposure of interest was sUA level at the initiation of XOIs. The data were defined as the nearest neighbor value from the index date within 180 days. All data were extracted from out- and in-patients' electronic health records and were uniformly standardized by the distributor independent from the researchers.
Outcomes
The primary outcome was a composite incidence of a significant decline in eGFR or all-cause death in 3 and 5 years. eGFR was calculated by the following formula, which was developed and fully validated for the Japanese population.
14
A significant eGFR decline was defined by a renal composite outcome of ≥40% decline in eGFR from baseline and sustained for at least two consecutive measures, or the development of eGFR <30 mL/1.73 m2/min. 15,16 As secondary and tertiary outcomes, we divided the primary outcome into renal composite outcomes and all-cause death, respectively. Outcome variables are defined in detail in Supplementary Table S2 and Supplementary Fig. S1.
Patient follow-up
We designated a follow-up period of 3 and 5 years from XOI initiation to evaluate the long-term association of baseline sUA at the time of UALD initiation. 17 –19 We observed the patients until the occurrence of a study outcome, treatment discontinuation, change of hospital, or end of the study period, whichever occurred first. We defined treatment discontinuation as no further prescription within a 365-day grace period after the final day of the preceding prescription. For patients who switched to another XOI, we maintained observation for the occurrence of events as long as the patient was not censored.
Covariates
Based on previous studies and expert opinion, we identified the following variables as potential confounders or well-known risk factors. We adjusted for sex, age, body mass index (BMI), 20,21 smoking habit as measured by the Brinkman index (BI), 22,23 baseline eGFR, type of initiated XOI, 24 –26 previous diagnosis of gout, diabetes, diabetic retinopathy, hypertension, dyslipidemia, use of angiotensin converting enzyme inhibitors (ACEIs), 27 and calendar year of the index date. In addition, we adjusted the all-available number of eGFR measurements before the index date to minimize bias due to a lack of examination follow-up. To improve the validity of disease diagnosis, the diseases mentioned above were defined using a combination of the International Classification of Diseases, Tenth Revision (ICD-10) code and prescription dispensing coded according to the Anatomical Therapeutic Chemical (ATC) classification system and procedure codes, as far as possible. Definitions, codes, and time window for assessment regarding covariates are shown in Supplementary Table S3 and Supplementary Fig. S1.
Statistical analysis
Patients were divided into four groups using the quartile value of baseline sUA, with the first quartile group defined as reference. Patient characteristics are expressed as medians with interquartile ranges (IQRs) for continuous variables and number with percentages for categorical variables. Time-to-event curves were described using Kaplan–Meier plots. To minimize selection bias due to missing data, we conducted 10 sets of multiple imputations with chained equations for missing data of covariates (BMI and BI) using the other nonmissing variables. 28 Cox proportional hazard models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) for predictive association between baseline sUA and composite incidence of a significant eGFR decline or all-cause death as primary analysis. We separately calculated the cause-specific HRs for significant eGFR decline and all-cause death using the same set of covariates.
To visualize the potentially nonlinear association between baseline sUA and each outcome, we used restricted cubic splines using 4 knots at prespecified locations according to percentiles of the distribution of baseline sUA, with the 5th, 25th, 75th, and 95% percentiles 29 as secondary analysis. For tertiary analysis, we also drew the trajectory of eGFR progression for each group using restricted cubic splines with four knots at prespecified locations of the distribution of eGFR. Each individual's repeated eGFR data, including after the occurrence of outcome events, were used for the modeling, and within-person correlations were treated as clusters. The nonlinear regression models mentioned above were modeled based on the Akaike Information Criteria 29 and adjusted using the same set of covariates as in the primary analysis.
Sensitivity analysis
To confirm the robustness of the primary analysis's results, we conducted four sensitivity analyses. First, to assess the impact of outcome misclassification, we reperformed the primary analysis without censoring for drug discontinuation. We maintained observation for the occurrence of events for patients who stopped using the index drug or who switched to other XOIs. This is called initial-treatment approach, which is similar to intention-to-treat approach. 30 Second, to assess selection bias due to missing data, we reconducted the primary analysis in the complete case analysis. Third and fourth, to assess the influence of the upper limit of the arbitrary cutoff range of sUA, we reconducted the primary analysis after changing the upper limit of the baseline sUA range from 16 to 18 mg/dL and to 20 mg/dL. All analyses were performed with R, version 4.2.2 31 and STATA version 17.1 (Stata Corp, College Station, TX).
Results
Participant characteristics
Figure 1 presents the flow of patient selection. After applying the inclusion and exclusion criteria, 1170 XOI initiators were analyzed. Table 1 shows patient characteristics by baseline sUA quartiles (n = 292 or 293). Median (IQRs) age of all patients was 71 years (59, 80), and 29% were female (335/1170). The median and (minimum–maximum) sUA of the overall population was 10 mg/dL (8–16), and the minimum–maximums of each quartile group were 8–10, 10–10, 10–11, and 11–16 mg/dL, respectively. The higher sUA quartile groups were slightly older, contained slightly more females, included fewer missing values, and had more frequent eGFR measurement. Types of drugs were distributed roughly equally across quartiles. Overall median (IQRs) follow-up for outcomes was 824 (343, 1576) days. Median (IQRs) days of follow-up of the first, second, third, and fourth quartiles of baseline sUA were 875 (358, 1552), 950 (371, 1581), 785 (342, 1614), and 706 days (267, 1574) days, respectively.
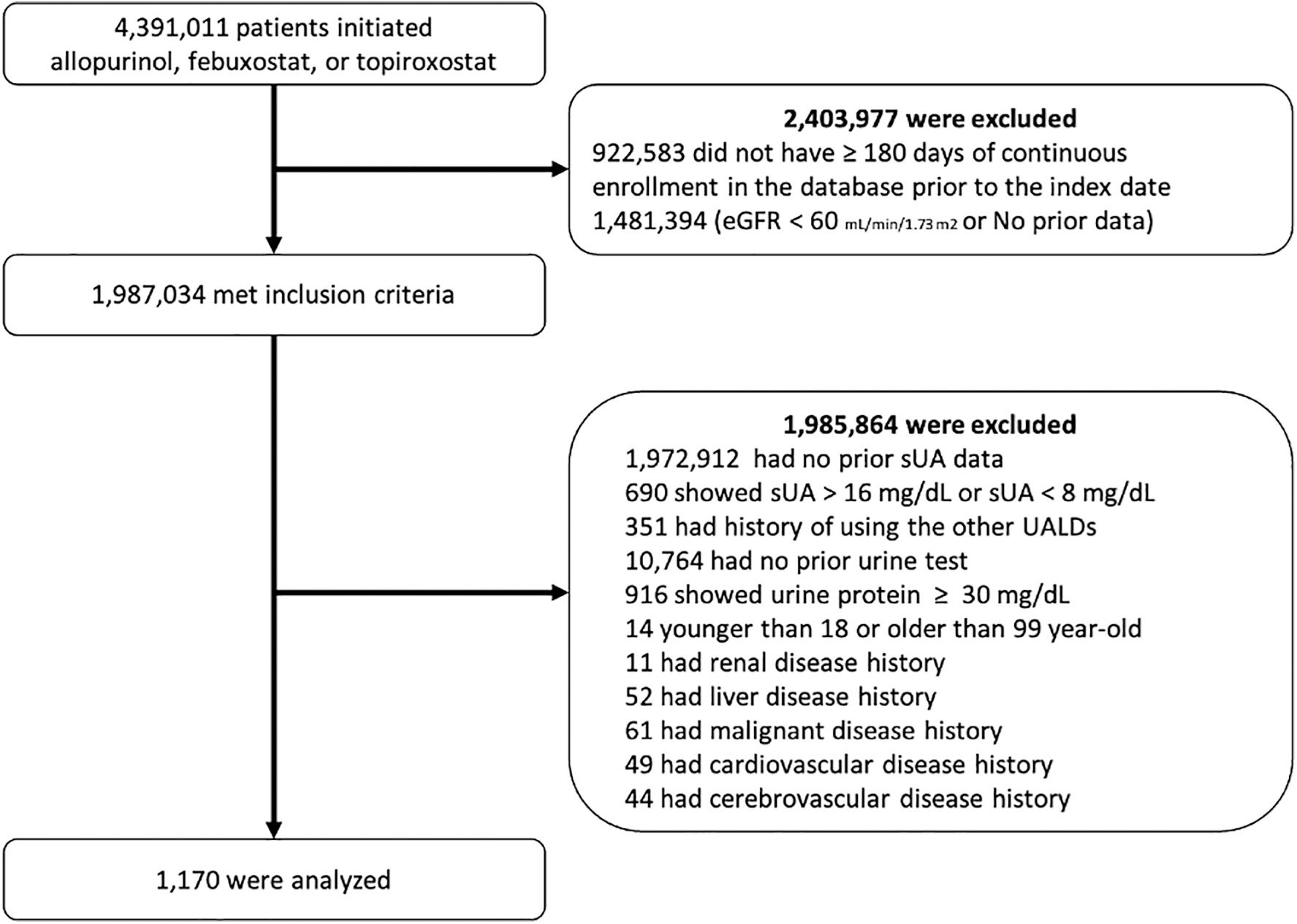
Study flow diagram. eGFR, estimated glomerular filtration rate; sUA, serum uric acid; UALDs, uric acid-lowering drugs.
Patient Characteristics and Incidence of Outcomes
[Minimum–maximum]; n (%); median [25%, 75%]. Decline means >40% decline from baseline or <30 mL/min/1.73 m2 in eGFR.
ACEI, angiotensin converting enzyme inhibitor; BI, Brinkman index; BMI, body mass index; eGFR, estimated glomerular filtration rate; sUA, serum uric acid; XOIs, xanthine oxidase inhibitors.
Outcome data
During the observation period, the overall incidence rate for the composite incidence of a significant eGFR decline or all-cause death was 321 per 1000 person-year (499/1170, 43%) for 3 years and 287 per 1000 person-year (529/1170, 45%) for 5 years. The Q1–Q4 incidence rate for the composite incidence were 296, 367, 434, and 485 per 1000 person-years for 3 years and 265, 323, 395, and 435 per 1000 person-years for 5 years, respectively.
Association of baseline sUA with incidence of composite outcomes and significant eGFR decline
The Kaplan–Meier plot in Supplementary Fig. S2 illustrates the event-free probability of the composite outcome and significant eGFR decline in 3 and 5 years by quartile of baseline sUA. Plots for the Q1 (reference) group showed a constantly high event-free proportion and did not cross the other quartile groups' plot during the observation period.
The results of primary analysis are summarized in Fig. 2. Although nonadjusted Cox models showed a dose–response association between baseline sUA and the composite outcome, the adjusted model did not show any significant association. Adjusted HRs (95% CIs) for second, third, and fourth quartiles of baseline sUA for the composite outcome (incidence of a significant eGFR decline or all-cause death) within 3 years compared to the first quartile were 1.00 (0.77, 1.30), 1.01 (0.78, 1.31), and 1.03 (0.79, 1.33) and within 5 years were 1.00 (0.78, 1.29), 1.00 (0.80, 1.30), and 1.02 (0.80, 1.32), respectively. The adjusted HRs (95% CIs) of the second, third, and fourth quartiles of sUA for incidence of a significant eGFR decline within 3 years compared to the first quartile were 1.07 (0.80, 1.43), 1.07 (0.80, 1.43), and 0.96 (0.72, 1.29) and within 5 years were 1.04 (0.78, 1.39), 1.07 (0.81, 1.43), and 0.98 (0.74, 1.30), respectively.
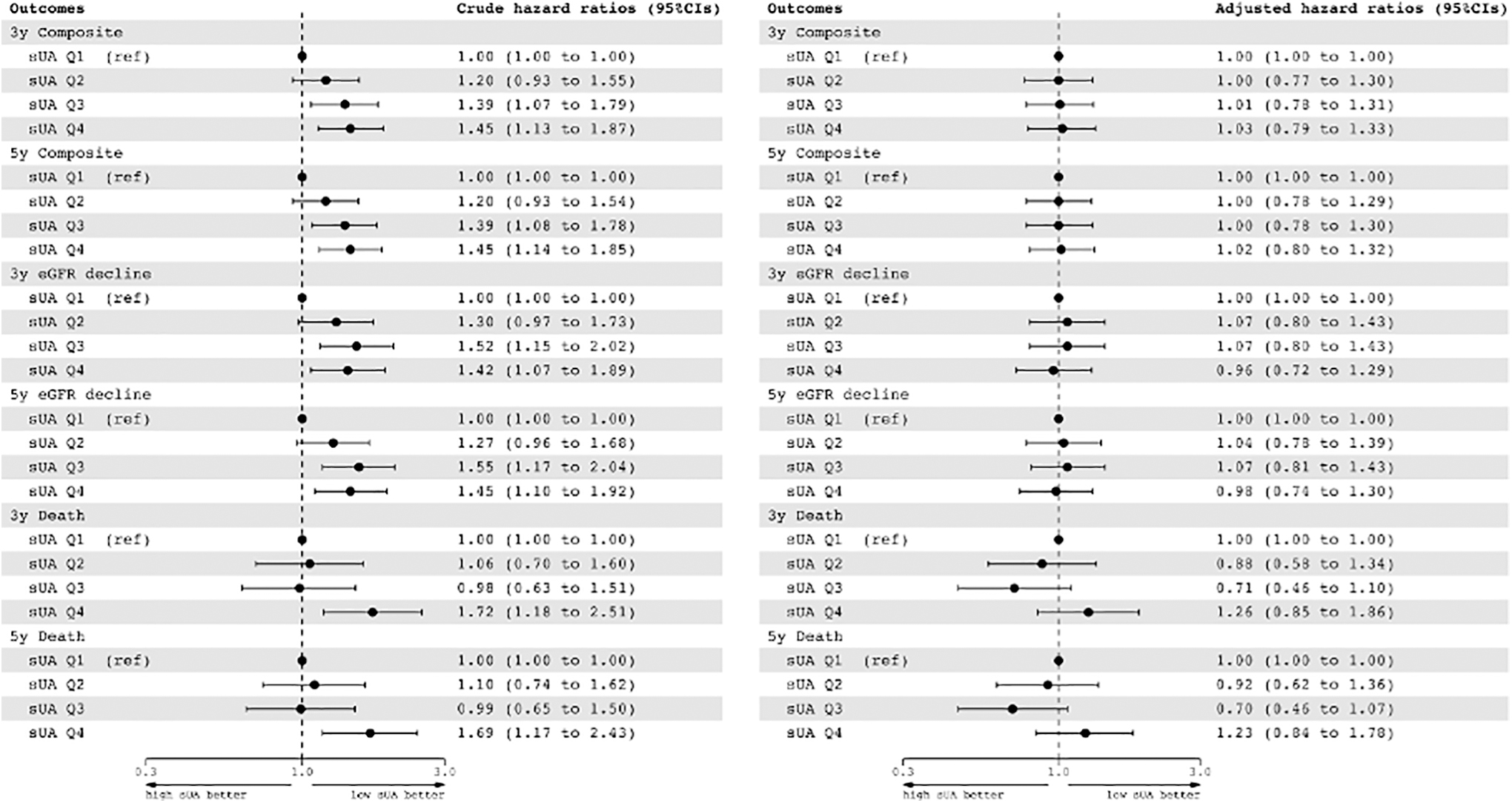
Association of baseline sUA with incidence of a significant eGFR decline or/and all-cause death. “Composite” means incidence of “eGFR decline” or all-cause death; “eGFR decline” means composite incidence of ≥40% decline in eGFR from the baseline sustained for at least two consecutive measures or development of eGFR <30 mL/1.73 m2/min. Cox proportional hazard models were used to calculate HRs and 95% CIs. The models were adjusted for sex, age, body mass index, Brinkman index, baseline eGFR, type of initiated XOIs, previous diagnosis of gout, diabetes, diabetic retinopathy, hypertension, dyslipidemia, use of angiotensin converting enzyme inhibitors, calendar year of cohort entry, and total number of eGFR measurements. 95% CI, 95% confidence interval; HR, hazard ratio; Q, quartile; XOI, xanthine oxidase inhibitor; y, years.
Supplementary Figure S3 and Fig. 3 describe the continuous association between baseline sUA and the composite outcome and a significant eGFR decline in the 3- and 5-year observation periods, respectively. In both periods, the nonadjusted model showed that relative hazard for both outcomes increased with increasing baseline sUA level. After adjustment, in contrast, the association line became flat. For sUA levels from 8 to 11 mg/dL, the association was along the null line for both the 3- and 5-year periods. Furthermore, even though the line slightly increased with sUA more than 12 mg/dL, the CIs included the null line throughout the observed sUA range.
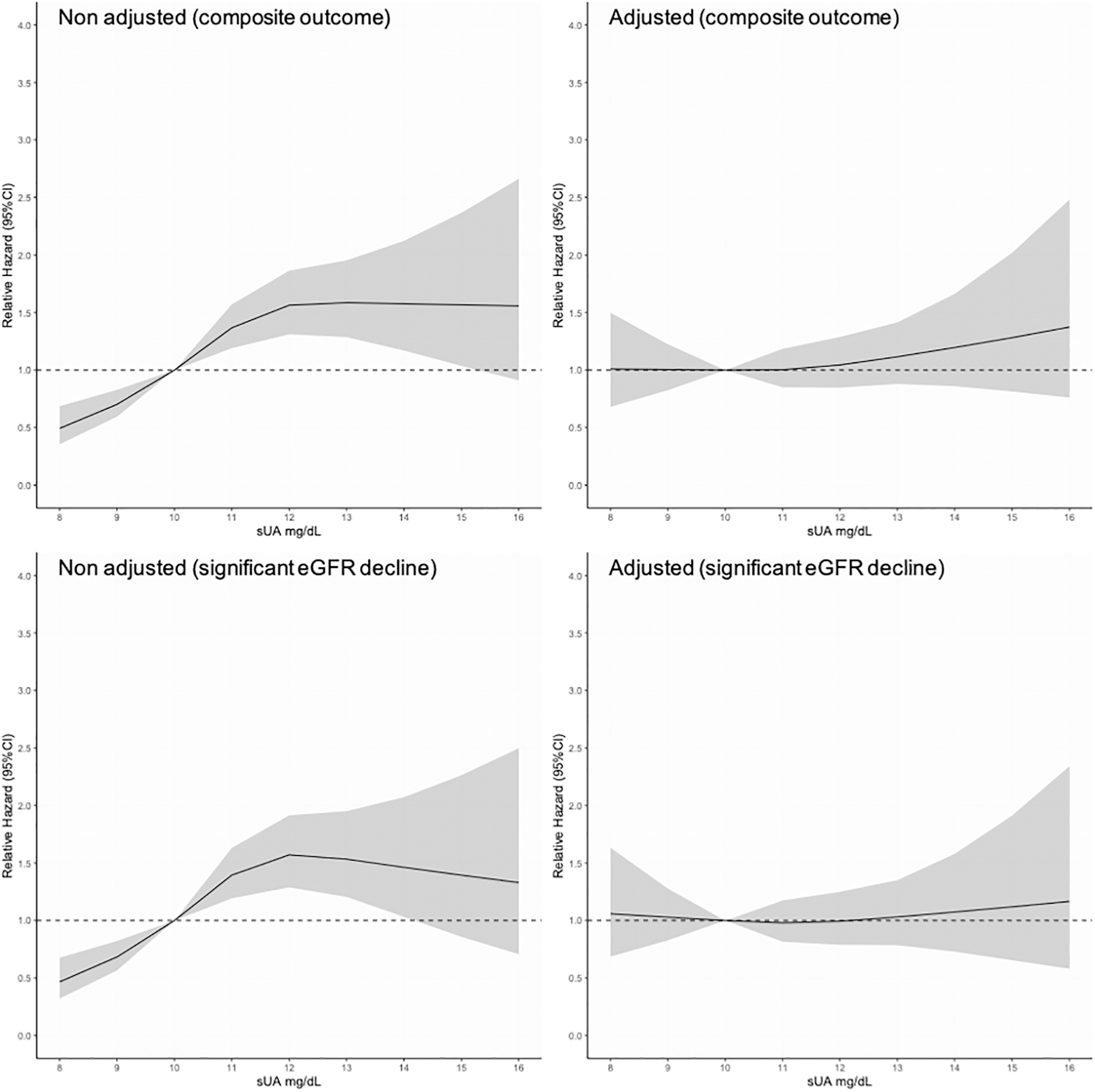
Continuous association of baseline sUA with composite outcome and significant eGFR decline in 5 years (nonadjusted/adjusted model). Composite outcome means incidence of significant eGFR decline or all-cause death; significant eGFR decline means composite incidence of ≥40% decline in eGFR from baseline sustained for at least two consecutive measures or development of eGFR <30 mL/1.73 m2/min. Cox proportional hazard models were used to calculate HRs and 95% CIs. The models were adjusted for sex, age, body mass index, Brinkman index, baseline eGFR, type of initiated XOI, previous diagnosis of gout, diabetes, diabetic retinopathy, hypertension, dyslipidemia, use of angiotensin converting enzyme inhibitors, calendar year of cohort entry, and total number of eGFR measurements.
Figure 4 depicts the longitudinal trajectory of eGFR progression for each quartile group. The nonadjusted model showed a more rapid decline in eGFR with a higher baseline sUA level. However, the adjusted model shows a diminution in the difference in eGFR between groups and a reversal of the relationship between eGFR progression speed and baseline sUA level.

Longitudinal trajectory of eGFR progression by quartile of baseline sUA. The gray-shade area represents the 95% CI; the models were adjusted for sex, age, body mass index, Brinkman index, baseline eGFR, type of initiated XOI, previous diagnosis of gout, diabetes, diabetic retinopathy, hypertension, dyslipidemia, use of angiotensin converting enzyme inhibitors, calendar year of cohort entry, and total number of eGFR measurements.
Sensitivity analysis
Supplementary Figures S4–S7 summarize the results of the four sensitivity analyses. Results were similar to those of the primary analysis for all, confirming the robustness of the findings.
Discussion
Although early initiation of XOIs has been expected to improve renoprognosis among patients with eGFR within a reference range and without proteinuria, we consistently found no significant differences between baseline eGFR level on renoprognosis among patients in this population-based cohort study using real world data. Furthermore, the longitudinal trajectory of eGFR progression also showed no significant difference between baseline eGFR level after adjusting for covariates.
In this study, we specifically investigated the difference in renoprognosis by baseline sUA at the initiation of hyperuricemia treatment among patients with preserved kidney function, in whom this treatment is expected to be beneficial. Similar results were reported by a previous study that analyzed the continuous association between baseline sUA and a composite of initiation of chronic dialysis or pre-emptive transplantation among patients with CKD stage 3 or higher. 32 After adjustment for a similar set of covariates to those in our study, their nonlinear graph of the association also showed a flat line, which strongly supports the reproducibility of our results.
Furthermore, the several large RCTs mentioned above denied a significant benefit of XOIs on renoprognosis among stage 3 and 4 CKD patients. 9,10 In this study, therefore, we focused on patients with reference range eGFR and without proteinuria. Since clinicians in Japan have commonly prescribed XOIs for patients with hyperuricemia regardless of a history of gout and a stage of kidney function, our database contains patients who started XOIs at various levels of sUA and kidney function. This unique characteristic of our data allowed us to investigate the clinical effectiveness of early initiation of XOI based on sUA level on renoprognosis.
Given that sUA levels increase with age 33 and that higher sUA is associated with CKD progression, 34,35 early initiation of ULT based on the sUA level was apparently reasonable when the lowering therapy directly improved renoprognosis. Despite this, the applicability of ULT in improving renoprognosis is now limited or even controversial. Several systematic reviews (SRs) have reached various conclusions. For instance, a Cochran review of 12 RCTs concluded that ULT conferred no benefit on progression of kidney function. 36 A more recent SR of the impact of ULT on composite renal events (deterioration of renal function, end-stage renal disease, and initiation of renal replacement therapy; but excluding the development of isolated albuminuria) among patients with asymptomatic hyperuricemia suggested that allopurinol and febuxostat reduce the incidence of composite renal events. 37 However, neither of these reviews included the recent large and well-designed RCTs that found no benefit of XOI in delaying the progression of eGFR decline. 9,11
Thus, considering this most current evidence, our results underscore the low validity of early initiation of XOIs based on sUA, at least with regard to the goal of reducing the decline in eGFR among patients with preserved kidney function.
Although ULT has been expected to improve kidney function, some researchers suggest the opposite possibility. Many experimental studies have indicated a mechanism in which high sUA impairs endothelial function through a reduction in nitric oxide production which potentially accelerates CKD progression. 38 However, a recent animal study denied the idea that CKD progression is driven solely by hyperuricemia. 39 Furthermore, contrary to the expected benefit of ULT, a study that focused on patients with preserved kidney function—precisely the same population we focused on in this study—raised the possibility that ULT could accelerate CKD progression. 40 Moreover, subgroup analysis in that study revealed a negative impact of ULT on CKD progression in patients with sUA levels of 8 mg/dL or less, but not in those with levels >8 mg/dL. These results may be partially concordant with our results in Fig. 3 and Supplementary Fig. S3, namely that the risk of significant eGFR decline was slightly increased when sUA level was 8 mg/dL compared to a reference level of 10 mg/dL, even though the difference was not statistically significant.
Given these findings, clinicians should take a more cautious approach to the proper indications for XOIs, especially for patients with only asymptomatic hyperuricemia.
Our study has several limitations. First, this study did not observe non-XOI users. Thus, the effect of XOIs on renoprognosis compared to non-XOI users could not be deduced from our study. However, we constructed this study design focusing on the difference of renoprognosis based on sUA level at the beginning of XOIs to avoid involved indication bias between users and nonusers. Second, mainly due to a lack of laboratory data, a relatively large population was excluded from the target population. This selection procedure may have limited the external validity of our findings. Patient selection was, however, highly important to confirming the internal validity of the comparison. Furthermore, since clinicians tend to order laboratory tests more frequently for patients with advanced conditions, the lack of laboratory tests among patients with a mild condition would not dilute our findings concerning the severity of illness among the high sUA group. Accordingly, we consider that the strict selection procedure indeed enhanced the overall validity of our results.
Third, this study was limited to a mostly Japanese population. In Japan, doctors have historically prescribed XOIs to patients with hyperuricemia regardless of diagnosis of gout or tophi. Indeed, only 9.4% of our analyzed population had been diagnosed with gout at the initiation of XOIs. This unique setting may also limit the generalizability of this study. Fourth, while we focused on patients with reference range eGFR and without proteinuria by analyzing disease names, procedure code histories, and laboratory data, our database did not contain imaging or pathological information. In the process of selecting patients, this might have led to misclassification of the target population. Fifth, eGFR data, as outcome variable in this study, were automatically and inclusively collected from each hospital's electronic medical record. We did not observe and could not obtain the specific reason for individual eGFR measurements. Thus, the actual reason for significant eGFR decline might have varied among cases. Further studies are necessary to overcome these limitations.
Conclusion
This study showed that early initiation of XOIs based on sUA value did not predict a significant benefit on renoprognosis, even among patients with preserved kidney function and no proteinuria. Therefore, an elevated sUA may not be a suitable indicator of the time to initiate XOIs at least aiming to reducing a decline in eGFR.
Footnotes
Acknowledgments
The authors deeply thank all staffs who were involved in this research.
Authors' Contributions
A.T.: conceptualization, methodology, visualization, investigation, writing—original draft preparation. T.F.: conceptualization, methodology, writing—reviewing and editing. M.T.: methodology, writing—reviewing and editing, supervision. K.K.: conceptualization, writing—reviewing and editing, supervision.
Author Disclosure Statement
A.T. has received research funds from the Japan Society for the Promotion of Science's KAKENHI Grants and SECOM Science and Technology Foundation. T.F. has been employed by the Department of Digital Health and Epidemiology, an Industry-Academia Collaboration Course supported by Eisai Co., Ltd., Kyowa Kirin Co., Ltd., Real World Data Co., Ltd., and Mitsubishi Corporation; and has received consulting fees from Real World Data Co., Ltd. and speaker fees from Asahi Kasei Pharma Corporation and EPS Corporation. M.T. has received research funds from Japan Society for the Promotion of Science's KAKENHI Grants. K.K. receives research funds from Eisai Co., Ltd., Kyowa Kirin Co., Ltd., OMRON Corporation, and Toppan, Inc.; consulting fees from Advanced Medical Care, Inc., JMDC, Inc., and Shin Nippon Biomedical Laboratories Ltd.; executive compensation from Cancer Intelligence Care Systems, Inc.; and honoraria from Chugai Pharmaceutical Co., Ltd., and Pharma Business Academy.
Funding Information
This study was supported by SECOM Science and Technology Foundation. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Figure S7
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.