
Abstract
Introduction:
Chronic kidney disease (CKD) is associated with metabolic disorders. However, the evidence for the causality of circulating metabolites to promote or prevent CKD is still lacking.
Methods:
The two-sample Mendelian randomization (MR) analysis was conducted to evaluate the latent causal relationship between the genetically proxied 486 blood metabolites and CKD. Genome-wide association study (GWAS) data for exposures were derived from 7824 European GWAS on metabolite levels, which have been extensively utilized in the medical field to elucidate the mechanisms underlying disease onset and progression. The random inverse variance weighted (IVW) is the primary analysis for causality analysis while MR-Egger and weighted median as complementary analyses. For the further identification of metabolites, reverse MR and linkage disequilibrium score regression were performed for further evaluation. The drug target for N-acetylornithine was subsequently supplemented into the analysis, with MR and colocalization analysis being utilized. Key metabolic pathways were identified via MetaboAnalyst 4.0 (https://www.metaboanalyst.ca/) online website.
Results:
N-acetylornithine was identified as a reliable metabolite that increases the susceptibility to estimated glomerular filtration rate (eGFR) decrease (β = 0.047; 95% confidence interval: −0.068 to −0.026; P IVW = 1.5E-5). The “glyoxylate and dicarboxylate metabolism” pathway showed significant relevance to CKD development (P = 6E-4), whereas the “glycine, serine, and threonine metabolism” pathway was also recognized as associated with CKD by general practitioners (P = 7E-4). Colocalization analysis revealed a robust genetic link between N-acetylornithine and both CKD and eGFR, with 85.1% and 99.4% colocalization rates, respectively. IVW-MR analysis substantiated these findings with a significant positive association for CKD (odds ratio = 1.43, P = 4.7E-5) and a negative correlation with eGFR (b = −0.04, P = 1.13E-31).
Conclusions:
MR was utilized to explore the potential causal links between 61 genetic serum metabolites and CKD. N-acetylornithine and NAT8 were further explored as a potential therapeutic target for CKD treatment.
Introduction
The main function of the kidneys is to filter waste products in the blood, and glomerular filtration rate (GFR) reflects the rate at which the kidneys filter blood per unit of time. 1 Kidney disease has a significant hereditary predisposition, and the kidneys are not only the target organ for many diseases but also drive and influence the progression of many systemic diseases. 2 Chronic kidney disease (CKD) arises from diverse underlying causes, manifesting clinically as a decline in kidney function and pathologically characterized by the presence of renal fibrosis. 3 Owing to its high global prevalence of 10%–16% in common people and over 50% in high-risk subpopulations and lack of therapeutic options, 4 CKD imposes heavy burden to health. 3,5
Serum metabolites, from a more nuanced micro-level perspective, offer insights into the etiology and progression of diseases and guide the investigation of potential drug targets. The 486 serum metabolites utilized in this study are derived from prior research and have been extensively applied across various medical fields, including the exploration of sepsis 6 and anxiety disorders. 7 Preliminary investigations within this domain have focused on the mannose molecule, yet they have not delved into the exploration of further drug targets. 8
In this article, we want to introduce a novel instrument, Mendelian randomization (MR), 9 to assist us in confirming the potential relationship between blood metabolites and CKD. In contrast to various other methodologies used in epidemiological studies, MR offers a unique advantage by delivering impartial assessments regarding the allocation of genetic variants at the time of conception. This approach is typically impervious to the influences of confounding elements and the issue of reverse causation. 10 –12 This research methodology, which uses innate genotypes as instrumental variables (IVs), emulates the design of randomized controlled trials (RCTs), thereby enhancing the reliability of the conclusions drawn and significantly mitigating the risk of reverse causality. 13,14
Owing to its significant analytical prowess, MR has seen extensive application over the past 10 years. It is utilized to deduce the causal relationships between risk factors and disease outcomes by leveraging publicly accessible genome-wide association study (GWAS) summary data. 15,16
Studies on biomarkers for the diagnosis and pathology of CKD using MR have been numerous. 17 The use of proteomic techniques in the blood of patients with CKD established testosterone-2 as an important cornerstone of clinically relevant physiological markers of kidney disease progression and pointed to other proteins that deserve further study. 18 Previous studies have noted that high-density lipoprotein is a protective factor for kidney function, in patients with CKD, whereas low-density lipoprotein is not causally associated with CKD. 19 Higher baseline levels of fibroblast growth factor-23, parathyroid hormone, and phosphate were associated with an increased risk of end-stage renal disease (ESRD) or death, respectively, independent of GFR. 20 Serum 6-bromotryptophan levels were identified as a risk factor for the exacerbation of CKD. 21 Advanced glycation end products include methylglyoxal (MG)-derived hydro imidazolidinone MG-H1, Nε-carboxymethyl-lysine, and glucosinolates advance CKD. 22 The single nucleotide polymorphism (SNP) rs13538, located within the NAT8 gene, has been identified as associated with N-acetylornithine levels in African American patients with CKD, further implicating its connection with CKD progression and estimated glomerular filtration rate (eGFR). We have taken note of this intriguing finding and are exploring its potential as a genetic target for CKD therapy. 23
We hypothesized that the genetically determined metabolites (GDMs) atlas could serve as a tool for deducing the causal influence of GDMs on CKD. To explore this, we used a two-sample MR strategy with the following objectives: (1) to evaluate the potential causal impacts of circulating human serum metabolites on the development of CKD, (2) to pinpoint specific GDMs exerting causal effects across four distinct GWAS related to CKD, (3) to uncover possible metabolic pathways that could shed light on the underlying mechanisms of anxiety disorders, and (4) to investigate drug targets for the prevention and delayed progression of CKD.
Methods
GWAS data for 486 blood metabolites
Genomic data for serum metabolites were obtained from the GWAS server. (http://metabolomics.helmholtz-muenchen.de/gwas/). By performing a GWAS study on the untargeted metabolome, Shin et al. obtained the most comprehensive serum metabolome GWAS data to date, screening 486 genetically influenced serum metabolites. 24 The researchers recruited 7824 participants from two European population cohorts, including 1768 participants in Germany and 6056 participants in the United Kingdom. Both studies were approved by local ethics committees, and all participants voluntarily signed informed consent forms prior to the study. After a rigorous screening process, 486 genetically influenced serum metabolites were ultimately screened, of which 309 are known, whereas the remaining 177 are unknown. Known metabolites are classified as peptides, nucleotides, amino acids, energy, cofactors and vitamins, lipids, carbohydrates, and xenobiotics, based on the Kyoto Encyclopedia of Genes and Genomes (KEGG) database. Ultimately, this GWAS incorporated 2.1 million SNPs. 24,25 More details can be found in Table 1. The flowchart of the study is shown in Fig. 1.

The overview of the study.
Basic Information About GWAS Datasets Involved
CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; UACR, urine albumin-to-creatinine ratio.
CKD genetics Consortium data
We analyzed the data gathered from the CKD genetics (CKDGen) Consortium to obtain effect estimates on three different parameters: quantitative eGFR, dichotomous eGFR < 60 mL/min/1.73 m2, and albuminuria for the selected variants. Kidney function was assessed using eGFR, a quantitative measure adjusted for sex and age. Out of 133,814 participants, the average eGFR was 87.12 ± 23.09 mL/min/1.73 m2. Albuminuria, quantified by the urine albumin-to-creatinine ratio (UACR) from spot urine samples, was assessed in a cohort of 54,450 participants. The analysis was performed using sex- and age-adjusted residuals following the natural logarithm transformation. Patients with diabetes were designated as the case group, whereas non-diabetic individuals served as the control group. 26 A cohort of 118,147 individuals with an eGFR below 60 mL/min/1.73 m2 were designated as the case group for CKD. 20,27 More details can be found in Table 1.
Instruments selection
In order to satisfy the most important assumption of relevance in MR, we screened the IVs with strict criteria. We adjusted the significance threshold to P < 1 × 10−5 to select SNPs related to metabolites. Then, we clumped SNPs by removing linkage disequilibrium (LD) (R 2 > 0.01) within 500 kb. The above criteria have proven to be reliable in the literature in the past. 28,29 To remove bias from faulty instruments, we computed R 2 and F statistics for each SNP. 20
SNPs with an F value less than 10 were considered inadequate and subsequently excluded. 30 We then extracted the previously obtained SNPs in the outcome and excluded the SNPs associated with the outcome (P < 1E-5). Furthermore, we harmonized the exposure with the data in the outcome and synergized the effect alleles. Then to fulfil hypothesis 3, we excluded SNPs directly associated with the outcome (P < 1E-5). 31
Estimation of causal effect and sensitivity analyses
The primary approach used for assessing the causal impact of potentially influential metabolites on eGFR, CKD, and UACR was the inverse variance weighted (IVW) analysis. This method aimed to evaluate the relationship between these metabolites and the outcome. To further investigate the presence of heterogeneity and pleiotropy effects, Cochran’s Q statistic and the corresponding P values were computed. 32
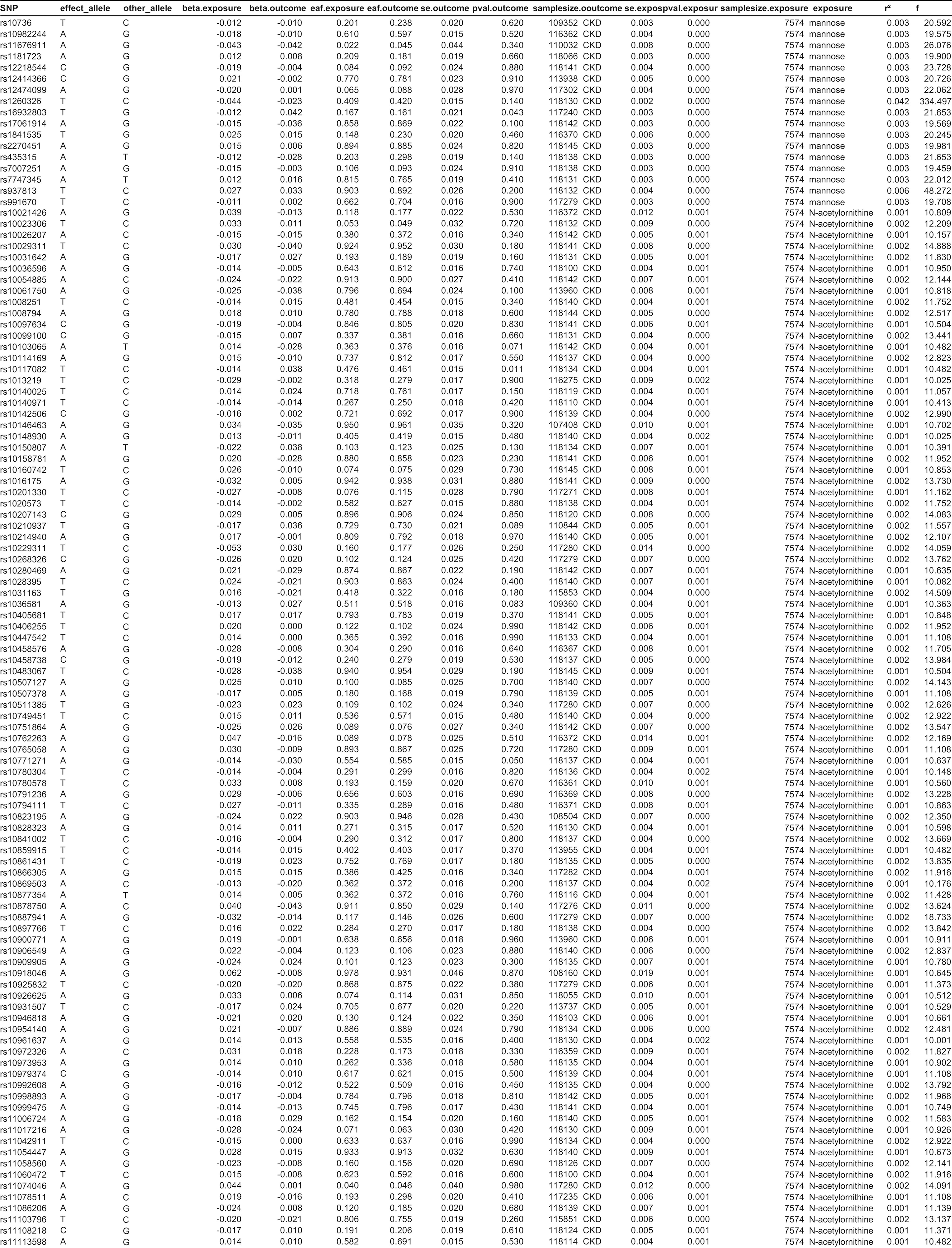
In order to effectively address the issue of horizontal pleiotropy, three complementary and rigorous sensitivity analyses were performed. First, the weighted median-based method was used, which yields a reliable estimate by considering valid IVs with a weight of at least 50%. 33 Second, the mode-based method was utilized, which offers a consistent effect estimate by assuming that the majority of the genetic variants are valid instruments, especially as the sample size increases. 34 Lastly, MR-Egger regression was used, providing a robust approach to test for potential horizontal pleiotropy. 35 These sophisticated analytical techniques collectively strengthen the validity and reliability of our findings. To validate any potential horizontal pleiotropic outliers that could significantly impact the estimation, we used two robust methods: Leave-one-out analysis and the MR pleiotropy residual sum and outlier (MR-PRESSO) method. 32 These analytical approaches provide a rigorous assessment of the data, allowing us to identify and address any influential outliers that may compromise the accuracy of our estimation. By incorporating these comprehensive validation techniques, we further enhance the credibility and robustness of our findings. 36 In essence, we conducted a meticulous screening of blood metabolites for their potential causal effects on CKD, using a range of rigorous criteria: (1) The P value derived from the primary analysis demonstrated statistical significance (P < 0.05, IVW method). (2) Consistency was observed in both the direction and magnitude of effects across all three MR methods utilized. (3) No evidence of heterogeneity or horizontal pleiotropy was found in the MR results, ensuring robustness. (4) The MR estimates remained largely unaffected by the presence of a single SNP, indicating their stability and reliability. MR results of CKD, eGFR, and UACR can be found in Table 2, Table 3, and Table 4, respectively. SNPs selected for mannose and N-acetylornithine can be found in Table 8.
Results of Primary and Sensitivity Analysis About CKD
IVW, inverse variance weighted; NSNP, Number of SNP.
Results of Primary and Sensitivity Analysis About eGFR
NSNP, Number of SNP.
Results of Primary and Sensitivity Analysis About UACR
NSNP, Number of SNP.
Evaluation of genetic correlation and directionality
However, MR estimates may violate causal effects in cases where there is a genetic correlation between exposure and the outcome of interest. 37,38 Although SNPs related to CKD were excluded in the selection of IVs, there is still a possibility that SNPs with no direct relation to CKD may mediate the genetic pathways of CKD. To address this concern and ensure that the causal effects are not confounded by the coheritability of the exposure with the outcome, we utilized linkage disequilibrium score (LDSC) regression and performed a reverse MR analysis. 39 That is, MR analyses were performed using CKD, eGFR, and UACR as exposures and 486 serum metabolites as end points. LDSC regression estimates the coinheritance of two traits based on SNP data by performing chi-squared statistics. Therefore, LDSC was implemented in this study to examine the genetic correlation between the screened metabolites and CKD. More detailed results of LDSC can be found in Table 5.
LDSC Results of 61 Associations to Outcomes Respectively
SE, Standard Error; RG, Regression; RGP, Regression p value.
Colocolization and drug target analysis
Bayesian colocalization, leveraging the “coloc” package with default settings, was applied to assess the probability of overlapping causal variants for two traits. Detailed methodology and package source code are available at the GitHub repository (https://github.com/chr1swallace/coloc). This analysis quantifies the posterior probability for five hypotheses, with a focus on Hypothesis 3, which assumes independent variants link both protein levels and molecular signatures to a common genomic region, and Hypothesis 4 (PPH4), which proposes shared variants for both associations. We used both the coloc.abf and coloc.susie algorithms, with colocalization evidence defined by a gene-based PPH4 exceeding 80%, as indicated by either algorithm. 40
We further developed an instrumental variable by identifying SNPs within a 100 kb window of the NAT8 gene, which are genome-wide significantly (P < 5E-8) associated with N-acetylornithine levels, to serve as proxies for the exposure to potential target drugs. To consolidate the findings, we utilized the IVW-MR approach to synthesize effect estimates derived from genetic variants linked to N-acetylornithine levels. In addition, we validated our results using external GWAS databases, specifically the ebi-a-GCST008026 and ieu-a-104 datasets. 41 More detailed results of colocolization and drug target analysis can be found in Table 6.
Colocalization Results and Drug Target Analysis
Metabolic pathway analysis
To explore the function of the identified serum metabolites, we used the MetaboAnalyst 4.0 (https://www.metaboanalyst.ca/) online website to perform the analyses. In order to obtain comprehensive and reliable results, all metabolites associated with CKD, UACR, and eGFR at P < 0.05 were included in the analysis. More detailed results of pathway enriched can be found in Table 7.
Primary Enrichment Results
FDR, False discovery rate.
Results
IVs selection
The range of instruments for each metabolite varied from 4 to 86, whereas two metabolites lacking the minimum requirement of three instruments were excluded from the MR analysis. The minimum F statistic for instrumental SNPs exceeded 10 for each metabolite, demonstrating the substantial strength of the instruments. The primary impact of these SNPs on metabolites is observed at the blood level, specifically at the translational level, with no investigation conducted into their functional implications.
Causal effects on 3 datasets related to CKD phenotype
In the IVW model, a total of 61 significant metabolite associations (IVW, P < 0.05) with three CKD-related phenotypes were successfully identified. Out of these associations, 39 were linked to known metabolites, whereas 22 associations were found for previously unidentified metabolites. 14,19,6 associations of known metabolites and 6,7,6 associations of unknown metabolites for CKD, eGFR, and UACR are shown in Fig. 2. MR results of CKD, eGFR and UACR are detailed in Figs. 3–5, respectively.
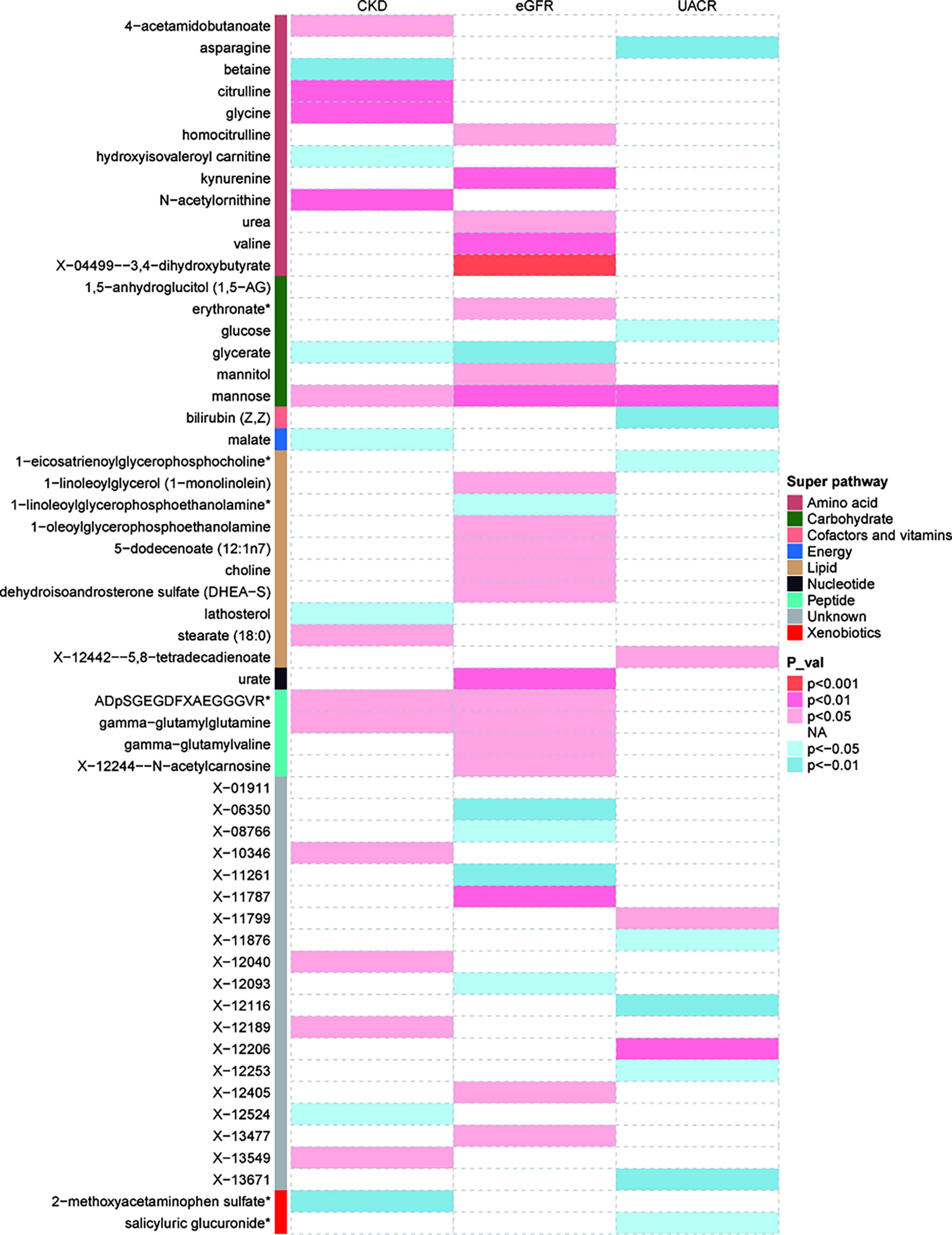
Mendelian randomization associations of known metabolites on the risk of the three different GWAS datasets of CKD, eGFR, and UACR (derived from IVW analysis). CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; GWAS, genome-wide association study; IVW, inverse variance weighted; UACR, urine albumin-to-creatinine ratio.
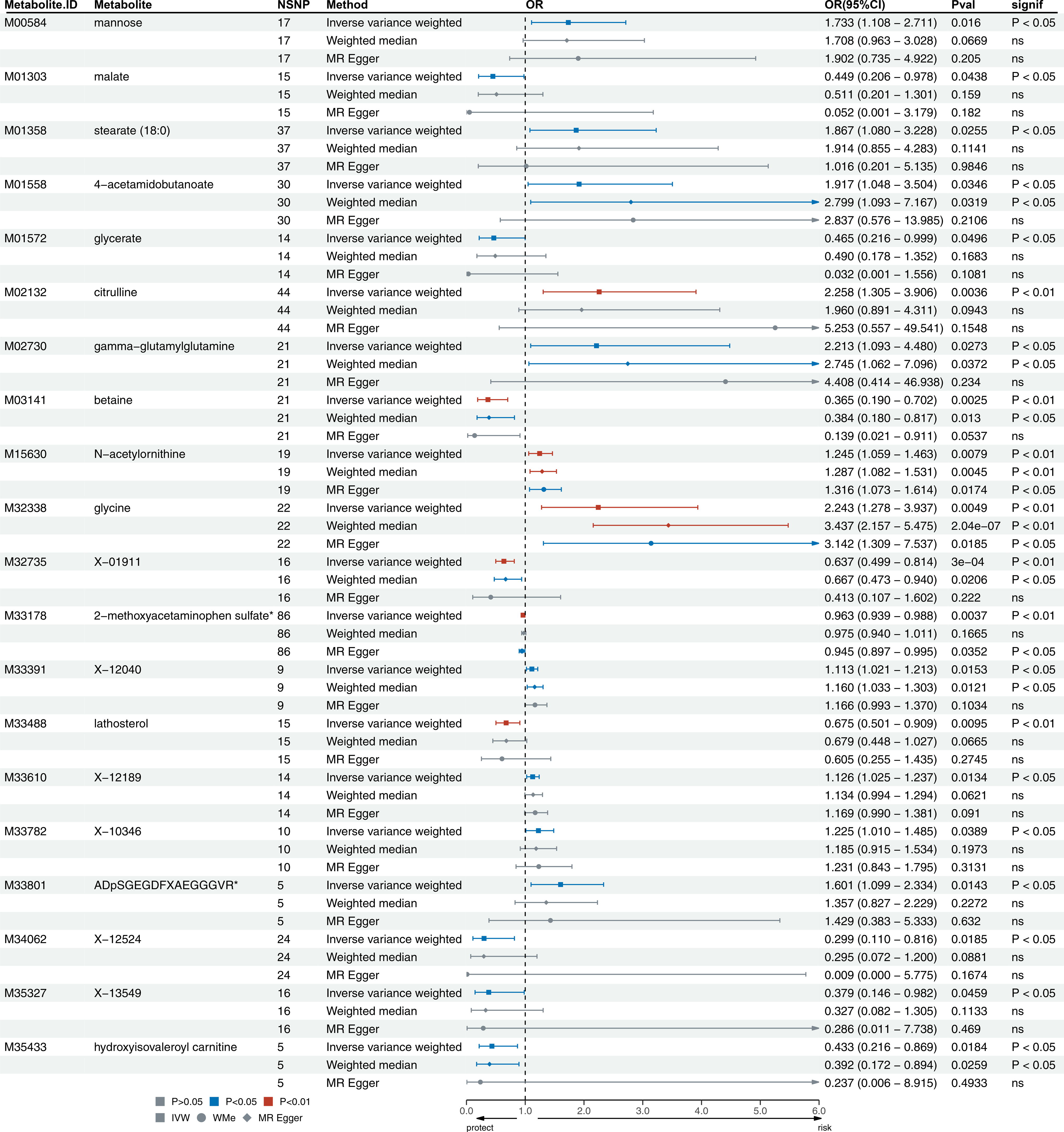
A forest plot about causal associations between 20 causal metabolites and CKD showing NSNPs, OR, OR (95% CI) and P value. CI, confidence interval; OR, odds ratio.

A forest plot about causal associations between 28 causal metabolites and eGFR showing NSNPs, OR, OR (95% CI) and P value.

A forest plot about causal associations between 13 causal metabolites and UACR showing SNPs, OR, OR (95% CI) and P value.
Following multiple-testing correction, a single robust association (IVW, P < 1.03E-4) was identified for eGFR, specifically with N-acetylornithine (P IVW = 1.51E-5). Notably, the IVW analysis indicated that N-acetylornithine significantly heightened the risk of eGFR reduction [β = 0.047; 95% confidence interval (CI): −0.068 to −0.026; P IVW = 1.5E-5]. Furthermore, alternative methods such as weighted median analysis (β = 0.048, 95% CI: −0.068 to −0.027, P = 5.77E-6) and MR-Egger analysis (β = 0.052, 95% CI: −0.079 to −0.025, P = 1.5E-3) consistently supported these findings. In addition, a reverse MR analysis was conducted, revealing no causal link between eGFR and N-acetylornithine. Consequently, the study’s findings offer compelling evidence for a causal association between N-acetylornithine and CKD, thereby confirming the reliability of the results.
However, by intersecting the serum metabolites derived from the three analyses, a metabolite of potential significance across all three phenotypes was identified, which is mannose. The relationship between mannose and 3 CKD phenotypes are shown in Fig. 6.
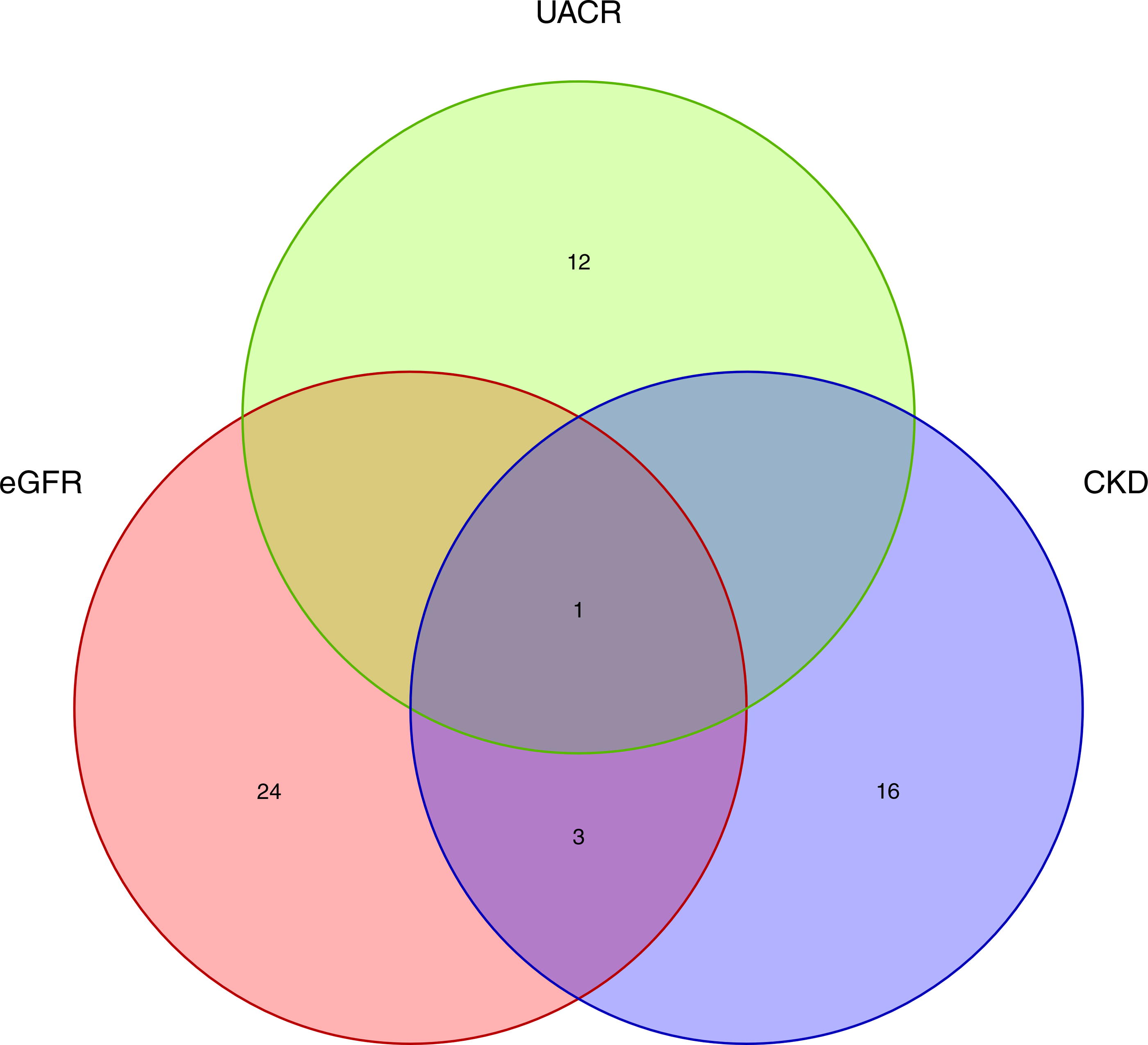
Venn plot for the crossover of three phenotypic metabolites-mannose.
Sensitivity
Although the IVW method is highly effective in establishing causal relationships between an exposure and a disease outcome, it is susceptible to weak instrument bias. To ensure the robustness of the findings, additional sensitivity and pleiotropy analyses were conducted.
The sensitivity analyses result for N-acetylornithine on the eGFR is shown in Tables 2–4. In the case of the IVW method, the Cochran’s Q statistic yielded a value of 22.0 (P = 0.232). Similarly, for the MR-Egger method, the Cochran’s Q statistic was 21.49 (P = 0.205). These results from the Cochran’s Q test indicate minimal heterogeneity within the data.
Upon examining the relationship between IVs and results, no significant intercept was found [intercept = 0.0005, Standard Error (SE) = 0.0008, P = 0.54]. In addition, the MR-PRESSO analysis revealed no evidence of horizontal pleiotropy, as demonstrated by the absence of any noticeable asymmetry in the funnel plot. These findings indicate the absence of heterogeneity and horizontal pleiotropy in our MR study, reinforcing the reliability of the causal effect of N-acetylornithine on eGFR. Notably, all metabolites that successfully passed all sensitivity analyses (P < 0.05). Furthermore, the MR-Egger regression analysis, which aimed to assess the presence of horizontal pleiotropy for the 61 associated metabolites, revealed no remarkable intercept. Consistent with these results, the Cochran’s Q test indicated minimal heterogeneity. Details can be found in Table 8.
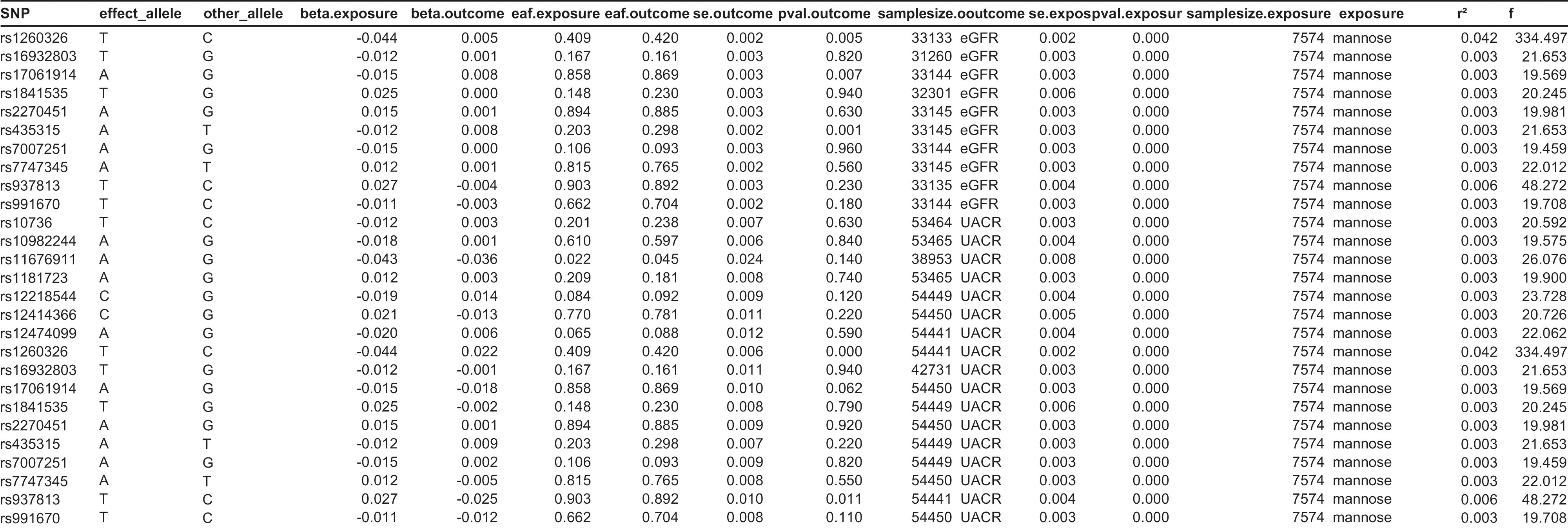
Information About SNPs of N-Acetylornithine and Mannose



Evaluation of genetic correlation and directionality
Regarding the LDSC, owing to limitations of the exposure and outcome database, some metabolite scores could not be calculated. In addition, a reverse MR analysis had been previously conducted. Taking into account the results from both methods, it is suggested that the LDSC results may serve as supplementary references rather than as definitive evidence. LDSC-based estimates noted little genetic correlation observed between our blood metabolites and three CKD phenotypes except for CKD and X-13549 (RG = −1.52, SE = 0.68, P = 0.03), eGFR and urate (RG = −0.43, SE = 0.17, P = 0.01), kynurenine (RG = −0.23, SE = 0.09, P = 0.01), choline (RG = −0.63, SE = 0.28, P = 0.02), N-acetylornithine (RG = −0.79, SE = 0.35, P = 0.03), X-12244–N-acetylcarnosine (RG = −0.62, SE = 0.24, P = 0.01). The MR Steiger directionality test results confirmed the accuracy of our causal inference (P < 0.001). Details can be found in Table 5.
Colocolization and drug target analysis
The colocalization analysis results are predominantly contingent upon PPH4, which indicates the likelihood of shared genetic predispositions at the SNP level for both exposure and outcome. Specifically, for N-acetylornithine, the PPH4 posterior probability was 85.1% for its association with CKD and 99.4% for eGFR, suggesting a strong genetic correlation.
Four common SNPs [minor allele frequency (MAF) > 1%] in low linkage disequilibrium (R 2 < 0.30), significantly associated with N-acetylornithine, were identified within ±100 kb of the NAT8 region (P < 5E-8). Furthermore, IVW-MR analysis revealed a positive association between NAT8-mediated N-acetylornithine and CKD [odds ratio (OR) = 1.43, 95% CI: 1.20–1.70, P = 4.7E-5) and eGFR (β = −0.04, 95% CI: −0.02 to −0.06, P = 1.13E-31), underscoring the importance of NAT8 in kidney function regulation.
These findings were robust to sensitivity analyses and free from pleiotropy, confirming the reliability of the results. Results are shown in Fig. 7.

Metabolic pathway analyses
The metabolic pathway analyses revealed the identification of two crucial metabolic pathways that are primarily involved in the development of CKD. The findings indicated that the “Glyoxylate and dicarboxylate metabolism” pathway displayed potential relevance to the development of CKD (P = 0.0006, FDR = 0.028). In addition, the “glycine, serine and threonine metabolism” pathway was identified as being associated with CKD by general practitioners (P = 0.0007, FDR = 0.028). Results are shown in Fig. 8.

Enriched significant metabolic pathways of CKD.
Discussion
In this two-sample MR study, 61 causal relationships for three CKD phenotypes were identified, all of which passed sensitivity analyses. One relationship showed multiple statistically significant tests even after correction and was considered the most reliable marker. Another relationship was observed in all three phenotypes simultaneously, suggesting its crucial role in CKD onset and progression. In addition, two metabolic pathways associated with CKD were identified. The research approach was enhanced by incorporating colocalization methods and expression quantitative trait locus analyses to connect metabolites with genetic variants, thus advancing the identification of potential drug targets. Previous articles have been mainly limited to methodological constraints that do not allow the demonstration of a causal relationship between genetically significantly influenced serum metabolites and the progression of CKD, or to lipid 20 or proteomic studies. 19 The study offers novel insights into the interaction between genes and the environment in the development of CKD, thereby deepening the understanding of its etiology. The findings indicate potential metabolic targets and the gene target NAT8 23 as therapeutic targets for CKD, suggesting that the condition could be prevented and improved with long-term treatment.
In the amino acid or peptide pathway, 13 amino acids and three peptides have been identified as causally associated with the development of CKD. Among them, three are considered protective factors: betaine, hydroxyisovaleroyl carnitine, and asparagine. The remaining amino acids and peptides are classified as risk factors for CKD. These include N-acetylornithine, 4-acetamidobutanoate, glycine, citrulline, γ-glutamylglutamine, valine, urea, kynurenine, homocitrulline, 3,4-dihydroxybutyrate, N-acetylcarnosine, γ-glutamylvaline, and ADpSGEGDFXAEGGGVR*. It is worth noting that in the African American population, N-acetylornithine has been identified as an important factor in the development and progression of CKD. This was demonstrated through RCTs showing a reduction in GFR. 23 In a cross-sectional study, it was observed that valine and asparagine were significantly elevated in patients with diabetic nephropathy. Valine was predicted to be associated with a rapid decline in eGFR and was identified as an independent risk factor for CKD. In contrast, the exploration of the role of asparagine was limited owing to constraints inherent in the study methodology itself. 42 In patients with hepatorenal dysfunction in cirrhosis, it has been observed that 4-acetamidobutanoate is significantly elevated. However, its specific role in CKD requires further in-depth study and investigation. 43 The decreased renal function has been found to be associated with alterations in microbial composition, glycine metabolism, and polyamine metabolism, which can contribute to renal fibrosis. In addition, hypertension has shown a strong positive correlation with dysregulation of glycine metabolism and microbiota. 44 Previous literature has confirmed that citrulline serves as a marker of renal metabolism and is associated with the development of CKD. This association has been established through urinary isotope dilution studies. However, the literature has not yet been able to identify the specific antecedents or precursors of citrulline in relation to CKD. 45 Betaine has been observed to have beneficial effects in improving renal fibrosis in patients with CKD. Its mechanisms of action are attributed to its anti-inflammatory and antioxidant properties. 46 In an MR study, it was found that an obesity-induced increase in blood urea levels is a risk factor for CKD. This suggests that elevated blood urea, which can be influenced by obesity, contributes to the development of CKD. 47 The kynurenine pathway, which is the primary metabolic pathway for tryptophan degradation, has been found to be positively associated with the development of new-onset CKD and poor renal prognosis. This pathway is considered a risk factor for CKD, likely because of its promotion of renal fibrosis. These findings have been consistently observed in three large-cohort longitudinal studies. 48 –50 In metabolomics studies, N-acetylcarnosine, homocitrulline, and γ-glutamylvaline have been identified as risk factors for CKD progression. However, it is important to note that these studies have not established a causal relationship between these metabolites and the progression of CKD. Although they have shown an association, further research is needed to determine the underlying mechanisms and establish causation. 51 –53 Studies of hydroxyisovaleroyl carnitine, γ-glutamylglutamine, 3,4-dihydroxybutyrate, and ADpSGEGDFXAEGGGVR* in CKD are still lacking and need to be initiated.
In the lipid pathway, 10 lipids were identified as being causally associated with the development of CKD. Four of them are protective factors: lathosterol, 1-linoleoylglycerophosphoethanolamine*, 1-oleoylglycerophosphoethanolamine, and 1-eicosatrienoylglycerophosphocholine*. The others are risk factors, which include stearate (18:0), choline, 1-linoleoylglycerol (1-monolinolein), dehydroisoandrosterone sulfate (DHEA-S), 5-dodecenoate (12:1n7), and X-12442–5,8-tetradecadienoate. Lathosterol is a marker of cholesterol synthesis. In two case–control studies, it was found that populations with lower eGFR had lower levels of lathosterol, and lathosterol was associated with higher eGFR. However, neither of these studies discussed the relationship between lathosterol and the development of CKD. 54,55 Deposition of lipids, such as stearate (18:0), in the kidneys has been implicated in the progression of inflammation in the kidneys. 56 Choline, which is produced by the gut microbiota, has been found to be associated with the onset and progression of CKD. However, many aspects of this association still need to be further investigated and clarified. 57 It has been found in a network pharmacology study that 1-monolinolein was identified as one of the key targets for the treatment of diabetic nephropathy. However, its role in the progression of CKD development has not yet been extensively studied or focused on. 58 The observation that patients with CKD often have lower levels of DHEA-S and are associated with increased mortality may appear contradictory to our findings. However, the existing literature does not extensively discuss or study the relationship between DHEA-S and the development of CKD in healthy individuals. Therefore, the causal relationship between DHEA-S and the development of CKD remains unclear and requires further investigation. 59,60 The role played by 1-linoleoylglycerophosphoethanolamine, 1-oleoylglycerophosphoethanolamine, 1-eicosatrienoylglycerophosphocholine*, 5-dodecenoate (12:1n7), and X-12442–5,8-tetradecadienoate in the development and progression of CKD has not been addressed by studies.
In the carbohydrate pathway, six carbohydrates and one energy-related component have been identified as causally associated with the development of CKD. Among them, three are identified as protective factors: glycerate, malate, and glucose. In addition, there are three risk factors: mannitol, 1,5-anhydroglucitol (1,5-AG), and erythronate*. The effect value of mannose differed among the three outcomes and was a bidirectional factor for CKD. The fact that malate is a protective factor in CKD seems to contradict the previous finding in the literature that tricarboxylic acid pathway metabolites, such as malate, are elevated in patients with CKD. However, the previous literature is deficient in that only correlations can be made, and no analytical studies have been carried out to argue for causality. 61,62 Glucose has been shown to be a high risk factor for kidney failure in diabetic nephropathy, thus seemingly contradicting our results. However, since not all of our patients with CKD were because of diabetic nephropathy, the results are still valid, and further stratification of the sample is needed to explore the role in renal diseases other than diabetic nephropathy as well as in CKD. Another possible explanation is that the relationship between glucose and outcome is nonlinear and therefore within a certain range our results are worth referring to, as glucose is the main substance for tubular energy supply. Mannose is analyzed in eGFR and UACR with opposite effects on CKD, whereas it is an important substance for complement activation and may have a dual role in the progression of CKD, which is worth exploring. 63,64 Mannitol dilates renal blood vessels and is associated with contrast-induced nephropathy, but the exact mechanism remains unexplored. 65 Recent studies have shown that 1,5-AG can improve the performance of patients with CKD by inhibiting oxidative stress and inflammation to attenuate renal fibrosis. 66 Glycerat has been shown to reduce the risk of CKD. 52 Erythronate can be used as a serum metabolite for estimating GFR, but the association with CKD is not clear. 67
In addition, it was found that urate, part of the nucleotide pathway, acts as a risk factor, whereas salicyluric glucuronide, which belongs to Xenobiotics, serves as a protective factor. In addition, bilirubin (Z,Z), belonging to the cofactors and vitamins pathway, is also identified as a protective factor. Urate has been recognized as a risk factor for CKD in observational studies. However, an MR article demonstrated that there does not seem to be a causal relationship between urate and CKD. To further investigate this matter, this article aims to explore the association between urate and decreased eGFR, which clarifies the inconsistent conclusions found in experimental studies and previous MR studies. 68,69 Previous observational and MR studies have consistently identified bilirubin as a protective factor against the development and progression of CKD. The findings correspond with prior studies, underscoring the necessity for additional research to elucidate the precise mechanisms through which bilirubin provides its protective effects in CKD. Understanding these mechanisms in depth will provide valuable insights into potential therapeutic interventions for CKD. 70 –72 Salicyluric glucuronide* in the development and progression of CKD has not been addressed by studies.
Moreover, 10 protective factors and 9 risk factors were found but are unknown material which deserve to be explored in depth.
The strength of our study is that it provides a more comprehensive summary of the relationship between 486 genetically influenced blood metabolites and the onset and development of CKD. Many findings in the literature support our findings, which adds much credibility to the article. These metabolites are potential CKD risk factors or protective factors, especially several metabolites that are directly causally related to the development of CKD. Their mechanisms in the development of CKD deserve to be further explored, and they can also be tried as predictors of CKD development. Those associated with eGFR and UACR, in contrast, are likely to play an important role in the development of CKD and deserve further exploration for their value as indicators of CKD progression and prognosis.
However, this study has several limitations. First, the GWAS data were not stratified based on the primary cause of CKD, despite multiple causes being involved. Second, the sample primarily consisted of a European population, necessitating validation through expansion to other ethnicities. Third, the effect values obtained through MR do not indicate the direct benefits from interventions as the genetic variant’s impact on exposure is a long-term effect. Fourth, owing to limited data availability, the study used metabolites with uncorrected p values for pathway analysis, which may introduce biases or incomplete understanding of underlying mechanisms. Lastly, although the study identified metabolites associated with the risk of CKD, further research is required to elucidate their specific roles in the pathogenic mechanisms of CKD.
In recent years, the role of chronic low-grade inflammation in the development and progression of CKD has gained recognition. Serum metabolites, such as peptides, lipids, and glycans, have been discovered to serve as either proinflammatory or anti-inflammatory mediators within the realm of chronic inflammation. 73 –75 Furthermore, CKD is typically considered irreversible and tends to worsen over time. To address this, advanced MR methods were utilized to identify both risk and protective factors associated with the onset of CKD. MR studies have emerged as a burgeoning trend in drug target identification, offering enhanced preclinical preparation for clinical pharmacological research. 76 This approach ensures that resources are allocated to potential drug targets with a higher likelihood of success. In an RCT, a site mutation in NAT8 was linked to adverse outcomes in African American patients with CKD. 23 The study, which included a European population, supports the potential efficacy of NAT8 as a drug target, thus paving the way for further investigation. MR studies targeting drug interventions for CKD are relatively scarce. Current examples include GLUT9 inhibitors, 77 which protect the kidneys by lowering uric acid levels, and SLC13A5 inhibitors, where plasma calcium and citrate serve as biologically plausible target biomarkers. 76
The MR research conducted in this study identified 61 causal relationships that are potentially linked to the pathogenesis of CKD. Significantly, N-acetylornithine has been identified as having a substantial influence on CKD. Consequently, colocalization analyses were conducted, and the effects of NAT8-mediated N-acetylornithine on CKD and eGFR were examined to strengthen the evidence supporting its potential as a drug target. The study also highlighted two metabolic pathways that are likely relevant to the pathology of CKD. These findings offer valuable insights into the use of certain metabolites as potential biomarkers for exploring targeted drugs in the treatment of human diseases. However, further research is warranted to elucidate the specific mechanisms by which these metabolites contribute to either adverse or favorable outcomes, and the associated drug research is deemed worthy of investment.
Footnotes
Acknowledgment
The authors would like to thank Mr. Guozi for his support in programming skills and Mr. Yiyu for his advice on code and essay writing.
Authors’ Contributions
Research idea and study design: Z.Z. and B.C.; data acquisition: Z.Z.; data analysis/interpretation: Z.Z., B.C., and Q.W.; statistical analysis: Z.Z., B.C., and Q.W.; supervision or mentorship: Z.Z. and Q.W. Each author contributed important intellectual content during article drafting or revision and accepts accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved.
Study Approval Statement
No more ethical approval was required for this study because it was a secondary analysis based on publicly available datasets. The original studies have obtained local ethical approvals and informed consent from the participants.
Data Availability Statement
Author Disclosure Statement
No conflicting financial interests exist.
Consent to Participate Statement
Patient consent was not required as this study was based on publicly available data. All participants provided informed consent in their corresponding original studies, as described in the Methods section.
Funding Information
This study was not supported by any sponsor or funder.