
Abstract
Introduction:
Shift work disrupts sleep–wake cycles and may lead to adverse health outcomes, including cardiovascular disease and metabolic disorders. This study examines the association between shift work and the risks of metabolic syndrome (MetS) and circadian syndrome (CircS) in U.S. workers.
Methods:
We analyzed data from 4173 participants aged 18 and above from the National Health and Nutrition Examination Survey (NHANES) spanning 2005–2010. Shift work status was determined based on work hours, and MetS and CircS were defined using established criteria. Statistical analyses included weighted multivariate logistic regression models, weighted multivariate linear regression models, and inverse probability weighted propensity score matching to ensure accurate comparison between shift and nonshift workers.
Results:
The study found no significant association between shift work and the prevalence of MetS. However, shift workers exhibited a higher prevalence of CircS compared with nonshift workers. This association was more pronounced in specific subgroups, including those under 60 years of age and various ethnicities. The study highlights the heightened risk of CircS among shift workers, underscoring the potential impact of shift work on circadian rhythm disruptions.
Conclusion:
Shift work is associated with an increased risk of CircS but not MetS, according to NHANES 2005–2010 data.
Prior research has established that shift work can disrupt normal sleep–wake cycles and is associated with various negative health outcomes. Understanding the specific conditions associated with shift work, like metabolic and circadian syndromes, is crucial for workplace health and policy-making.
This research clarifies that although shift work does not significantly impact metabolic syndrome rates, it is associated with a higher risk of circadian syndrome. This distinction is vital for understanding and mitigating health risks in shift-working populations.
The study’s findings could inform workplace policies, health guidelines, and future research directions. By highlighting the specific risks of circadian syndrome associated with shift work, it can lead to targeted strategies for health monitoring and intervention among shift workers.
Introduction
Approximately one quarter of the global workforce engages in shift work outside of traditional working hours (7 a.m. to 6 p.m.). 1 In order to maintain essential services on a 24-hr basis, shift work is practiced in many sectors, such as health care, emergency response, and social production. 2 This work pattern disrupts the sleep–wake cycle, light exposure, and eating rhythms of employees. Consequently, shift workers experience alterations in the homeostasis of their circadian rhythms, leading to potential adverse health outcomes. 3 Those regularly engaging in irregular work schedules face an increased risk of diseases, including cardiovascular disease (CVD), cancer, and metabolic disorders. 4 Extensive research has been conducted on both the short-term and long-term health risks associated with shift work.
Previous research has indicated that shift workers may contribute to obesity and abnormal metabolic functions. Metabolic syndrome (MetS), a prevalent metabolic disorder, is often linked with the rising rates of obesity. 5 MetS encompasses several conditions: obesity, high blood pressure, dyslipidemia (characterized by high triglycerides and low high-density lipoprotein cholesterol levels), and elevated fasting glucose levels. It is recognized as the most frequent risk factor and co-morbidity for CVD. Factors like nocturnal light exposure during shift work and irregular meal timings, which disrupt the endogenous biological clock, are considered potential contributors to MetS. 6 The endogenous biological clock is involved in almost every aspect of human physiological health and metabolism. Evidence suggests that disruption in circadian rhythms is not only strongly linked to MetS but may also be an underlying cause of sleep disorders, depression, and cognitive impairments in older adults.
In 2019, Zimmet and colleagues introduced the concept of circadian syndrome (CircS), suggesting that disruptions in circadian rhythms might be a central cause of MetS and its associated co-morbidities. 7 CircS includes not only the components of MetS but also encompasses various diseases related to circadian rhythm disturbances, such as sleep disorders, depression, and nonalcoholic fatty liver disease, thus potentially offering a more comprehensive reflection of an individual’s health status. Studies on both American and Chinese populations have indicated that compared with MetS, CircS is a stronger and better predictor of CVD. 8,9 In addition, research has found that CircS is associated with multiple health issues, including cognitive dysfunction, 10,11 overactive bladder, 12 chronic kidney disease, 13 and frailty, 14 highlighting its importance as a new integrative health risk assessment indicator. Our study aimed to evaluate the association between shift work and the risks of CircS among U.S. workers.
Method
Research population
This study uses data from the National Health and Nutrition Examination Survey (NHANES), which is a national, cross-sectional survey targeting noninstitutionalized civilians across the United States. NHANES uses a multistage, stratified sampling design to collect health and nutrition information from a representative sample of the U.S. population on a 2-year cycle. Because information on shift work was only recorded in the 2005–2010 surveys, we selected participants from these three cycles for our study. Detailed information about the research design, sampling procedures, exclusion criteria, and other relevant aspects are illustrated in Figure 1.
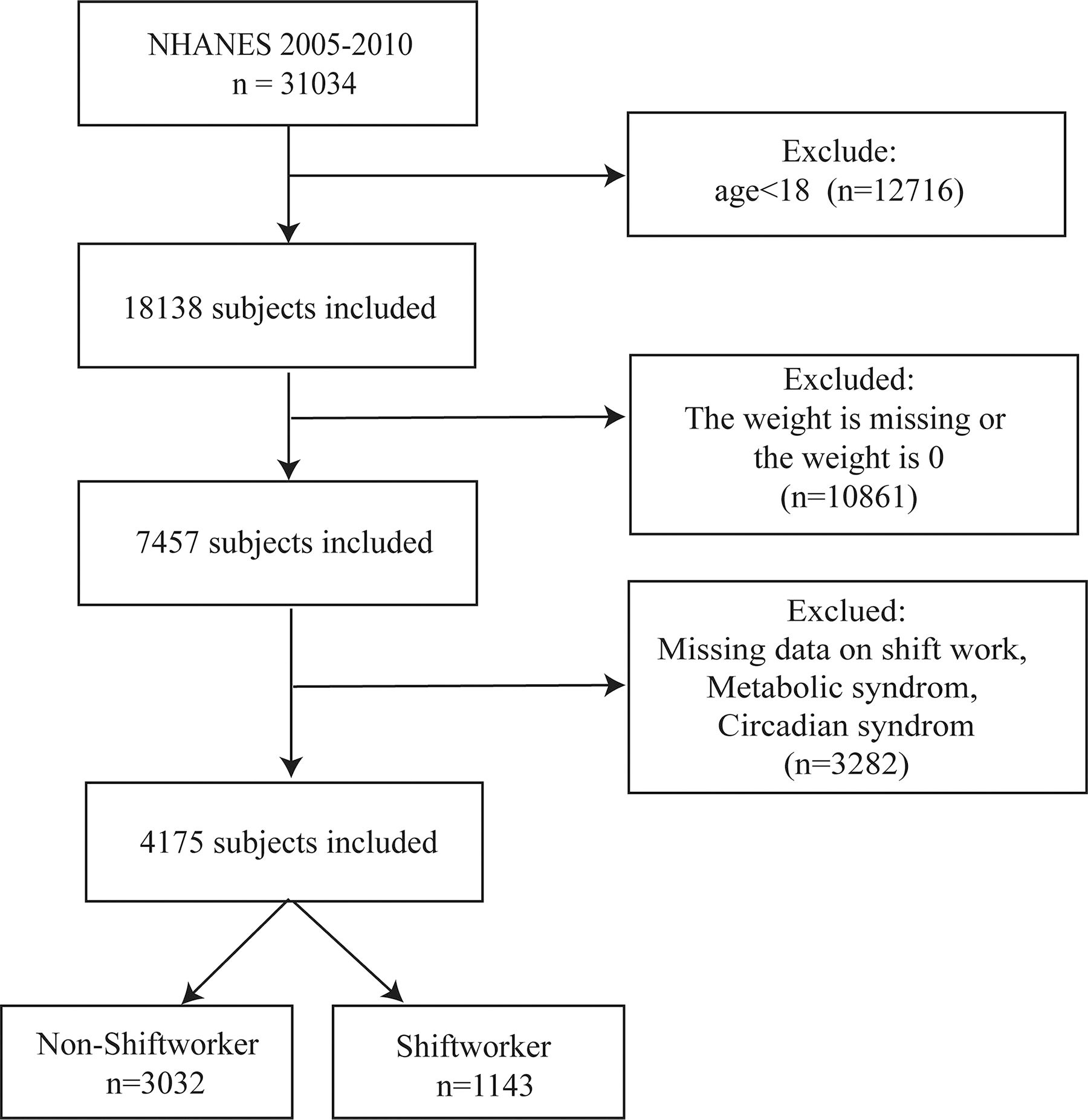
Flow chart of the study.
Shift work exposure
Shift work status was assessed by the following question, “Which best describes hours worked?” Response options included the following: (a) regular daytime, (b) evening shifts, (c) night shifts, (d) rotating shifts, or (e) another schedule. Based on previous research, we defined nonshift workers as participants whose work hours were fixed day shifts and others as shift workers. 15
Definition of MetS and CircS
MetS was defined using the harmonized criteria proposed in the joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention, National Heart, Lung, and Blood Institute, American Heart Association, World Heart Federation, International Atherosclerosis Society, and International Association for the Study of Obesity. As shown in Supplementary Table S1, participants were considered to have MetS if they included three or more components of the disorder: (1) elevated waist circumference (≥102 cm in men and ≥88 cm in women); (2) elevated triglycerides or use of lipid-modifying medications (triglycerides ≥150 mg/dL); (3) reduced low-density lipoprotein (LDL) cholesterol or use of medications that would reduce LDL; (4) hypertension or use of antihypertensive medications (systolic blood pressure ≥130 mmHg/or diastolic blood pressure ≥85 mmHg); and (5) elevated fasting glucose or use of antihyperglycemic medications.
CircS is defined by adding the components of short sleep duration and depressive symptoms to MetS. Self-reported sleep duration was considered short if ≤6 hr. Depressive symptoms were evaluated according to the Patient Health Questionnaire (PHQ-9). A diagnosis of CircS is established when any four out of these seven risk factors are present, as detailed in Supplementary Table S1.
Covariate
In this study, we considered a range of basic sociodemographic factors: age, gender, race/ethnicity, household income, education level, marital status, and insurance status. Smoking and drinking status of the participants was also considered. Smoking status was categorized as never smoked (less than 100 cigarettes in lifetime), former smoker (smoked more than 100 cigarettes and no longer smoked), and current smoker (smoked more than 100 cigarettes and still smoked daily or occasionally). Alcohol consumption was categorized as never drinking (<12 drinks), previous drinking (more than 12 drinks but no more in the last year), and current drinking (more than 12 drinks and still drinking). Daily diet of participants was also considered, including total energy intake, carbohydrate, protein and fat intake. Body mass index (BMI) was included as a covariate in our regression analysis to adjust for the impact of body weight on the relationship between shift work and health outcomes.
Statistical analysis methods
Given the complex multistage sampling design of NHANES, all analyses in this study consider sample weights, strata, and primary sampling units to ensure accurate national representation. Sample weights were constructed so that the sum of the weights matched the survey totals at the midpoint of each survey period, according to the NHANES guidelines for analyzing combined data across cycles. Between-group differences for categorical samples and continuous variables were tested using the chi-squared test and independent samples t test, respectively. Continuous variables are presented as mean ± standard deviation (x ± s) and categorical variables as weighted percentages.
To estimate the association between shift work and both MetS and CircS, we used weighted multivariate logistic regression models. In addition, we assessed the relationship between shift work and the number of MetS and CircS risk factors using univariate and multivariate weighted linear regression models. Furthermore, to examine the impact of various shift work patterns, we analyzed associations between five specific work patterns (regular daytime, evening, night, rotating shifts, and other schedules) and the risks of MetS and CircS. In the above regression analysis, we built four different models to provide statistical inference. In Crude Model, there are no adjustment variables. Adjusted for age and gender in Model 1. In Model 2, adjustments were made from Model 1 for race/ethnicity, educational attainment, PIR, health insurance, marital status, smoking, and alcohol use. In Model 3, dietary factors were additionally adjusted from Model 2 for BMI, calorie intake, fat intake, protein intake, and carbohydrate intake.
In addition, subgroup analyses were conducted to identify sensitive populations. Subgroup analyses were conducted by age (18–60, ≥60), sex (male or female), race/ethnicity (non-Hispanic white, non-Hispanic black, Mexican American, other Hispanic, and other), smoking (never, former, current, unknown), and alcohol use (never, former, current, unknown). Potential interactions were examined by testing the corresponding multiplicative interaction terms.
Sensitivity analyses were conducted to validate the robustness of our findings. This included the application of the inverse probability weighted propensity score matching (PSM) method. In addition, we excluded women aged 45–55 to mitigate the potential confounding effects of menopause.
All analyses were performed using R software (version 4.3.1). A two-tailed P value of less than 0.05 was considered to indicate statistical significance.
Results
Baseline characteristics
Table 1 displays the baseline characteristics of the study participants. This study included a total of 4173 adults, representing 107,077,213 shift workers (74.25%) and 37,125,681 nonshift workers (25.75%) in the United States. The average age of the participants was 41.2 years. Compared with nonshift workers, shift workers were younger, less likely to be non-Hispanic white, and had higher proportions of being impoverished (PIR <1.35), without health insurance, and never married. In addition, the proportion of current smokers was higher among shift workers, but there was no significant difference in alcohol consumption. There were no significant differences between the two groups in terms of diet and energy intake. Notably, compared with nonshift workers, shift workers had lower total cholesterol, low-density lipoprotein cholesterol, and high-density lipoprotein cholesterol, and also lower diastolic blood pressure. The prevalence of hypertension and a decrease in high-density lipoprotein cholesterol was lower among shift workers, but they had higher rates of short sleep duration and depression. Among the participants, 1606 had MetS, representing 37.27%, and 978 had CircS, representing 22.26%. The incidence of MetS did not differ significantly between the two groups, but the proportion of CircS was higher among shift workers.
The Baseline Characteristics of the Study Population Based on Shift Work
Data are presented as mean ± standard error for continuous variables and as number (percentage) for categorical variables. P values were calculated using chi-squared tests for categorical variables, t tests for normally distributed continuous variables, and Mann–Whitney U tests for non-normally distributed continuous variables, comparing the characteristics between shift workers and nonshift workers.
BMI, body mass index; TG, triglyceride; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure; PIR, ratio of family income to poverty; FPL, federal poverty level.
Association between shift work and MetS and CircS
The weighted logistic regression analyses (Table 2) revealed no significant association between shift work and MetS prevalence across all models (odds ratio [OR] for Model 3: 1.04, 95% confidence interval [CI]: 0.78–1.40, P = 0.78). Conversely, shift workers exhibited a significantly higher prevalence of CircS (OR for Model 3: 1.57, 95% CI: 1.23–2.01, P < 0.001).
The Association Between Shift Work and the Risks of Both MetS and CircS
Crude was univariate logistic regression.
Model 1: Adjusted for age (as a continuous variable), gender, race/ethnicity, and education.
Model 2: Adjusted for age (as a continuous variable), gender, race/ethnicity, educational attainment, PIR, health insurance, marital status, smoke status, and alcohol use.
Model 3: Adjusted for age (as a continuous variable), gender, race/ethnicity, BMI, educational attainment, PIR, health insurance, marital status, smoke status, alcohol use, calorie intake, fat intake, protein intake, and carbohydrate intake.
MetS, metabolic syndrome; CircS, circadian syndrome; OR, odds ratio; CI, confidence interval.
Analysis of risk factors and different work patterns
Further analyses, as detailed in Supplementary Table S2, reveal that shift workers are associated with a higher number of risk factors for CircS (regression coefficient in Model 3: 0.13, 95% CI: 0.01–0.25), with no significant change in MetS risk factors (regression coefficient: 0.05, 95% CI: −0.05–0.14).
In addition, different shift work patterns compared with a regular daytime schedule showed no significant increase in MetS risk (Table 3). However, all patterns except for the regular night shift significantly increased the risk of CircS in Model 3.
The Association Between Different Work Patterns and the Risks of Both MetS and CircS
Crude was univariate logistic regression.
Model 1: Adjusted for age (as a continuous variable), gender, race/ethnicity, and education.
Model 2: Adjusted for age (as a continuous variable), gender, race/ethnicity, educational attainment, PIR, health insurance, marital status, smoke status, and alcohol use.
Model 3: Adjusted for age (as a continuous variable), gender, race/ethnicity, BMI, educational attainment, PIR, health insurance, marital status, smoke status, alcohol use, calorie intake, fat intake, protein intake, and carbohydrate intake.
MetS, metabolic syndrome; CircS, circadian syndrome; OR, odds ratio; CI, confidence interval.
Subgroup analysis
Subgroup analyses revealed distinct responses to shift work across demographics. Figure 2 shows a significant correlation between shift work and CircS in individuals under 60, both genders, non-Hispanic whites, and those with a PIR ≥3.5, with no observed interaction effects. Conversely, Supplementary Figure S1 indicates no significant link between shift work and MetS in any population subgroup, consistent across all demographics without interaction effects.
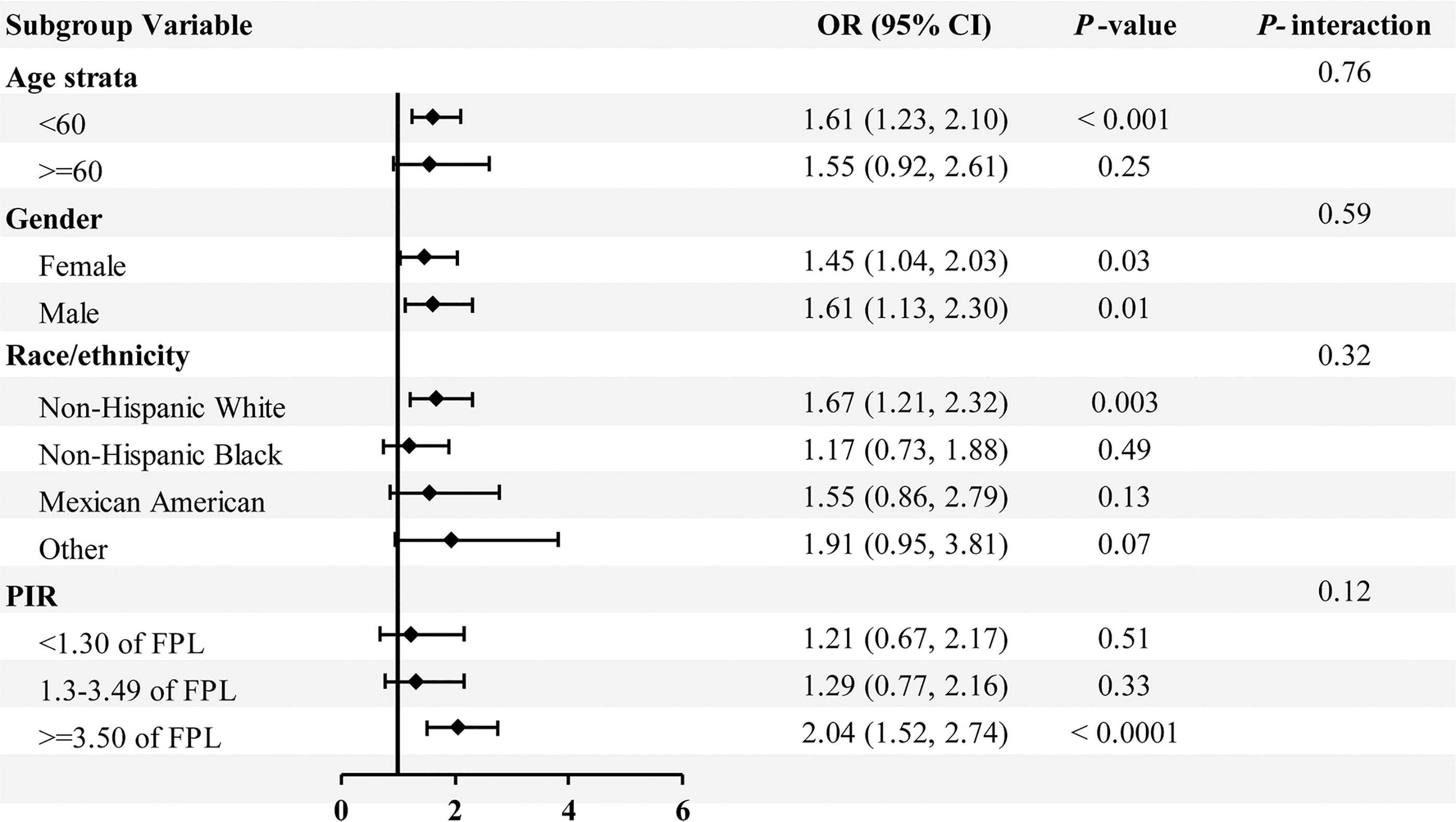
Subgroups analyses for the associations of shift work with the CircS. When not used as stratifying variables, the following covariates were adjusted for in Model 3: age (as a continuous variable), gender, race/ethnicity, BMI, educational attainment, PIR, health insurance, marital status, smoke status, alcohol use, calorie intake, fat intake, protein intake, and carbohydrate intake. OR, odds ratio; CI, confidence interval; PIR, ratio of family income to poverty; BMI, body mass index.
Propensity score matching
To further control for potential confounding factors, we adopted the method of PSM. We selected significant covariates such as age, race/ethnicity, ratio of family income to poverty (PIR), health insurance status, and smoking habits for matching. This was performed using caliper matching with a caliper value set at 0.02 and a matching ratio of 2:1. Supplementary Figures S2 and Figure S3 demonstrate the effectiveness of PSM, showing a significant increase in similarity between the two groups on key variables. The distribution of baseline characteristics in the propensity score-matched population (2186 individuals) is detailed in Supplementary Table S3, indicating that the differences in baseline characteristics between shift workers and nonshift workers have been effectively controlled. After PSM, the results remained consistent with previous findings: there was still no significant relationship between shift work and MetS (Supplementary Table S4). In the fully adjusted model, the risk of CircS in shift workers was higher than in nonshift workers (OR: 1.80, 95% CI: 1.32, 2.45).
After excluding menopausal women, all regression models showed that shift work is linked to a higher risk of CircS with an odds ratio of 1.76 (95% CI: 1.32, 2.36) in Model 3, indicating a significant association (Supplementary Table S5). However, there is no significant correlation with MetS risk.
Discussion
In this nationally representative study, we observed that over 20% of adults are affected by CircS. Unlike CircS, the prevalence of MetS did not differ significantly between shift workers and nonshift workers. Regression analyses yielded consistent results, with shift work being associated with an increased risk of prevalence of circadian rhythm syndrome, but not MetS, in multiple adjusted models. This association was more pronounced among those younger than 60 and non-Hispanic whites. Sensitivity analysis confirmed the robustness of the results.
In the current study, no significant association was found between shift work and MetS, consistent with previous findings from a meta-analysis 16 and other research. 17,18 However, contrasting evidence exists in the literature. 19,20 Recent studies and a new meta-analysis have linked shift work, particularly permanent night shifts, with increased cardiometabolic risks, including dyslipidemia 21 and MetS over a 6-year period. 22,23
The relationship between shift work and other cardiometabolic risks such as overweight, obesity, insulin resistance, and type 2 diabetes has also been well-documented. 24 –27 Shift work, especially long-term night shifts, appears to exacerbate these risks due to increased duration, frequency, and intensity of exposure. Overall, despite some variation and uncertainty, there is growing evidence that shift work may increase cardiometabolic risk.
The circadian rhythm syndrome expands on the traditional cardiovascular risk factors by expanding the definition based on the pathological mechanisms of circadian rhythm disruption. Shift work is associated with sleep disorders, dietary imbalances, and unhealthy lifestyles, all of which disrupt the body’s internal 24-hr biological clock, affecting nearly all physiological cycles. 28,29 A large proportion of genes and proteins in the human body are regulated by circadian genes, 30 –32 and the circadian system can directly or indirectly regulate almost every endocrine factor or its downstream effects. 33 Shift work increases hormone disruption in midwives, a multicenter study suggests. 34 Current breakthroughs in basic research on the circadian system are helping us to understand physiology and disease at the molecular level. However, diagnosis of circadian rhythm disorders may often involve multiple samples throughout the day, and the difficulty of detecting and diagnosing circadian rhythm disorders-related disorders is a major obstacle to applying this knowledge in the clinic. 29 This study found that shift work was associated with an increased risk of CircS and was not significantly associated with MetS. This may add to the diagnosis of metabolic dysfunction in shift workers, whereas circadian rhythm disruption syndrome provides evidence as a clinical test for circadian rhythm disruption.
There are some limitations to this study. First, the transect design limits the ability to assign causality. In addition, there is no standardized definition of shift work, which varies from country to country and from survey to survey, as shift work is based more on legal definitions than on scientific backgrounds. 35 Owing to limitations in the survey design, there was no consideration of shift work hours in the study, and it is clear that there are differences in the health effects of short- and long-term shift exposures. The effects of shift work are multifaceted, and other factors may also affect health, such as the intensity of physical activity at work, occupational stress, and the work environment; how to identify confounding factors has been an ongoing issue in the study of shift work. Although we consider a variety of statistical models to control confounding factors, residual confounding factors may still exist. The strengths of this study are the use of a nationally representative sample and the enhanced ability to generalize the entire U.S. population with full consideration of the weighting of each participant. In addition, this is the first program to study shift work and circadian rhythm syndrome. Comparisons were made with the traditional MetS, and the results suggest that circadian rhythm syndrome may be a better response to metabolic disturbances in shift workers than the MetS. Another significant limitation is that CircS is a newly proposed concept, and there has yet to be comprehensive research into its sensitivity and accuracy as a diagnostic tool. This lack of empirical grounding could affect the reliability of CircS as an indicator of health outcomes in shift workers.
Conclusion
In summary, shift work is associated with an increased risk of circadian rhythm syndrome, not MetS, according to NHANES 2005–2010 data. This may add to the rationale for clinical recognition of circadian rhythm disorders. However, to enhance the quality of evidence and establish more definitive conclusions, further research is essential. Specifically, longitudinal studies are required to explore the causality and long-term effects of shift work on circadian health.
Footnotes
Acknowledgments
The author extends sincere gratitude to all individuals who made invaluable contributions to this research.
Authors’ Contributions
X.L. conceived and designed the study. L.W. extracted and analyzed data. L.W., S.W., and Y.W. wrote the article., S.W. conducted data visualization analysis, Y.J., J.H., and X.L. reviewed and revised the article, and X.L. supervised this project. All authors have read and agreed to the published version of the article.
Institutional Review Board Statement
The National Center for Health Statistics and Research’s Ethics Review Committee has approved the NHANES studies. The consent form was signed by every participant in the survey. The NHANES database is accessible without ethical or administrative approval.
Data Availability Statement
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
Grants supported this study from the
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.