
Abstract
Lipid disorders are related to the risk of nonalcoholic fatty liver disease (NAFLD). Remnant cholesterol (RC), a nonclassical and once-neglected risk factor for NAFLD, has recently received new attention. In this study, we assessed the relationship between the RC levels and NAFLD risk. We searched across PubMed, Web of Science, Embase, Cochrane Library, and China National Knowledge Infrastructure, with no restrictions on publication languages. Retrospective cohort studies and cross-sectional studies were enrolled from the inception of the databases until August 6, 2023. A random-effect model was applied to construct the mean difference, and a 95% confidence interval was applied to assess the relationship between the RC levels and NAFLD risk. We used two methods to estimate RC levels: Calculated-1 subtracts low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol from total cholesterol; Calculated-2 uses the Friedewald formula for LDL-C when triglycerides are <4.0 mmol/L, otherwise directly measured. A total of 265 published studies were selected through preliminary retrieval. Of these, six studies met the inclusion requirements and were enrolled in the meta-analysis. The RC level in the NAFLD group was significantly higher than that in the non-NAFLD group (mean difference: 0.18, 95% confidence interval: 0.10–0.26, P < 0.00001). We conducted subgroup analyses of computational methods and geographic regions. Notably, in the subgroup analysis of Calculation Method 2, the NAFLD group had significantly higher RC levels than the non-NAFLD group. On the other hand, in Calculation Method 1, the difference between the two groups was insignificant. In both the Asian and non-Asian populations, the RC levels were significantly higher in the NAFLD group than in the non-NAFLD group. The association of RC with an increased NAFLD risk was not dependent on the triglyceride. This meta-analysis suggests that elevated RC levels are associated with an increased risk of NAFLD. In addition to the conventional risk factors for fatty liver, clinicians should be concerned about the RC levels in the clinic.
Introduction
Nonalcoholic fatty liver disease (NAFLD) is a group of diseases associated with metabolic dysfunction of the liver, which is characterized by excessive accumulation of intrahepatic lipid accumulation. 1 NAFLD is the most common chronic liver disease worldwide, with a prevalence rate of 30.1%. 2 In fatty liver, fat is deposited in the liver, and NAFLD can progress to nonalcoholic steatohepatitis at an early stage, which can further lead to cirrhosis and hepatocellular carcinoma. 3,4 The pathogenesis of NAFLD is complex, with patients predominantly having obesity, type 2 diabetes mellitus, hypertriglyceridemia, and low high-density lipoprotein (HDL) levels. 5 –7 Dyslipidemia is an important factor in the development of NAFLD. Only a few studies have reported the roles of different types of dyslipidemia in the occurrence and development of NAFLD, and these findings are inconsistent. Elevated low-density lipoprotein cholesterol (LDL-C) levels are associated with an increased risk of developing NAFLD. 8 Furthermore, increased very low-density lipoprotein (VLDL) secretion has been recorded in patients with NAFLD. 9
Remnant cholesterol (RC) is defined as the cholesterol content of the remnants, which are a subset of cholesterol-rich lipoproteins. These include celiac remnants, VLDL, and intermediate-density lipoprotein. RC is commonly calculated as total cholesterol minus LDL-C minus HDL cholesterol (HDL-C). 10 RC is larger and carries more cholesterol on a per particle basis than LDL-C particles. 11 A significant risk of NAFLD was still observed, although the goal of an LDL-C in the normal range was achieved in the trial using exercise methods and medications. 12 –14 RC can lead to cardiovascular damage through the induction of oxidative stress, lipid deposition, inflammation, and accelerated endothelial damage. 15,16 A small study from the United Kingdom revealed that RC was related to elevated liver transaminase levels in adolescents with NAFLD. 14 Therefore, RC was considered as a potential risk factor for increased risk of NAFLD. However, whether elevated RC increases the risk of NAFLD remains inconclusive. 17,18 Although RC was previously overlooked as a potential risk factor for NALFD, it has recently attracted attention in this respect. Accordingly, we conducted a meta-analysis including all clinical trials to further substantiate the relationship between RC levels and the risk of NAFLD.
Materials and Methods
Protocol and registration
A standard protocol was developed in accordance with the Preferred Reporting Items for Meta-Analyses guidelines. 19 The protocol of this meta-analysis has been registered in PROSPERO (CRD42023458439).
Search strategy and study selection
We searched the Web of Science, Embase, PubMed, China National Knowledge Infrastructure, and Cochrane library databases from inception until August 6, 2023. There were no restrictions on the language of publication. Conference abstracts were manually searched to discover potentially eligible studies. A search strategy was listed as follows: (“Nonalcoholic Fatty Liver Disease” [All Fields] OR “NAFLD” [All Fields]) OR (“NASH” [All Fields] OR “Nonalcoholic Steatohepatitis” [All Fields]) AND (“Remnant cholesterol” [All Fields] OR “residual cholesterol” [All Fields] OR “RLP-C cholesterol” [All Fields]).
Inclusion and exclusion criteria
Inclusion criteria: (i) original articles explored the relationship between NAFLD/nonalcoholic steatohepatitis (NASH) and RC, (ii) retrospective cohort studies and cross-sectional studies, and (iii) age and sex were not limited.
Exclusion criteria: (i) conference abstracts, letters, reviews, and meta-analyses; (ii) duplicate studies; (iii) experimental studies; (iv) editorials/comments and case reports; (v) studies with no relevant data; and (vi) original articles including patients with NAFLD, but competing with steatosis and other coexisting causes of chronic liver disease (e.g., heavy alcohol consumption, hepatitis C, and drugs).
Study selection
The relevant studies were independently screened by two reviewers (J.-K.T. and C.L.) based on the titles and abstracts. If the studies were found to be potentially eligible, full texts were further read and screened. Any disagreements were resolved via mutual discussion between the two reviewers. We reviewed all the study characteristics (i.e., year of publication, the first author’s surname, study design, sample, NAFLD detection methods, and outcomes). We also collected data on specific methods used to either measure or estimate RC in each study. The indirect methods for estimating RC were as follows: (i) indirect method used to estimate RC by calculating total RC (mg/dL) = TC (mg/dL)-HDL-c (mg/dL)-LDL-c (mg/dL); irrespective of the level of triglycerides (TG), LDL-C was measured directly, and (ii) indirect method used to estimate RC by calculating total RC (mg/dL) = TC (mg/dL)-HDL-c (mg/dL)-LDL-c (mg/dL). LDL-C was calculated using the Friedewald equation when plasma TG were <4.0 mmol/L; otherwise, it was measured directly. The review protocol is available at www.crd.york.ac.uk/PROSPERO, identifier: CRD42023458439. No ethics approval was required.
Statistical analysis
The correlation between the RC levels and NAFLD/NASH risk was assessed. For continuous data, the mean difference (MD) with 95% confidence interval (CI) was calculated using the inverse variance statistical method. Data were combined using a random-effects model to obtain the conservative estimates. The I 2 statistic and Q-test were employed to measure heterogeneity between the included studies, where I 2 > 50% and P < 0.1 were considered to indicate significant heterogeneity. If more than five eligible studies were included in a meta-analysis, we employed funnel plots to assess any publication bias. All statistical analyses were performed using Review Manager 5.4 software.
Results
Outcomes of the electronic search
We searched the PubMed, Web of Science, Embase, China National Knowledge Infrastructure, and Cochrane Library databases and screened the references of the retrieved published studies. The retrieval deadline was August 6, 2023. The search words included “Nonalcoholic fatty liver Disease (NAFLD)” and “remnant cholesterol (RC),” and the search language was not restricted. In the preliminary retrieval, 265 studies were obtained, of which 179 were duplicated studies, 15 were reviews or letters, 20 were basic, and 45 were studies with irrelevant or no relevant data; hence, these studies were excluded. Through thorough reading of the texts, six studies were found to conform to the inclusion requirements and were therefore included in the meta-analysis [35,064 participants (10,712 patients with NAFLD)]. All studies were included in the meta-analysis of the relationship between the RC levels and NAFLD risk (Fig. 1).
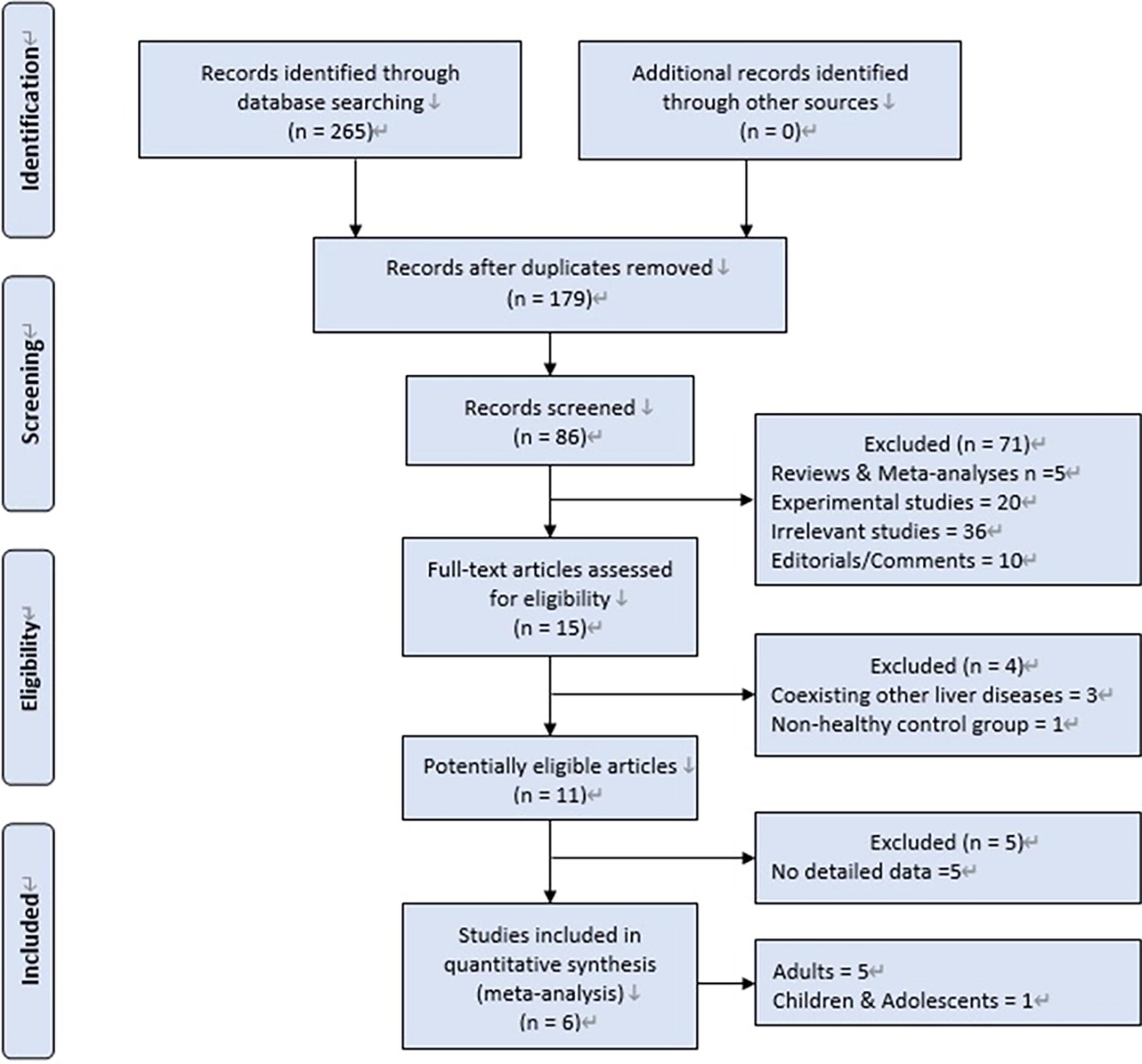
Literature screening flowchart.
Characteristics of the included studies
The characteristics of all studies are summarized in Table 1. 20 –25 These studies were included in pooling the relationship between the RC levels and NAFLD risk. Among the included studies, there were two cross-sectional studies and four cohort studies. Of them, three studies were from China, and one study each from the USA, Japan, and Australia. All included studies described the number of patients without and with NAFLD. Accordingly, 10,712 patients were included in the NAFLD group and 24,352 in the non-NAFLD group. Four studies recorded the median and quartiles of RC, and two studies recorded the mean and standard deviation of RC. Five studies utilized liver ultrasound to diagnose NAFLD, while one study employed transient elastography of the liver for diagnosis. Regarding the calculation method for RC, two studies adopted the Calculation-1 method, and four studies utilized the Calculation-2 method.
Characteristics of Included Studies
Indirect method was used to estimate RC by calculating total RC (mg/dL) = TC (mg/dL)-HDL-c (mg/dL)-LDL-c (mg/dL); regardless of the level of triglycerides, LDL-C was measured directly.
Indirect method was used to estimate RC by calculating total RC (mg/dL) = TC (mg/dL)-HDL-c (mg/dL)-LDL-c (mg/dL). LDL-C was calculated using the Friedewald equation when plasma triglycerides were <4.0 mmol/L; otherwise, it was measured directly.
HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; NAFLD, nonalcoholic fatty liver disease; RC, remnant cholesterol.
Meta-analysis
The RC level in the NAFLD group was significantly higher than that in the control group (MD: 0.18, 95% CI: 0.10–0.26, P < 0.00001) (Fig. 2). RC showed a better predictive value for assessing the condition of patients with NAFLD. The funnel plot indicated that the included studies were symmetrically distributed on both sides of the midline, with no significant publication bias (Fig. 3).
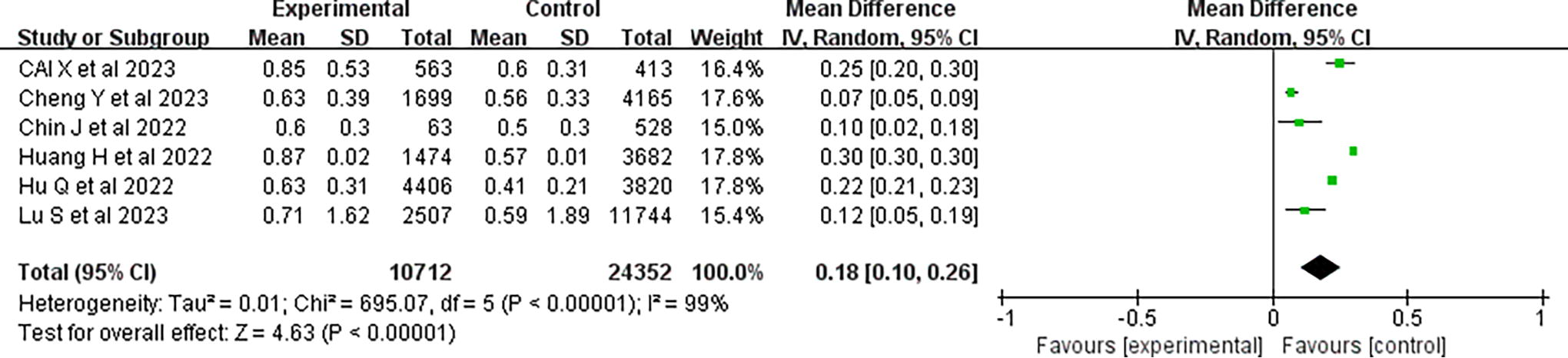
Forest plot comparing RC values between NAFLD patients and controls (random-effects model, MD). MD, mean difference; NAFLD, nonalcoholic fatty liver disease; RC, remnant cholesterol.

Filled funnel plot based on the result of elevated RC levels is associated with an increased risk of NAFLD.
Several methods are available for measuring RC. We analyzed the subgroups of different methods. In the subgroup analysis of Calculation-2, the RC levels were higher in the NAFLD group than in the non-NAFLD group, with an overall MD of 0.20 (95% CI: 0.13–0.26). In the subgroup analysis of Calculation-1, the RC levels were not significantly different between the NALFD and non-NAFLD groups, with an overall MD of 0.16 (95% CI: −0.02 to 0.33) (Fig. 4).

Forest plot of circulating RC levels correlated more with NAFLD in the Calculated-2 subgroup than in the Calculated-1 subgroup.
Considering dietary and environmental impacts on individuals, we analyzed the subgroups across geographic regions. In a subgroup analysis of the Asian population, RC levels were significantly higher in the NAFLD than in the non-NAFLD group, with an overall MD of 0.17 (95% CI: 0.07–0.26). In the subgroup of non-Asian populations, the RC levels were significantly higher in the NAFLD group than in the non-NAFLD group, with an overall MD of 0.20 (95% CI: 0.01–0.40). No significant differences were noted in the RC levels between the Asian and non-Asian regions (Fig. 5).

Forest plot of circulating RC levels between NAFLD and the healthy control group, subgroup analysis divided into Asian and non-Asian according to region (random-effects model, MD).
Considering the interference of TG on lipid levels, we analyzed subgroups with different TG levels. In the subgroup analysis of TG ≥1.7 mmol/L, RC levels were significantly higher in the NAFLD group than in the non-NAFLD group, with an overall MD of 0.28 (95% CI: 0.24–0.33). In the TG <1.7 mmol/L subgroup, RC levels were significantly higher in the NAFLD group than in the non-NAFLD group, with an overall MD of 0.08 (95% CI: 0.05–0.10) (Fig. 6).
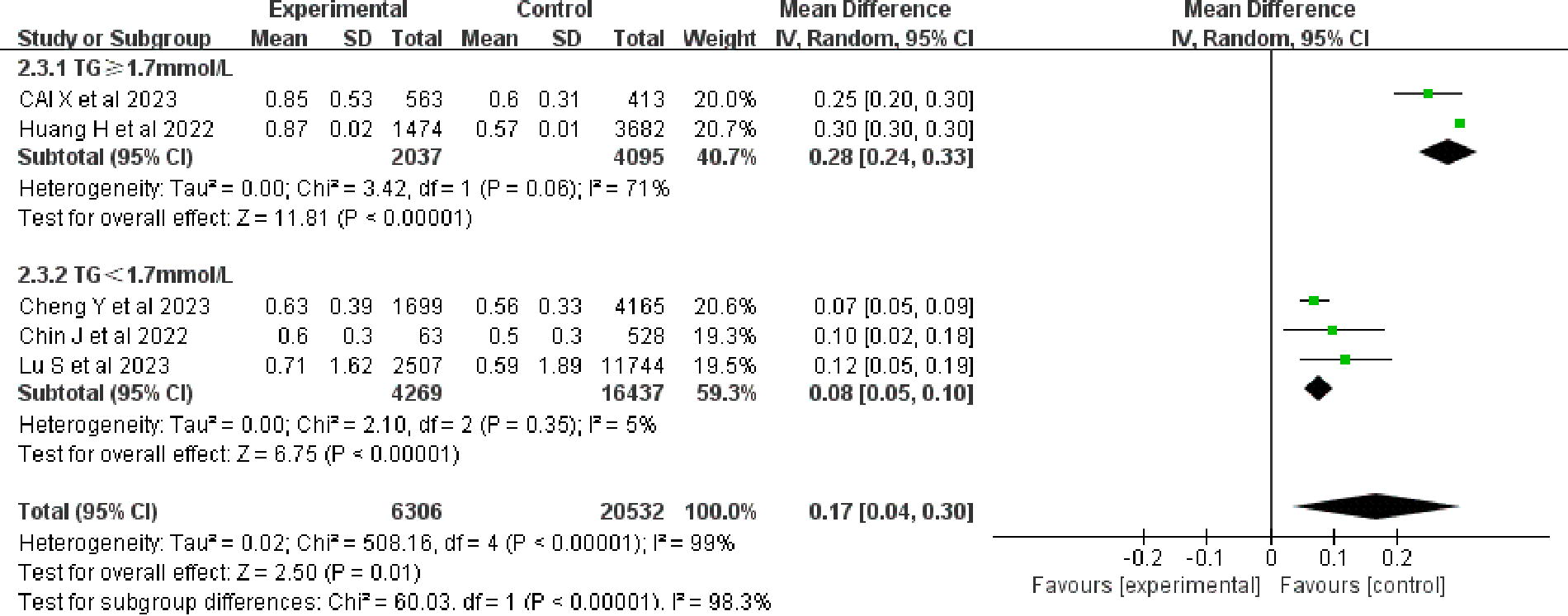
Forest plot of circulating RC levels between NAFLD and healthy controls, subgroup analysis according to TG ≥1.7 mmol/L and TG <1.7 mmol/L (random-effects model, MD). TG, triglycerides.
Discussion
We analyzed data from 35,064 individuals to assess the relationship between the RC levels and the risk of NAFLD. The association between RC levels and cardiovascular disease, stroke, and all-cause mortality has been previously demonstrated in meta-analyses. 26,27 However, none of these studies discussed the relationship between RC levels and NAFLD risk. To the best of our knowledge, this is the first meta-analysis to demonstrate an association between RC levels and NAFLD risk. Our results are similar to those of previous studies. Yuan et al.’s study indicated a relationship between NAFLD and TG (OR: 1.23, 95% CI: 1.15–1.33 per standard deviation increase). 28 Previously, Varbo provided a biologically effective way of treating NAFLD with statins. 29 In the subgroup analysis in the present study, the geography and TG levels did not affect the relationship between the RC levels and NAFLD risk.
RC can be obtained in a variety of ways and categorized as direct or indirect determinations. Direct determination includes ultracentrifugation, agarose gel electrophoresis, or immune separation. 30 However, these methods are expensive and time-consuming. Therefore, they are less applied in clinical practice. 31 Presently, RC is calculated based on the standard lipid profile: (i) the indirect method is used to estimate RC by calculating total RC (mg/dL) = TC (mg/dL)-HDL-c (mg/dL)-LDL-c (mg/dL); regardless of the level of TG, LDL-C was measured directly, and (ii) the indirect method was used to estimate RC by calculating the total RC (mg/dL) = TC (mg/dL)-HDL-c (mg/dL)-LDL-c (mg/dL). LDL-C was calculated using the Friedewald equation when the level of plasma TG was <4.0 mmol/L; otherwise, it was measured directly. 29,32 We performed a subgroup analysis of the two methods and observed that studies employing Calculation-1 did not show a significant association between the RC levels and the risk of NAFLD, possibly attributable to the insufficient number of studies incorporating this calculation method. In the studies that utilized Calculation-2, a modified Friedewald formula was used to calculate the LDL cholesterol, and a significant link between the RC levels and NAFLD risk was detected. However, Lin’s team reported no significant difference between the direct measurement of LDL-C and the Friedwald formula. 33 The outcomes of Calculation Method 2 are still influenced by the TG levels. Calculating RC using the Friedewald formula demonstrates notable flexibility and operability and is, hence, currently feasible. However, we recommend the Calculated-1 method, which is also recommended by the 2019 European Atherosclerosis Society Guidelines for the Management of Dyslipidemia. 10 However, this step necessitates the inclusion of more studies employing Calculation Method 1 for NAFLD research. The clinical monitoring of nonfasting RC levels may be relatively complicated currently as the results depend not only on the acquisition method of RC but also on the evaluation method.
The underlying mechanisms of how RC affects the development of NAFLD are unknown, and some of the possible mechanisms include, delayed TG metabolism leading to increased RC levels. 34 Chylomicrons and VLDLs are believed to be derivatives of RC and are produced in the liver and small intestine, respectively. 35 Lipoprotein lipase plays a decisive role in the catabolism of Triglyceride-rich lipoproteins, as it reduces the activity leading to decreased Triglyceride-rich lipoproteins clearance. 34 The activation of lipoprotein lipase is effective in reducing the severity of NAFLD. 36 Moreover, inflammation plays an important role in the pathogenesis of NAFLD. 35 Several studies have linked RC to low inflammatory markers. 37 –39 We accordingly hypothesized that RC affects NAFLD through inflammatory pathways. Since the early stages of NAFLD are reversible, there is an urgent need for early detection and intervention methods. RC is now recognized as a promising biomarker for assessing cardiovascular risk independent of other lipids. 40 A study including 5156 people found that patients with NAFLD with high RC levels had a higher risk of dying from cardiovascular diseases. These findings demonstrate the importance of measuring the RC levels in patients with NAFLD. The present study indicates a correlation between RC and NAFLD, thereby providing an evidence-based basis for clinicians to determine NAFLD by assessing the RC levels.
NAFLD is highly prevalent in all continents, and the highest rates are reported from the Middle East (32%), followed by Asia (27%) and the USA (24%). 41 Moreover, the cholesterol levels differ between Asian and Western countries. Non-HDL-C is elevated in Asian countries, and most Western countries have increased HDL-C and decreased non-HDL-C. 42 Considering that cholesterol and NAFLD are geographically distinct, we performed subgroup analyses and found that the RC levels did not differ significantly between Asian and Western countries in the NAFLD population. LDL-C tends to increase in Asian countries as the calorie intake increases with economic development. In Western countries, cholesterol tends to decrease with improved dietary structure, with a gradual convergence between them. 41
Nonetheless, there are several limitations to our study. First, the study sample was small, as we included only six studies. Second, the included literature lacked specific data for analysis, such as sex, age, and underlying disease. As such, additional subgroup analyses could not be performed to eliminate the impact of these confounding factors on the study findings. Third, liver biopsies and pathological indicators of patients were not collected in the included literature. Therefore, the correlation between the RC levels and pathological liver damage in NAFLD could not be confirmed.
Conclusions
In summary, lipid deposition affects the development of NAFLD, and changes in the RC levels reflect the impact of nontraditional adiposity indicators on the condition of patients with NAFLD, implying that RC has a good predictive value for evaluating the condition of patients with NAFLD.
Footnotes
Authors’ Contributions
X.Z., M.W., and F.T. contributed to conceptualization (lead) and writing—original draft (lead). J.T., T.T., and Q.Y. performed data curation, analysis, data visualization, and writing. X.T., C.L., C.C., S.H., and S.Z. assisted with conceptualization (supporting), development and design of methodology, and reviewing and editing. Y.Y., C.W., J.L., W.W., and J.C. supported with conceptualization (supporting), analysis supervision, and reviewing and editing.
Author Disclosure Statement
None of the authors had any financial disclosures/conflicts of interest pertaining to this study.
Funding Information
This study was supported by Medical and Technology Project of Zhejiang Province (No. 2021KY890, No. 2024KY1348, No. 2024KY200); Zhejiang Traditional Chinese Medicine Scientific Research Fund Project (No. 2022ZB280, No. 2024ZL723, No. 2019ZA093); Zhejiang Kangenbei Hospital Management Soft Science Research Project (No. 2022ZHA-KEB316); Hangzhou Medical Health Technology Project (No. 20220919Y021); Hangzhou Agricultural and Social Development Research Initiative Design Project (No. 20190101A03); Hangzhou Biomedicine and Health Industry Development Support Science and Technology Project (No. 2021WJCY238); Hangzhou Biomedicine and Health Industry Development Support Science and Technology Project (No. 2023WJC148); Interdisciplinary Research Project of Hangzhou Normal University (2024JCXK05); and Zhejiang Medical Association Clinical Research Fund Project (No. 2020ZYC-A14). The funders have no role in the data collection, data analysis, preparation of the article, or decision to submission. The work was supported by the key medical disciplines of Hangzhou.