
Abstract
Background and Objective:
Hypertension and type-2 diabetes are strong risk factors for cardiovascular diseases, and their management requires lifestyle changes, including a shift in dietary habits. The consumption of salt has increased in the last decades in some countries, but its association with type-2 diabetes remains unknown. Thus, we aimed to estimate the amount of salt intake among adults with and without diabetes and to assess whether concomitant hypertension and diabetes are associated with higher salt intake.
Methods:
Data from 11,982 adults 35–74 years of age enrolled in the baseline of the Longitudinal Study of Adult Health-Brasil study (2008–2010) were studied. A clinical and anthropometric evaluation was performed, and their daily salt intake was estimated by the overnight 12-hr urine sodium excretion.
Results:
Salt intake (gram per day) was higher in participants with diabetes as compared with those without diabetes, regardless of sex (men: 14.2 ± 6.4 vs. 12.4 ± 5.6, P < 0.05; women: 10.5 ± 4.8 vs. 9.1 ± 4.1, P < 0.05). However, salt intake is high in participants with fasting glucose ≥126 mg/dL or HbA1c ≥6.5%, but not in participants with blood glucose 2 hr after the glucose tolerance test ≥200 mg/dL. When hypertension and diabetes coexisted, salt consumption was higher than among people without these conditions. The prevalence of hypertension increased with increasing salt intake in women with diabetes, but not in men with this condition.
Conclusions:
Our findings highlight the high consumption of salt in individuals with diabetes and/or hypertension, and the need for effective strategies to reduce salt consumption in these groups of increased risk for major cardiovascular events, especially in women.
Introduction
The increased consumption of salt by the population has brought to light the intricate connection between dietary patterns and cardiovascular diseases (CVD). The greater availability and consumption of ultra-processed food have contributed to elevated salt (sodium) intake in many countries. 1 Studies in robust samples in the general population of several developed countries have revealed a daily salt intake of ∼10 g, surpassing the recommended limit of <5 g/day. 2 Data from the National Health and Nutrition Examination Survey (NHANES) revealed a median salt intake of ∼8.5 g/day among the adult population of the United States. 3 Furthermore, findings from the Longitudinal Study of Adult Health (ELSA-Brasil) in Brazil showed a salt consumption of 11 g/day in adults, being slightly higher in men (12.9 g/day) than in women (9.3 g/day). 4
As the pivotal component of salt, sodium serves essential functions in nerves and muscles, in addition to directly contributing to the maintenance of extracellular water and electrolyte balance. However, high sodium intake is deemed a significant risk factor for CVD, primarily due to the associated increase in blood pressure (BP) and the development of hypertension. 1,5 In addition to its effect in increasing BP due to extracellular volume expansion, heightened salt intake can directly affect other structures that play a key role in BP control, such as endothelial function, autonomic control of the heart, and cardiac and vascular structure. 6 –8 The INTERSALT study 9 evidenced a direct association between salt intake and age-related elevation in BP in 48 out of the 52 studied populations. Numerous other studies have supported these findings, revealing elevated BP levels with increased salt intake 4,10 as well as a reduction in BP following salt intake reduction. 11
Diabetes constitutes a major global health problem given the continuous damage to the blood vessels with the progression of this disease. Diabetes can both impair endothelial function and expedite the vascular aging process, thus increasing BP. 12,13 In fact, over 60% of individuals with diabetes have concomitant hypertension. 14 It is already consolidated that diabetes and hypertension are independent risk factors for CVD and that the simultaneous presence of these two conditions increases the incidence of CVD. 15 Therefore, strict control of BP and glucose levels is essential for the prevention and treatment of microvascular and macrovascular damage in individuals with diabetes and hypertension, thereby avoiding the high mortality rate associated with these two diseases.
The effective management of diabetes and hypertension relies on modifications to the patient's lifestyle. High salt intake is a classical cardiovascular risk factor with a powerful effect on BP levels. 8 However, there is a debate regarding whether individuals with diabetes exhibit higher salt intake compared with those without diabetes. For instance, Kang et al. 16 reported in a large sample of Korean adults that patients with diabetes consumed less salt than those without diabetes. In contrast, a recent meta-analysis showed higher salt consumption in individuals with diabetes than in patients without diabetes. 17 Noteworthy, increased salt intake is associated with CVD even in patients with diabetes. 18 Therefore, our objective is to compare the sex-specific salt intake in a large sample of Brazilian adults with and without diabetes. Additionally, we aim to assess whether the simultaneous presence of hypertension and diabetes could be associated with a higher salt intake.
Methods
Study participants and design
The ELSA-Brasil study is an ongoing prospective cohort that included 15,105 adults at baseline (2008–2010), 35–74 years of age. All participants were active and retired public servants of five public universities and one research institution in six Brazilian state capitals (Belo Horizonte, Porto Alegre, Rio de Janeiro, Salvador, São Paulo, and Vitória). At baseline, all participants were invited to face-to-face interviews, clinical and anthropometric examinations, and laboratory and imaging examinations conducted by trained and certified research staff. 19 Detailed information regarding the study design and the main characteristics of the cohort are found elsewhere. 20,21 For the present study, we excluded 977 participants with self-reported previous CVD (myocardial infarction, stroke, congestive heart failure, coronary revascularization, including the use of vascular stents). Since sodium intake was evaluated based on a 12-hr overnight urine collection, we also excluded 2,292 participants without urine collection or if the collection was not validated.
Clinical and anthropometric measures
The clinical, anthropometric, and laboratory data were obtained in the morning period followed by an interview to collect the self-reported medical history, medications under regular use, and sociodemographic information.
In the ELSA-Brasil cohort, diabetes was defined as having at least one of the following criteria: (i) fasting blood glucose ≥126 mg/dL; (ii) blood glucose 2 hr after 75 g oral glucose tolerance test (GTT) ≥200 mg/dL, (iii) HbA1c ≥6.5%, (iv) the regular use of glucose-lowering medications, or (v) a previous medical diagnosis. 22,23 The systolic and diastolic blood pressure (SBP and DBP, respectively) and the heart rate were measured in the sitting position following a 5-min resting period. Three consecutive measurements, with a 2-min interval between them, were obtained with an oscillometric device (OMRON HEM 705CPINT, São Paulo, Brazil) in a silent and temperature-controlled room (20–24°C). The mean of the last two measurements was calculated. Hypertension was defined as SBP ≥140 mmHg and/or DBP ≥90 mmHg, and/or the use of BP-lowering drugs. 24
The body weight (Toledo Scale, Brazil) and height (Seca stadiometer) were obtained with the participant wearing light clothes, and, from these parameters, the body mass index (BMI) was calculated by dividing the weight by the squared height (kilogram per square meter). Waist circumference, measured at the midpoint between the last rib and the iliac crest, was measured with an inelastic tape, and the average of two measurements was used for the analysis. 24,25
A fasting blood sample was collected after 10–14 hr fasting and was processed by a central laboratory to measure total cholesterol, high-density lipoprotein cholesterol, and triglycerides (TG) by an enzymatic colorimetric method. Low-density lipoprotein cholesterol was calculated through the Friedewald equation for TG <400 mg/dL or measured by a direct method when TG ≥400 mg/dL. Fasting glucose, glycated hemoglobin (HbA1c), and uric acid levels were enzymatically determined. The glomerular filtration rate was estimated according to the Chronic Kidney Disease Epidemiology Collaboration (CKD-Epi) formulae without correction for race. 26
Urine collection
Participants received verbal and written instructions about the procedures for the overnight urine collection (12 hr). All participants were advised not to exercise the day before examinations. The collection kit included two large, wide-opened bottles (2 L each), an instruction form, and a handling bag. The participants were instructed to urinate in the bathroom around 7 p.m., and from there, to collect all urine in a bottle until the next morning. The last urine collection should be performed ∼12 hr after the last bathroom void. Participants were asked to record the exact times of the start and end of urine collection on the form and to report any potential loss of urine during the collection period. They were also instructed to keep the collected urine in a refrigerator and to bring it to the investigation center within 2 hr of the last urine collection. A few participants finished the collection right before the biochemical, anthropometric, and BP measurements. Upon arriving at the investigation center, participants were asked about the exact time they started and ended the collection.
The collected urine was aliquoted in sterile bottles and stored at −80°C until the evaluation of creatinine using the Jaffé method, and sodium and potassium concentrations through selective electrodes. The 12-hr urine collection validation was based on three defined criteria: volume ≥250 mL, collecting time between 600 and 840 min (10–14 hr), and a 12-hr creatinine excretion ≥7.2 and <16.8 mg/kg in men and ≥5.6 and <12.6 mg/kg in women. 4 The creatinine, sodium, and potassium urinary excretions were adjusted for 12 hr. Based on a validation study in a sample of adults, and assuming that all the excreted sodium is from the NaCl ingestion, the daily salt intake (gram per day) was estimated by dividing the 12-hr nocturnal sodium excretion by 0.47. 27 We considered the cutoff recommended by the American Heart Association (1500 mg of sodium, 3.75 g of salt) 28 and the American Diabetes Association (2300 mg of sodium, 5.75 g of salt). 29
Statistical analyses
All statistical analyses were performed using the SPSS 22.0 statistical software (SPSS, Chicago, IL, USA). The differences were considered statistically significant at two-sided P < 0.05. For continuous variables, data were presented as mean ± standard deviation or as absolute frequency and percentage for categorical variables. The adjustment for a Gaussian distribution was verified with the Kolmogorov–Smirnov test. To assess differences between clinical and anthropometric parameters among different groups, a Student's t-test was used. To compare the frequency of categorical variables between different salt intake or age categories, a chi-squared test was applied. Pearson's correlation analysis was used to test the correlation between salt intake and fasting blood glucose, HbA1c, and blood glucose post-GTT. The analysis of covariance was used to evaluate the association between salt intake and fasting glucose categories, controlling for the following variables: age, BMI, glomerular filtration rate, and use of BP-lowering drugs. In the case of a significant F test, Bonferroni's post hoc analysis was applied to reveal individual differences between groups.
Ethics statement
The Ethics Committees of the six participating institutions approved the present study, and all participants signed the free and informed consent form before the data collection. Confidentiality was guaranteed on participant data, and each individual's identity was hidden for all analyses. The research was completed in accordance with the Declaration of Helsinki as revised in 2013.
Results
After excluding 977 participants with previous CVD, and 2292 participants with nonvalidated urine collection, the analyses were conducted in a final sample comprising 11,982 participants (6385 women and 5597 men) with validated urine collection. The prevalence of diabetes was 19.2%, being higher in men than in women (22.9% in men vs. 15.9% in women, P < 0.05). Table 1 presents the clinical and anthropometric characteristics of the whole sample, stratified by sex and by the presence or absence of diabetes. Anthropometric variables were higher in participants with diabetes than in those without diabetes, as well as the lipid profile was worse in participants with diabetes. Also, SBP and DBP were significantly higher among participants with diabetes, regardless of sex.
Clinical and Anthropometric Characteristics of the Longitudinal Study of Adult Health-Brasil Participants Stratified by Sex and the Status of Diabetes
Continuous variables were compared using Student's t-test, and categorical variables were compared using Chi-squared test.
BMI, body mass index; DBP, diastolic blood pressure; GFR, glomerular filtration rate; GTT, glucose tolerance test; Hb1Ac, glycated hemoglobin; HDL-c, high-density lipoprotein cholesterol; HR, heart rate; LDL-c, low-density lipoprotein cholesterol; SBP, systolic blood pressure; TG, triglycerides; WC, waist circumference.
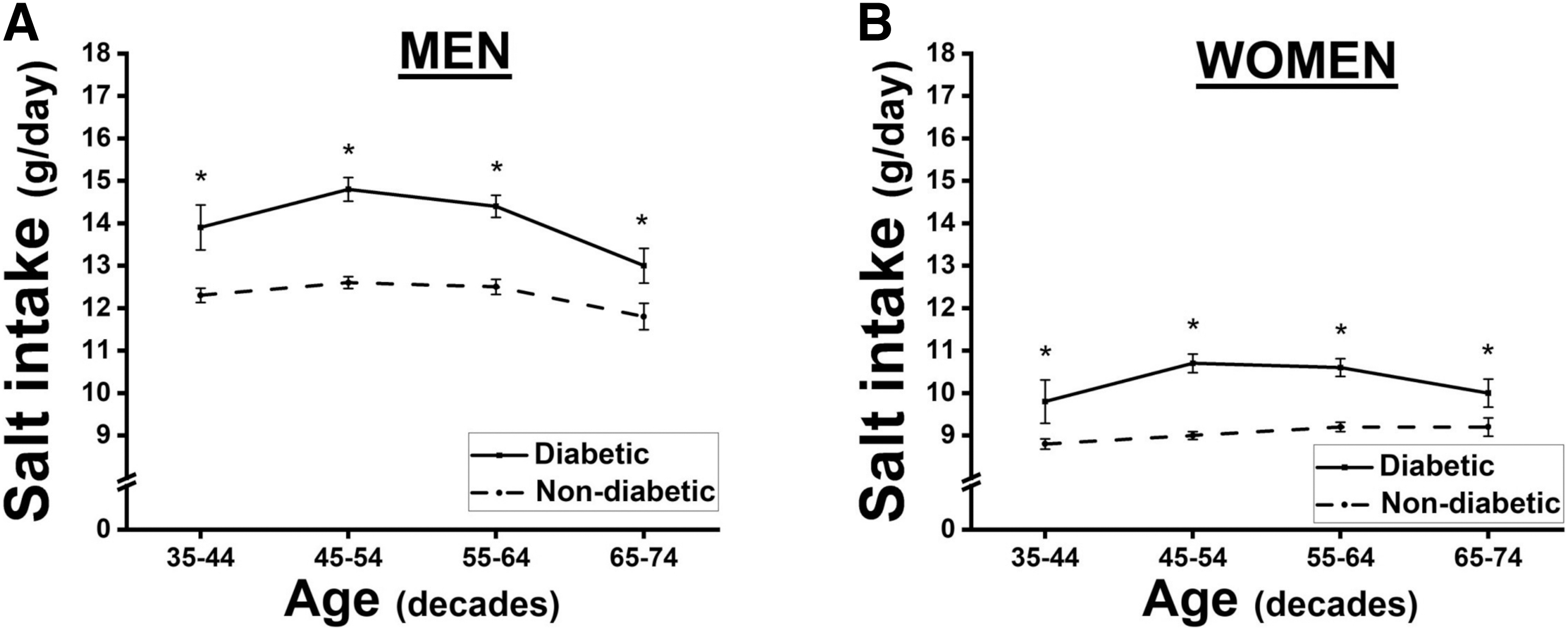
The daily salt intake estimated by the 12-hr urine sodium excretion was higher in men than in women (men 12.8 ± 5.9 g/day, women 9.3 ± 4.3 g/day; P < 0.05). Moreover, the salt intake was higher in participants with diabetes than without diabetes, regardless of sex (men: diabetics 14.2 ± 6.4 vs. nondiabetics 12.4 ± 5.6, P < 0.05; women: diabetics 10.5 ± 4.8 vs. nondiabetics 9.1 ± 4.1, P < 0.05). The salt intake was slightly higher (although without statistical significance) in those participants with the use of BP-lowering drugs, both in those without diabetes (men with the use of BP-lowering drugs: 12.8 ± 6.3 vs. men not using BP-lowering drugs: 12.3 ± 5.5; women with the use of BP-lowering drugs: 9.4 ± 4.7 vs. women not using BP-lowering drugs: 8.9 ± 4.0) or in those with diabetes (men with the use of BP-lowering drugs: 14.4 ± 6.5 vs. men not using BP-lowering drugs: 14.1 ± 6.2; women with the use of BP-lowering drugs: 10.6 ± 4.9 vs. women not using BP-lowering drugs: 10.4 ± 4.6).
We observed a positive correlation between salt intake and fasting glucose (r = 0.181, P < 0.001), HbA1c (r = 0.139, P < 0.001), and blood glucose post-GTT (r = 0.110, P < 0.001) in the whole sample, without significant differences between men and women. It is noteworthy that 73% of our sample showed a salt consumption higher than 5.75 g/day, being slightly higher in individuals with diabetes than in those without diabetes (75.9% vs. 72.3%, P < 0.001). Also, when we considered the AHA cutoff of 3.75 g/day, 96.8% of our sample was over that limit (men 98.6% and women 95.2%).
Figure 1 (A in men and B in women) shows the daily salt consumption between men and women with and without diabetes in different age categories. Significant differences in salt intake according to age categories were not observed, regardless of sex or diabetes diagnosis. Moreover, the mean salt intake was lower in women than in men, independently of age. However, in men (Fig. 1A) and women (Fig. 1B), mean salt intake was higher in participants with diabetes as compared with those without diabetes, regardless of age. No significant interaction was found between age and diabetes diagnosis (P = 0.307 for men and P = 0.214 for women).
Daily salt intake by age categories in men
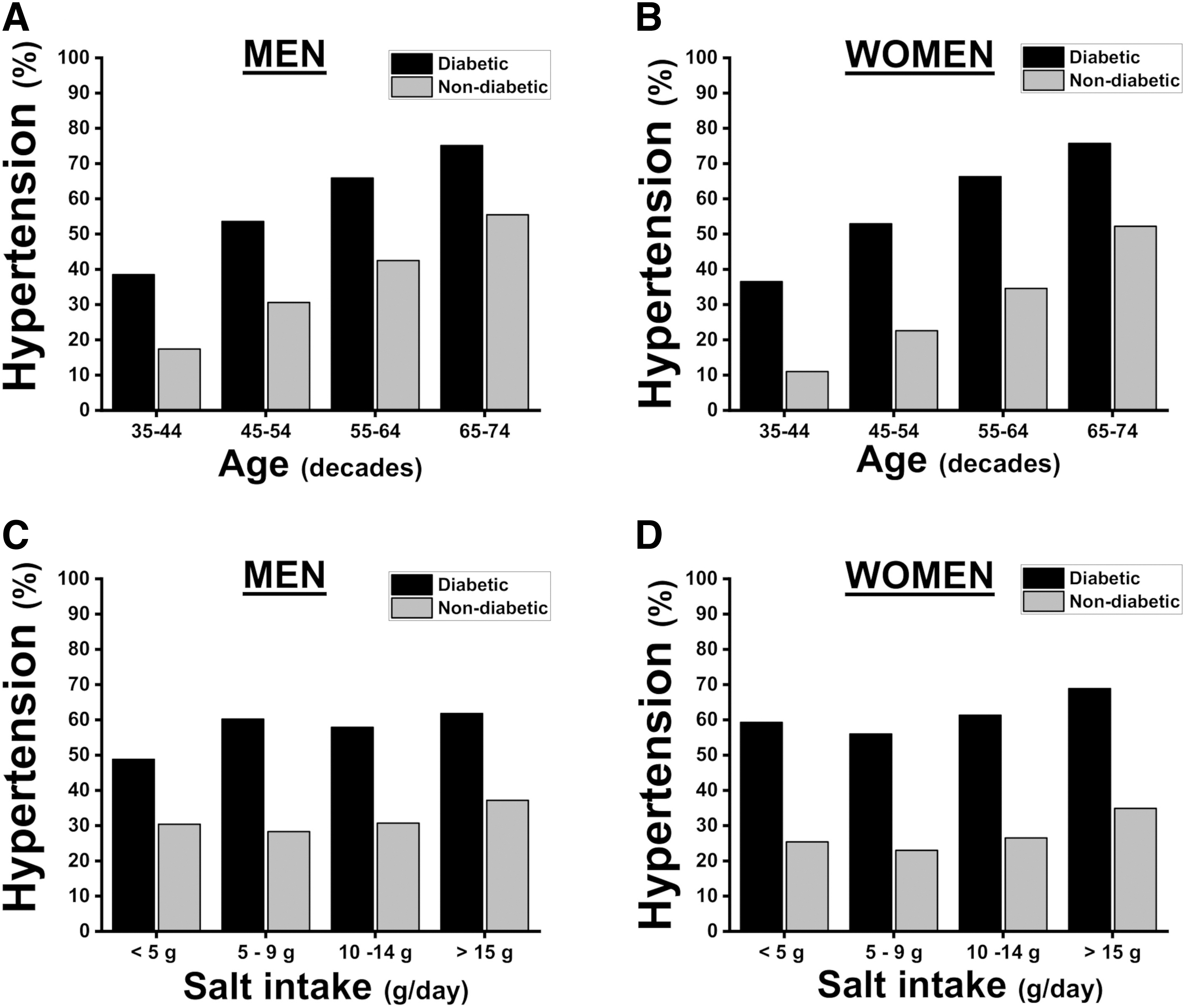
The prevalence of hypertension by age categories is presented in Fig. 2 (A for men and B for women). As expected, the prevalence of hypertension increases significantly with age, regardless of sex (P < 0.001). Moreover, the prevalence of hypertension was higher in participants with diabetes as compared with those without diabetes, regardless of sex or age (P < 0.001). When we evaluated the prevalence of hypertension among participants with and without diabetes and its association with daily salt consumption (Fig. 2C, D), a progressive increase in the prevalence of hypertension was observed toward higher mean salt intake extracts in women with diabetes (P = 0.035), but not men (P = 0.306). Among participants without diabetes, the prevalence of hypertension increases progressively across the categories of daily salt intake, regardless of sex.
Hypertension prevalence by age categories stratified by diabetes diagnosis in men
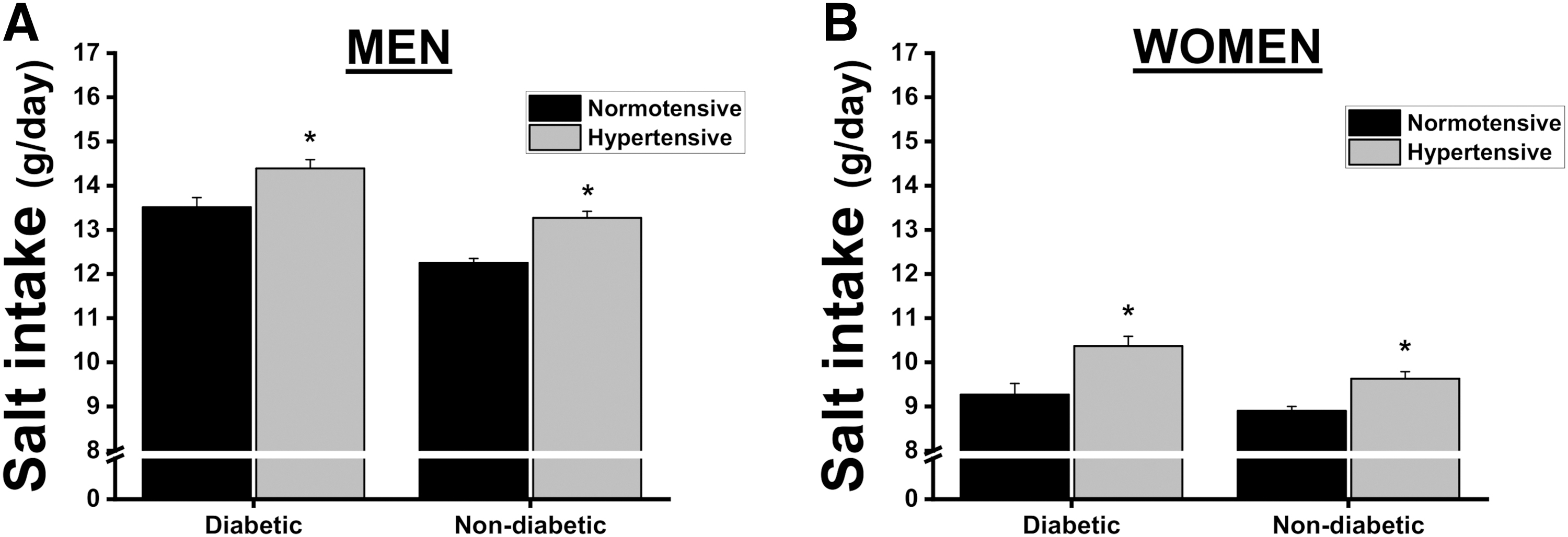
The next step was to evaluate whether salt consumption would be different in individuals with diabetes and concomitant hypertension. It is possible to observe in Fig. 3 that the mean salt intake was higher in men (Fig. 3A) and women (Fig. 3B) with diabetes, regardless of the hypertension diagnosis, even after adjustment for confounders, including age, BMI, estimated glomerular filtration rate (GFR), and the use of any BP-lowering drug, including diuretics. Moreover, salt intake was higher in hypertensive participants without diabetes as compared with those normotensive participants. We also observed that salt intake was higher among participants with simultaneous diabetes and hypertension than any other group, regardless of sex (Fig. 3). Finally, stratifying for the three laboratory criteria for the diagnosis of diabetes, salt intake is high in participants with fasting glucose ≥126 mg/dL or HbA1c ≥6.5%, but not in participants with blood glucose 2 hr after the glucose tolerance test ≥200 mg/dL (Table 2), after adjustment for confounders (age, BMI, GFR, and the use of any BP-lowering medication).
Salt intake in men
Salt Intake Based on Fasting Glucose, HbA1c, and 2-hr Post-Glucose Tolerance Test, Stratified by Sex and Blood Pressure Status
Values were adjusted by age, BMI, GFR, and use of any BP-lowering drugs. Data are presented as mean ± SD.
Indicates P < 0.05 versus the first category.
Indicates P < 0.05 versus the second category.
SD, standard deviation.
Discussion
Our results revealed a daily salt intake of 10.9 g in a cohort of Brazilian adults without CVD, highlighting that salt intake was ∼20% higher in participants with diabetes compared with those without this disease. Furthermore, we observed that individuals with both diabetes and hypertension had higher salt intake than any other group, regardless of sex. Finally, our findings support previous studies, indicating that 73% of the cohort consumes more than 5.75 g of salt per day, with this amount being slightly higher in individuals with diabetes.
People around the world consume more salt than recommended. Studies have shown that salt intake surpasses any guideline recommendation for any group or age category and is associated with high morbidity and mortality. 11 Some groups, however, show higher consumption than others. The NHANES study showed that 89% of the American population exceeds the recommended amount (5.75 g/day) of daily salt consumption. 30 An Australian study showed that only a few individuals with type 2 diabetes consume salt according to the recommended guidelines. 31 Provenzano et al. in the ENHANCE study reported that salt intake in individuals with diabetes is higher than in the whole North American population, with only 20% of the population following the recommended (5.75 g/day) daily intake. 32 Our results showed a daily salt intake of 10.9 g in the whole sample and this value was ∼20% higher in individuals with diabetes.
A few mechanisms seem to justify the association between high sodium intake and type-2 diabetes. Although controversies still exist, studies suggest an association between salt intake and insulin resistance pointed out as the underlying cause of several cardiometabolic alterations observed in individuals with diabetes, hypertension, and metabolic syndrome. 33,34 High salt intake is associated with decreased insulin sensitivity, which is mediated at least in part by the renin–angiotensin–aldosterone system (RAAS), inflammation, and oxidative stress. 35 Moreover, it is believed that an increased salt intake is directly associated with the development of overweight/obesity, due to its ability to induce an elevated intake of sweetened beverages, which are known to be associated with the development of cardiometabolic disorders. 36 An elevated salt intake seems to suppress the RAAS, decreasing the sodium reabsorption in the renal system, and thus increasing its excretion, mainly through aldosterone. However, the increased activity of sodium–glucose cotransporter 2 due to the increased glucose filtration can increase sodium reabsorption. 37
Aldosterone, a classical RAAS component has an important role in glucose metabolism, which reinforces the link between RAAS alterations and diabetic-associated disorders. Aldosterone is a mineralocorticoid that induces sodium retention and excretion of potassium and hydrogen ions in the kidney, being able to modulate salt appetite and sodium transport through the sympathetic nervous system. 38 Aldosterone production is supposed to be inhibited by sodium; however, this mechanism seems to be impaired under cardiometabolic disorders, mainly through inflammation and oxidative stress. Increased levels of aldosterone are associated with hypokalemia and consequent impairment of insulin secretion and insulin receptor functions, inducing glucose intolerance and thus being associated with diabetes. 39
The association between salt and BP is already well established. 8 It is known that high salt intake is accompanied by an increased blood volume and cardiac output, vascular dysfunctions, sympathetic nervous system activation, and arterial stiffness, in addition to other alterations that lead to increased peripheric resistance and BP increment. 8 Additionally, it has been shown that hypertensive individuals have an increased preference for salt as compared with normotensives, which may be due to taste preferences associated with social and dietary customs. 40 Some authors discuss the relationship between salt taste preference and BP, where individuals with a high salt taste sensitivity threshold seem to consume more salt and present increased BP levels. 41
In individuals with diabetes, controversy still exists concerning the preference for salty meals. Lawson et al. 42 showed that participants with diabetes have a preference for lower-salt meals. However, it has been shown that individuals with undiagnosed diabetes demonstrate a preference for high salt intake, but not those individuals already diagnosed. 43 Despite the controversy, it is known that diabetes is associated with gustatory alterations, mainly driven by xerostomia, 44 and neuropathy, 45 among others, which may justify at least in part the salt preferences in individuals with diabetes. 46
Concerning salt preference in the context of hypertension, evidence supports a stronger inclination toward salty foods among hypertensive individuals compared with normotensives, often coupled with a higher salt intake. 47 However, this assessment is intricate, as it raises the question of whether hypertensive patients exhibit an increased preference for salt, leading to elevated salt consumption and consequently reduced salt perception. Alternatively, it could be that due to a lower salt perception, they demonstrate an increased preference for and consumption of food with higher salt content. Despite the complexity, a few hypotheses may be drawn. The first hypothesis suggests that an increased salt preference may be an adaptive behavior due to an enhanced physiological need for sodium and/or other minerals. Additionally, the overactivation of the RAAS observed in these patients might change the sodium metabolism, thereby inducing higher salt consumption.
We observed that hypertension and diabetes are associated with increased salt intake. Our findings show that participants with both hypertension and diabetes consume more salt than those normotensives with diabetes. The BP response to salt intake, as previously mentioned, is at least partially dependent on the sensitivity of BP to salt. Patients with diabetes have high sensitivity of BP to salt intake, regardless of kidney function, due to several factors such as hyperinsulinemia, sympathetic activation, and renal function impairments. 37 Although studies aimed to evaluate the salt intake in this particular population (individuals with concomitant hypertension and diabetes) are scarce, the reduction in salt intake is capable of reducing BP levels in individuals with type-2 diabetes and glucose intolerance. 48 However, although the reduction of salt intake is widely implemented for the treatment of hypertension, the same is not true for diabetes management, especially due to uncertainties regarding the metabolic consequences of this intervention, which may justify their increased salt intake.
Some strengths of our study should be mentioned. First, the large sample size allowed subgroup analysis with robust statistical power, and the multivariate regression analysis was adjusted for major confounders. Also, our analyses were all conducted stratifying by sex. Finally, the ELSA-Brasil cohort has a strong quality of control for collecting data as well as for analyzing it. 19 As limitations, we could point to the cross-sectional design of our study, which does not allow us to exclude reverse causation. Also, while the gold standard technique for estimating sodium intake involves a 24-hr urine collection, we utilized an overnight 12-hr urine collection, a method supported by existing research. 49,50
Various methods, such as food questionnaires, dietary recall, and urine collection, are employed to assess sodium consumption. The most reliable and extensively validated method for evaluating sodium intake is the 24-hr urine collection, enabling the comprehensive measurement of all sodium excreted over a 24-hr period, closely reflecting sodium consumption during that timeframe. Although 24-hr urine collection is the recommended method for individual monitoring, challenges in its implementation raise the likelihood of incomplete collection.
Our previous findings indicate that an overnight 12-hr collection is more practical, with the 12-hr creatinine clearance demonstrating a strong correlation with the values observed over a 24-hr period. Additionally, the overnight collection minimizes sources of sodium loss other than urinary excretion. 27,51
Overall, the main findings of the current study highlight the close relationship between diabetes and hypertension, emphasizing that salt intake appears to exert detrimental effects on hypertensive individuals with diabetes, which is incremented when both conditions are simultaneously present. These findings light shed on the need for therapeutic interventions targeted at managing salt intake for individuals with diabetes, in addition to the already established interventions focused on hypertensive patients, as salt seems to not only have a significant role in diabetes pathophysiology but also cardiometabolic morbimortality.
Footnotes
Authors' Contributions
N.G.R.: conceptualization; methodology; and writing—original draft; D.F.L.: formal analysis and writing—original draft; R.H.G.: data curation and writing—review and editing; S.M.B.: data curation and writing—review and editing; M.d.C.B.M.: data curation and writing—review and editing; M.I.S.: data curation and writing—review and editing; B.B.D.: data curation and writing—review and editing; I.B.: data curation and writing—review and editing; P.A.L.: data curation and writing—review and editing; J.G.M.: conceptualization, supervision, and writing—review and editing; M.P.B.: conceptualization, data curation, formal analysis, supervision and data curation, and writing—review and editing.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
The ELSA-Brasil study was supported by the Brazilian Ministry of Health (Department of Science and Technology) and the Ministry of Science, Technology, and Innovation (FINEP, Financiadora de Estudos e Projetos), Grants No. 01 06 0010.00, 01 06 0212.00, 01 06 0300.00, 01 06 0278.00, 01 06 0115.00, and 01 06 0071.00, and CNPq (the National Council for Scientific and Technological Development).