
Abstract
Purpose:
To determine whether high-sensitivity C-reactive protein (hsCRP) is associated with incident Metabolic Syndrome (MetS) among U.S. Hispanic/Latino adults.
Patients and Methods:
The Hispanic Community Health Study/Study of Latinos is a longitudinal observational cohort assessing cardiovascular health among diverse U.S. Hispanic/Latino adults. hsCRP was measured at visit 1 (2008–2011) and classified as low, moderate, or high, based on the Centers for Disease Control and Prevention and American Heart Association (CDC/AHA) guidelines. All MetS components [abdominal obesity, triglycerides, high-density lipoprotein (HDL) cholesterol, blood pressure, and fasting glucose] were measured at visit 1 and visit 2 (2014–2017). MetS was defined as the presence of three or more components based on the 2005 definition from the modified Third Report of the National Cholesterol Education Program Adult Treatment Panel (modified NCEP ATP III). Participants free of MetS at visit 1 and with complete data on hsCRP and all MetS components were included (n = 6121 participants). We used Poisson regression analysis to determine whether hsCRP was associated with incident MetS after adjusting for demographic, behavioral, and clinical factors. All analyses accounted for the complex survey design of the study.
Results:
In fully adjusted models, moderate versus low hsCRP was associated with a 33% increased risk of MetS [incidence rate ratio (IRR): 1.33, 95% confidence interval (CI): 1.10–1.61], while high versus low hsCRP was associated with a 89% increased risk of MetS (IRR: 1.89, 95% CI: 1.58–2.25).
Conclusions:
Greater levels of hsCRP were associated with new onset of MetS in a diverse sample of U.S. Hispanic/Latino adults. Results suggest that hsCRP may be an independent risk factor for MetS.
Introduction
Metabolic syndrome (MetS) is characterized by a combination of cardiometabolic risk factors, including obesity, dyslipidemia, hypertension, and/or hyperglycemia. 1 MetS is associated with a twofold risk of developing cardiovascular disease (CVD) over 10 years. 1 Among U.S. adults from the 2018 National Health and Nutrition Examination Survey (NHANES), 38.3% have MetS. 2 Among Hispanic/Latino adults, the largest ethnic minority population in the United States, 3 35.0% have MetS, with substantial differences by Hispanic/Latino background group. 4 For example, Hispanic/Latino adults of Puerto Rican background have a higher prevalence of both MetS and its individual components compared with other Hispanic/Latino background groups. 4,5
C-reactive protein (CRP) is a marker of both acute and chronic systemic inflammation. 6 –8 CRP is implicated in the development of endothelial dysfunction in part by augmenting an inflammatory cascade. 9 This cascade is associated with several underlying features of MetS, such as insulin resistance and central adiposity. 10 High-sensitivity C-reactive protein (hsCRP) has been shown to be an independent predictor of incident cardiovascular events 11 and has been posited to be a risk factor for MetS. 12 Many cohort studies have identified a direct contribution of high CRP to MetS development and subsequent cardiovascular risk. 9 In fact, longitudinal studies show associations between higher hsCRP with incident MetS. 12 –14 For example, findings from mainland Asia and Europe found higher levels of hsCRP were associated with an increased risk of developing MetS among Chinese, Japanese, Korean, Italian, and Finnish adults. 13 –21
Among non-Hispanic Black (NHB) and non-Hispanic White (NHW) U.S. adults, a higher CRP level was associated with a greater risk of incident MetS and developing adverse levels of the individual MetS components. 11,22 Data from NHANES reported the prevalence of moderate (1.0–3.0 mg/L) or high (>3.0 mg/L) CRP concentrations in ∼60% of Hispanic/Latino adults. 23 Yet, limited longitudinal data exist from U.S. cohorts, including U.S. Hispanic/Latino adults relating hsCRP to MetS.
Although U.S. Hispanic/Latino individuals are the largest ethnic group in the United States, they remain underrepresented in research studies. 24 Given that Hispanic/Latino individuals account for roughly 19% of the U.S. population, 25 and MetS is highly prevalent, 4 it is important to understand the role of hsCRP in MetS development in this population. This is especially timely, as a growing body of literature increasingly suggests that hsCRP should be part of the decision tree on whether or not to start a patient on a statin therapy. 9 Therefore, the goal of our study was to determine whether hsCRP level is an independent predictor of incident MetS in U.S. Hispanic/Latino adults. To do so, we leveraged data from the Hispanic Community Health Study/Study of Latinos (HCHS/SOL), a comprehensive longitudinal cohort with representation from Hispanic/Latino adults of diverse backgrounds.
Methods
Study population
The HCHS/SOL is an ongoing, observational cohort study assessing cardiovascular health among diverse U.S. Hispanic/Latino adults. 26,27 Briefly, self-identified Hispanic/Latino adults living in the United States were recruited using a probabilistic sampling design from four urban centers in the Bronx, NY, Chicago, IL, Miami, FL, and San Diego, CA. Visit 1 occurred between 2008 and 2011 and included 16,415 eligible participants 18–74 years of age who were subject to a standardized examination. Visit 2 occurred about 6 years later from 2014 to 2017 and included re-examination of 11,623 participants. At both visits, participants completed questionnaires pertaining to health behaviors and medical history, underwent laboratory testing and physical examinations. Participants provided informed consent at both visits and IRB approvals were obtained from all participating institutions (Albert Einstein College of Medicine, University of Illinois at Chicago, University of Miami, and San Diego State University).
Measures
High-sensitivity C-reactive protein
The hsCRP was obtained from fasting blood serum samples at visit 1 and measured on a Roche Modular Chemistry Analyzer using an immunoturbidimetric method. 28 Participants with an hsCRP value >10 mg/L were excluded (n = 1374), as such values may be indicative of an active infection; 29 therefore, included visit 1 hsCRP values ranged from 0.1 to 10.0 mg/L. From these plausible hsCRP values, we subsequently categorized hsCRP as low (<1.0 mg/L), moderate (1.0–3.0 mg/L), or high (>3.0 mg/L), based on the Centers for Disease Control and Prevention and American Heart Association (CDC/AHA) guidelines. 29
Metabolic syndrome
Based on the modified Third Report of the National Cholesterol Education Program Adult Treatment Panel (modified NCEP ATP III) from 2005, 30 MetS was defined as the presence of at least three of five individual components [abdominal obesity, elevated triglycerides, low high-density lipoprotein (HDL) cholesterol, elevated blood pressure (BP), and elevated fasting glucose].
Abdominal obesity
Waist circumference (WC) was taken at the uppermost lateral border of the right ilium and rounded to the nearest centimeter using a measuring tape. 31 Abdominal obesity was defined as a WC ≥102 cm in men or ≥88 cm in women. 30
Elevated triglycerides
Triglycerides were measured from fasting blood samples using the glycerol blanking enzyme method. 28 A triglyceride level ≥150 mg/dL was defined as elevated. 30
Low HDL
HDL was measured from fasting blood samples using the direct magnesium/dextran sulfate method. 28 Low HDL cholesterol levels were defined as <40 mg/dL in men or <50 mg/dL in women. 30
Elevated BP
BP was measured three times, after an initial 5-min rest period in the seated position, with 30-sec intervals in between measurements, using an automated sphygmomanometer on the participant's right arm. 31 The average of the three measurements was used. Elevated BP was defined as systolic BP (SBP) ≥130 mmHg, diastolic BP (DBP) ≥85 mmHg, or self-reported use of BP-lowering medication. 13,30,32
Elevated glucose
Blood glucose was measured from fasting blood samples using the hexokinase enzymatic method. 28 Elevated glucose was defined as fasting glucose ≥100 mg/dL or self-reported use of diabetes medication. 13,30,32
We also utilized two alternative definitions of MetS components based on (1) the International Diabetes Federation (IDF) definition of MetS 33 and (2) Hispanic/Latino WC cutoffs based off HCHS/SOL findings. 34 The IDF definition of MetS includes stricter WC thresholds for men (WC ≥90 cm) and women (≥80 cm), based on criteria for South Asians, 33 while HCHS/SOL cutoffs use a more conservative definition of abdominal obesity for men (WC ≥102 cm) and women (≥97 cm). 34
Other variables of interest
Participants self-reported demographics and health behaviors through a standardized questionnaire. Participants' provided their date of birth and age (in years) was calculated, study site (Chicago, IL; Miami, FL; Bronx, NY; San Diego, CA), sex (male or female), education level (less than a high school education or at least a high school education), household income (less than $30,000 or at least $30,000), health insurance status (yes or no), marital status (married/living with partner or single/separated/divorced/widowed), employment status (full-time, part-time, not retired and not employed, or retired and not employed), nativity/years residing in the 50 U.S. states/DC (U.S. born, ≥10 years in the 50 U.S. states/DC, or <10 years in the 50 U.S. states/DC), and self-identified Hispanic/Latino background (Central American, Cuban, Dominican, Mexican, Puerto Rican, South American, or mixed/other).
Participants also reported their smoking behavior (current or former/never smoker), alcohol behavior (current use or former/never alcohol use), whether 2008 physical activity guidelines were met (yes or no, assessed through the Global Physical Activity Questionnaire 35 ), and diet quality (assessed through two 24-hr recalls and using the Alternative Healthy Eating Index-2010 diet score, with a higher score indicative of a healthier diet). 36 Symptoms of depression was assessed using the 10-item Center for Epidemiological Studies Depression Scale (CESD-10). 37 Body mass index (BMI, kg/m2) was measured using height (in meters) and weight (in kilograms).
Analytic sample
For our primary analysis, of the 16,415 HCHS/SOL participants at visit 1, we excluded anyone: with visit 1 MetS (n = 2850), missing any visit 1 MetS component (n = 403), missing visit 1 hsCRP (n = 172), or with visit 1 hsCRP >10.0 mg/L (n = 1374). We further excluded individuals who did not participate in visit 2 (n = 4798) or were missing any visit 2 MetS components (n = 697). Our final analytic sample included 6121 participants free from MetS at visit 1 and with complete data at both visits.
Given our additional interest in the incidence of each MetS component, a secondary analytic sample was restricted to 1328 participants who met the initial inclusion criteria and who were also free of any individual MetS components at visit 1.
Statistical analyses
We described characteristics overall and by hsCRP category. To determine whether visit 1 characteristics differed across hsCRP categories, we used analysis of variance for continuous variables or chi-squared tests for proportions. We also estimated the age-adjusted cumulative incidence of MetS, individual MetS components, and the number of MetS components met (range 0–5) overall and stratified by hsCRP category. Next, we used multivariable adjusted Poisson regression models to determine whether hsCRP was associated with incident MetS, each MetS component, and the number of MetS components met, with follow-up time included as an offset in all models.
We used four models. Model 1 was adjusted for age, and study site. Model 2 included Model 1 adjustments in addition to sex, Hispanic/Latino background, income, education, marital status, employment, health insurance status, and nativity/years in the United States. Model 3 included Model 2 adjustments in addition to alcohol use, smoking, CESD-10 score, physical activity, diet quality, and BMI (except for in abdominal obesity models). For our analysis of individual MetS components, we included an additional Model 4, which was adjusted for Model 3 covariates (except BMI), in addition to the individual MetS components when applicable (e.g., fasting glucose model was adjusted for all other MetS components, except for fasting glucose).
We repeated our estimation of the age-adjusted cumulative incidence of MetS and the multivariable adjusted Poisson models in two sensitivity analyses (using our modified definitions of MetS). Lastly, given that previous research has found differences in MetS incidence by sex 13 and HCHS/SOL was designed to assess health status by Hispanic/Latino background, 26,27 we used multiplicative interaction terms in minimally adjusted models to determine whether associations differed by sex or Hispanic/Latino background. All analyses were conducted in SUDAAN Version 11.0.3 to account for the complex survey design of the study.
Results
Among Hispanic/Latino adults free from MetS, 48% were 18–34, 31% were 35–49, 16% were 50–64, and 5% were 65 or older (Table 1). About half (49%) were women, 8% were Central American, 18.5% were Cuban, 10% were Dominican, 40% were Mexican, 13% were Puerto Rican, and 5% were South American. Approximately 29% had less than a high school education, 59% had an income <$30,000, 48% had health insurance, and 25% were U.S. born. Mean BMI was 27.4 kg/m2, 38.3% had low hsCRP, and 24.5% had high hsCRP. Compared with low hsCRP, those with high levels of hsCRP were more likely to be older, female, were less likely to have met 2008 physical activity guidelines, and had poorer diet quality (P < 0.05).
Baseline Demographics Among Those Without Metabolic Syndrome Overall (2008–2011), and According to High-Sensitivity C-Reactive Protein Category, the Hispanic Community Health Study/Study of Latinos
Indicates characteristic differs significantly (P < 0.05) by hsCRP category (chi-squared tests for categorical variables and ANOVAs for means).
AHEI, Alternative Healthy Eating Index; ANOVA, analysis of variance; BMI, body mass index; CESD-10, 10-item Center for Epidemiological Studies Depression Scale; CVD, cardiovascular disease; DBP, diastolic blood pressure; HDL, high-density lipoprotein; HS, high school; hsCRP, high-sensitivity C-reactive protein; PA, physical activity; SBP, systolic blood pressure; SE, standard error.
hsCRP and MetS
After an average of 6.1 years of follow-up, the age-standardized cumulative incidence of MetS was 20.5% [95% confidence interval (CI): 19.1–21.9] and differed by hsCRP category. Compared with a low hsCRP level (cumulative incidence = 15.3%; 95% CI: 13.3–17.6), the cumulative incidence of MetS was higher among those with moderate (20.4%; 95% CI: 18.1–22.8, P < 0.05) or high hsCRP 28.2% (95% CI: 25.3–31.2, P < 0.05). In multivariable adjusted models (Model 3), compared with a low hsCRP level, moderate and high hsCRP were associated with a 33% [incidence rate ratio (IRR): 1.33, 95% CI: 1.10–1.61], and a 89% (IRR: 1.89, 95% CI: 1.58–2.25) increased risk of MetS, respectively (Table 2). The interaction between hsCRP with sex or Hispanic/Latino background was not significant (P for interaction >0.10).
Multivariable Adjusted Associations Between High-Sensitivity C-Reactive Protein and Incident Metabolic Syndrome, the Hispanic Community Health Study/Study of Latinos (2008–2017)
Model 1: adjusted for age, and study site. Model 2: adjusted for Model 1 variables and sex, Hispanic/Latino background, income, education, marital status, employment, health insurance, and nativity. Model 3: adjusted for Model 2 variables and alcohol use, smoking, CESD-10, PA, and diet.
Indicates IRR is significant (P < 0.05).
CI, confidence interval; IRR, incidence rate ratio.
hsCRP and MetS components
Among participants without any individual MetS components at visit 1 (N = 1328), the age-standardized cumulative incidence of meeting each component was 22.0% (95% CI: 18.4–26.0) for abdominal obesity, 9.8% (95% CI: 7.9–12.1) for elevated triglycerides, 11.4% (95% CI: 9.4–13.9) for low HDL cholesterol, 16.0% (95% CI: 12.9–19.5) for elevated BP, and 18.8% (95% CI: 16.0–21.9) for elevated fasting glucose (Fig. 1). The cumulative incidence of abdominal obesity, low HDL cholesterol, and elevated BP was greater among those with high hsCRP compared with those with low hsCRP (P < 0.05). Furthermore, at visit 2, 30.8% (95% CI: 26.5–35.4) had one MetS component, 14.9% (95% CI: 12.4–17.8) had two MetS components, 3.1% (95% CI: 2.2–4.4) had three MetS components, 1.7% (95% CI: 0.8–3.5) had four MetS components, and 0.3% (95% CI: 0.1–0.8) had all five MetS components (Fig. 2). This distribution differed by category of hsCRP with a greater number of components among those with higher hsCRP (chi-squared P value <0.05).
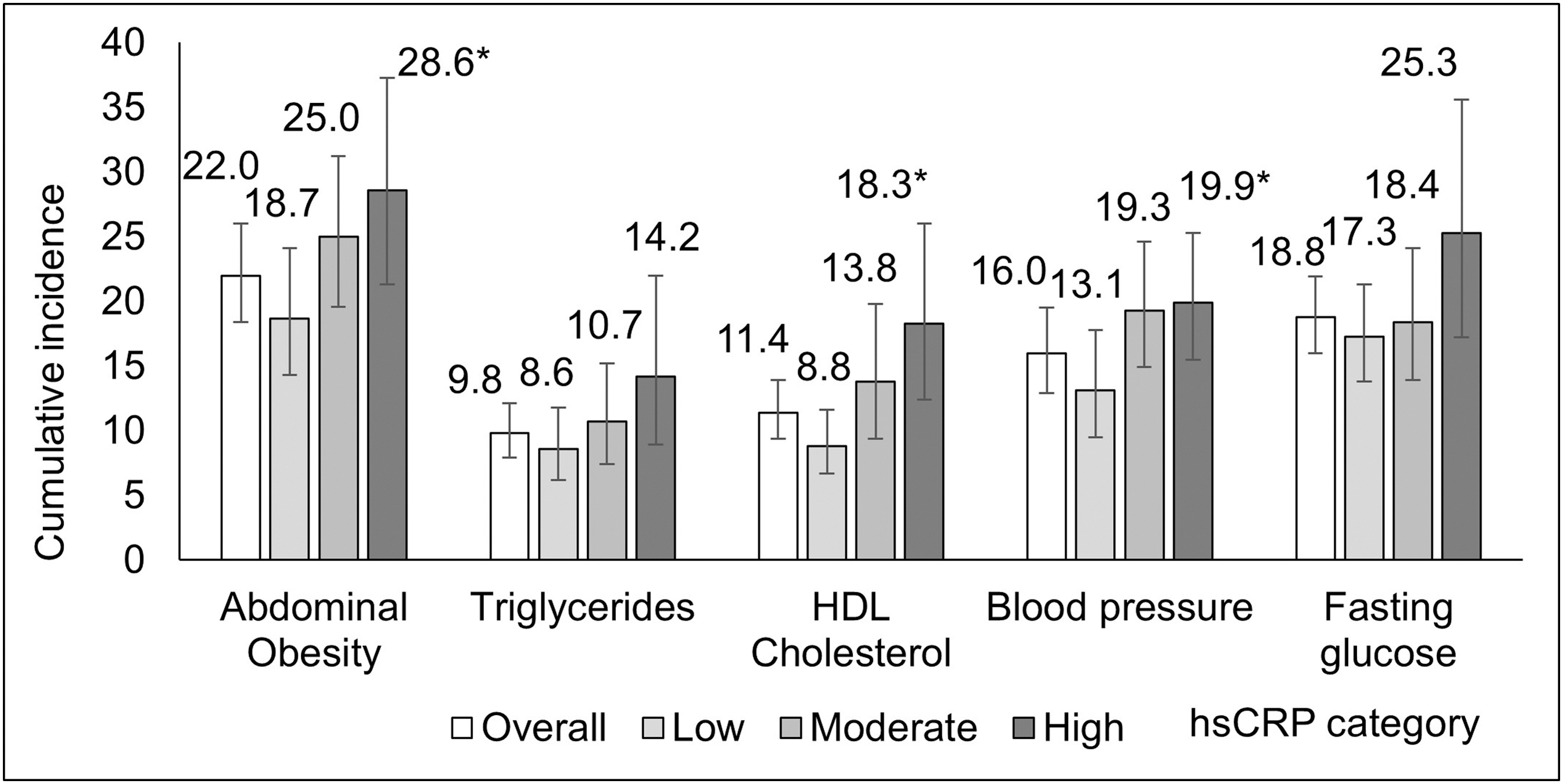
Age-adjusted cumulative incidence of individual MetS components by hsCRP category among participants with 0 MetS individual components at visit 1, the HCHS/SOL (2008–2017). *Significantly different from reference “Low” category (P < 0.05). HCHS/SOL, Hispanic Community Health Study/Study of Latinos; HDL, high-density lipoprotein; hsCRP, high-sensitivity C-reactive protein; MetS, metabolic syndrome.
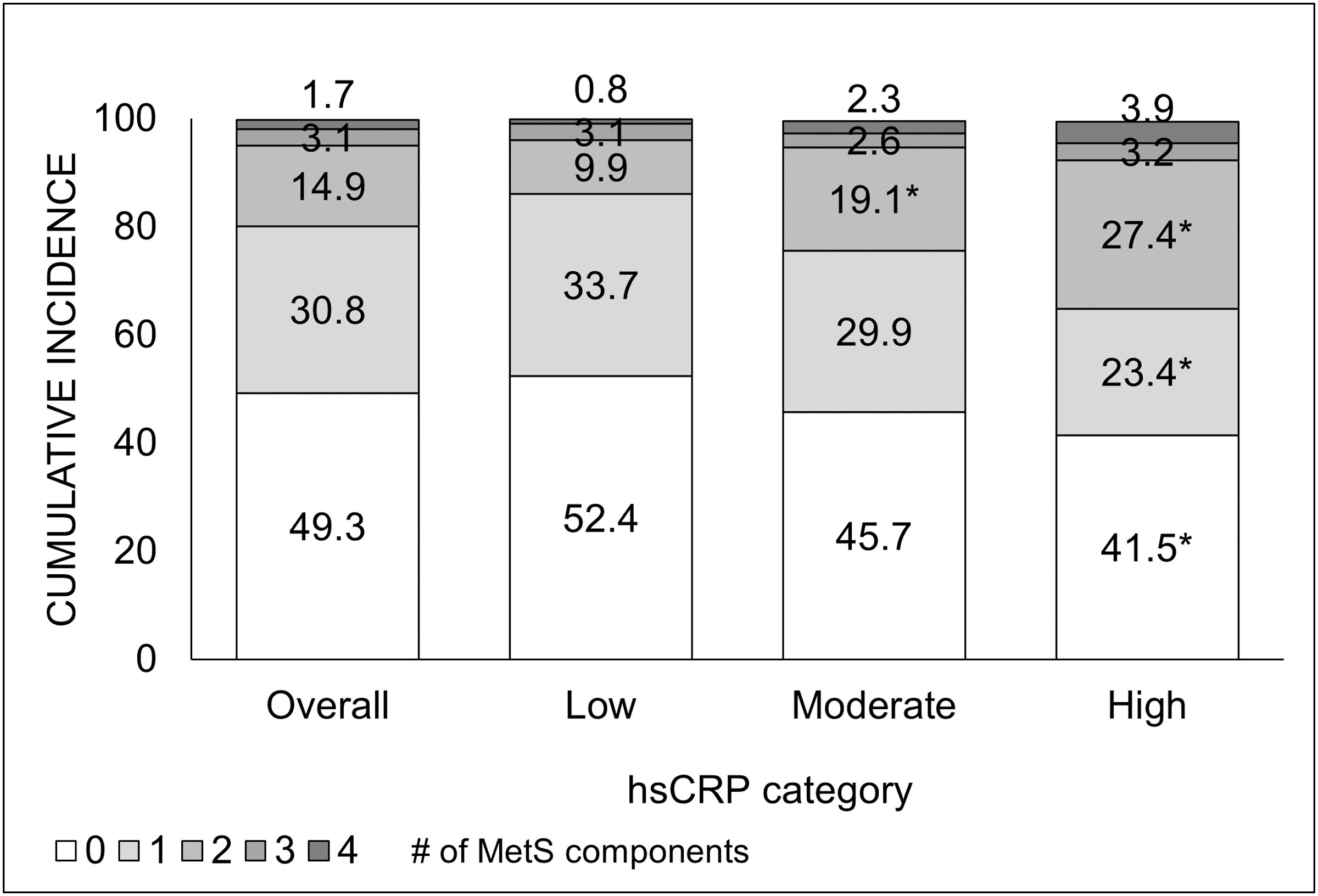
Age-adjusted cumulative incidence of the number of MetS components by hsCRP category among participants with 0 MetS individual components at visit 1, the HCHS/SOL (2008–2017).a aDid not include five components because there were only five participants with five components. *Indicates significantly different from reference “Low” category (P < 0.05).
In multivariable adjusted models, among participants without any MetS components at visit 1, compared with a low hsCRP level, the increase in the number of MetS components was higher by 0.28 (95% CI: 0.06–0.50) with moderate hsCRP, and higher by 0.51 (95% CI: 0.20–0.81) with high hsCRP. Furthermore, compared with a low hsCRP level, high hsCRP was associated with an 81% (IRR: 1.81, 95% CI: 1.24–2.65) increased risk of abdominal obesity, a 129% (IRR: 2.29, 95% CI: 1.31–4.01) increased risk of elevated triglycerides, and a 116% (IRR: 2.16, 95% CI: 1.31–3.54) increased risk of low HDL cholesterol (Table 3). After adjusting for individual MetS components, results were attenuated but largely consistent (Model 4).
Multivariable Adjusted Associations Between High-Sensitivity C-Reactive Protein and Metabolic Syndrome Individual Components Among Participants with 0 Metabolic Syndrome Components at Visit 1, the Hispanic Community Health Study/Study of Latinos (2008–2017)
Model 1: adjusted for age, and study site. Model 2: adjusted for Model 1 variables and sex, Hispanic/Latino background, income, education, marital status, employment, health insurance, and nativity. Model 3: adjusted for Model 2 variables and alcohol use, smoking, CESD-10, PA, diet, and BMI (not included in abdominal obesity models). Model 4: adjusted for Model 3 variables (not including BMI) and abdominal obesity (except in abdominal obesity models), triglycerides (except in triglyceride models), HDL cholesterol (except in HDL cholesterol models), blood pressure (except in blood pressure models), and fasting glucose (except in fasting glucose models).
Indicates IRR is significant (P < 0.05).
Sensitivity analyses
Results were largely consistent with main results and showed that both moderate and high hsCRP were associated with incident MetS using both the IDF (Supplementary Tables S1 and S2) and the HCHS/SOL definition (Supplementary Tables S1 and S2).
Discussion
In a population-based sample of diverse U.S. Hispanic/Latino adults we found that higher levels of hsCRP were associated with an increased risk of MetS, its individual components, and the number of MetS components. Specifically, over a 6-year follow-up period, the cumulative incidence of MetS was 20.5%; and 89% higher among participants with high versus low hsCRP. We found these associations robust to several sensitivity analyses utilizing alternative definitions of MetS. Among participants without any MetS components at visit 1, we found that high compared with low hsCRP was associated with an increased risk of meeting the individual MetS components of abdominal obesity, hypertriglyceridemia, and hyperlipidemia. Our results suggest that hsCRP is an important risk factor of those at risk of MetS.
Previous research in non-Hispanic/Latino populations has identified associations between hsCRP and MetS. 11,13,14,19,21 Findings among Chinese adults 13,15 and Finnish men 14 found that CRP was associated with higher risk of MetS in a dose–response manner. Notably, among Mexican women of the Mexico City Diabetes Study, the highest tertile of CRP was associated with increased risk of MetS development compared with women in the lowest tertile of CRP, after a similar 6-year follow-up period. 32
We extend this evidence to U.S. Hispanic/Latino adults, also showing a dose–response association, even after adjustment for clinical and lifestyle factors, like diet quality and exercise. This dose–response pattern may be attributed to the augmented endothelial and oxidative stress 38 resulting from higher concentrations of hsCRP and has been found in other studies. For example, research in a community-based cohort of NHW and NHB adults found a dose–response relationship between hsCRP with incident diabetes, heart failure, and coronary heart disease. 39 As the largest ethnic or racial minority population in the United States, 3 the burden of CVD and cardiometabolic disorders 5 is projected to increase among Hispanics/Latinos in the forthcoming decades. 40 Identification of modifiable factors that may contribute to MetS, such as inflammation, is critical to mitigating progression toward MetS and ultimately, CVD.
The incidence of MetS within HCHS/SOL was higher compared with studies conducted in non-U.S.-based populations. 13,19,32 This is likely attributable to unfavorable baseline characteristics and reflects the differential cardiometabolic health profile in the United States compared with other nations. 41 For example, only 20% of HCHS/SOL participants had high cardiovascular health defined by the AHA's Life's Essential 8 framework. 42 In fact, WC, BMI, and fasting glucose were all higher among HCHS/SOL participants compared with Chinese and Finnish adults. 13,14 This is meaningful given that U.S. Hispanic/Latino adults have a higher predisposition for elevated inflammation 23 due to unique cultural and social stressors, such as language barriers, lack of access to health care providers, and low socioeconomic status. 3,43 Given that 75% of the HCHS/SOL cohort was not born in the 50 U.S. states/DC, HCHS/SOL participants face adversity from immigration and acculturation. 44 –47
This is significant as racial/ethnic discrimination, an anti-immigrant sentiment, and acculturative stress has been shown to exert negative influences in health behaviors, mental and physical health, 44 –48 and psychosocial stress has been implicated in increased systemic inflammation. 49 Nonetheless, even among a younger population, we still found an association between hsCRP and MetS after adjusting for demographic and behavioral characteristics.
The European Society of Cardiology recommends measuring hsCRP in individuals with unfavorable cardiovascular risk profiles 50 and the NCEP ATP III has emphasized identification of individuals with MetS as a high-risk group for the development of CVD. 51 Although hsCRP is not regularly collected in clinical settings in the United States, hsCRP is now being considered as a novel marker of quantitative cardiovascular risk assessment. 52 Since the release of the 2003 CDC/AHA hsCRP risk category levels, 29 substantial evidence exists showing high compared with low hsCRP, measured at one point in time, is associated with an increased risk of cardiovascular events. 10,11 Furthermore, longitudinal increases in CRP concentration contribute to greater pathogenesis of atherosclerosis, and cardiovascular and neurodegenerative disease. 8,53
However, pharmacologic therapies, such as a statin medication, have been shown to reduce inflammation levels, thereby, decreasing risk of cardiovascular events among those with MetS. 9 Despite this, the prevalence of statin use was only 23% among Hispanic/Latino adults free of CVD with a high risk of a future cardiovascular event. 54 In addition to lifestyle changes that could decrease inflammation, such as diet modification and physical activity, 55,56 public health efforts are also needed to increase uptake of statins among the Hispanic/Latino population. 57
The current study has some limitations. First, two measurements of hsCRP are recommended for accuracy and reliability. 29 In our study, hsCRP was measured once at baseline. To help address any inaccuracy associated with our measure, we opted to restrict hsCRP to levels at or below 10.0 mg/L, to exclude those with a likely active infection. 58 Second, our study would have been enhanced by the inclusion of other inflammatory biomarkers, cytokines, such as interleukin-6 and tumor necrosis factor-α. 29,30,59 However, such inflammatory biomarkers were not collected. Nevertheless, hsCRP is the most extensively studied inflammatory biomarker and is widely used to measure a proinflammatory state. 29,30,60,61
Third, of the 16,415 enrolled participants at visit 1, only 11,623 participants were re-examined 6 years later at visit 2, of which 5502 participants had MetS at visit 1. Furthermore, given that there were only 1328 participants without any MetS components at visit 1, we were not powered to detect MetS among this population with favorable baseline health. Likewise, our ability to detect differences by Hispanic/Latino background was limited. Despite this, we still found a strong main effect between hsCRP and incident MetS. Finally, while representative of four U.S. urban centers, these findings cannot be generalized to all U.S. Hispanic/Latino adults.
The present study also has noteworthy strengths. To the best of our knowledge, this is the first study examining the association between hsCRP and incident MetS in a population-based sample of diverse U.S. Hispanic/Latino adults. Standardized measurements of hsCRP and all MetS components were utilized to minimize information bias. The modified 2005 NCEP ATP III definition for MetS was used, which aligned with the updated guidance from the American Diabetes Association in 2004 for impaired fasting plasma glucose. 30 Another strength of the study was the use of robust Poisson regression, which includes follow-up time as an offset in our model, thereby providing information on incidence rate and accounting for different follow-up times among participants. Finally, we found consistent graded associations between moderate and high hsCRP and incident MetS, using either strict or conservative WC thresholds, and findings were robust to sensitivity analyses.
Conclusions
In summary, in a population-based sample of diverse U.S. Hispanic/Latino adults, moderate and high hsCRP were associated with an increased risk of MetS (and individual MetS components) over a 6-year follow-up period. Associations remained significant after adjusting for demographic, clinical, and lifestyle factors. These results highlight the utility of hsCRP as a predictor of MetS among U.S. Hispanic/Latino adults.
Data Sharing Statement
All data can be made available through request from the HCHS/SOL publication committee (https://sites.cscc.unc.edu/hchs).
Footnotes
Acknowledgments
The authors thank the staff and participants of HCHS/SOL for their important contributions. The contents of this report are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health (NIH). Investigators Website: ![]() . Please contact the corresponding author for analytic methods and data used in this article. The conducted research was not preregistered.
. Please contact the corresponding author for analytic methods and data used in this article. The conducted research was not preregistered.
Authors' Contributions
R.A.M. was involved in conceptualization, methodology, data analysis, and article writing. T.E. was involved in conceptualization (supporting), methodology (supporting), supervision, and article writing. O.M.D., N.S., A.M.P., L.C.G., G.A.T., D.S.-A., M.L.D., A.P., and M.M.L. reviewed and edited the article. R.A.M. and T.E. are the guarantors of this work, and, as such, had full access to the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
The HCHS/SOL is a collaborative study supported by contracts from the National Heart, Lung, and Blood Institute to the University of North Carolina (HHSN268201300001I/N01-HC-65233), University of Miami (HHSN268201300004I/N01-HC-65234), Albert Einstein College of Medicine (HHSN268201300002I/N01-HC-65235), University of Illinois at Chicago (HHSN268201300003I/N01-HC-65236 Northwestern University), and San Diego State University (HHSN268201300005I/N01-HC-65237). The following institutes/centers/offices have contributed to the HCHS/SOL through a transfer of funds to the National Heart, Lung, and Blood Institute: National Institute on Minority Health and Health Disparities, National Institute on Deafness and Other Communication Disorders, National Institute of Dental and Craniofacial Research, National Institute of Diabetes and Digestive and Kidney Diseases, National Institute of Neurological Disorders and Stroke, and NIH Office of Dietary Supplements. T.E. is currently supported by the National Institute on Minority Health and Health Disparities (K01MD014158).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.