
Abstract
Background and Aims:
Menopause is a complex period in women’s life, when weight gain and predisposition to obesity are frequent. Moreover, even during menopause transition, women begin to lose lean mass up to 0.5% and, therefore, an increase in the percentage of fat mass with central distribution and an increased risk of metabolic syndrome. Despite lifestyle habits remain the cornerstone in this period, their long-term effectiveness is a challenge. In this sense, GLP-1 analogs have shown their efficacy in improving weight loss and other cardiovascular risk factors.
Methods:
To assess the effectiveness of low doses of semaglutide on body weight and composition for 4 months during menopause compared with premenopausal women.
Results:
Baseline weight and body mass index were significantly greater among postmenopausal women (95 ± 23.4 vs. 86.4 ± 12.8 kg and 35.9 ± 7.3 vs. 32.9 ± 4.7 kg/m2; P = 0.02 and P = 0.03, respectively). Fat mass was higher among postmenopausal women (45.2 ± 17.1 vs. 38.2 ± 9.8 kg; P = 0.03). The percentage of fat mass and lean mass were comparable between the two groups (43.2 ± 8.1% vs. 40.9 ± 7.1% and 29.6 ± 5.5 vs. 32.4 ± 8.4 kg; P = 0.2 and P = 0.08, respectively). After 4 months of semaglutide 1 mg, either weight loss (5.9 ± 5.2 vs. 4.5 ± 3.5 kg; P = 0.1) or percentage of weight loss (5.8 ± 4.7% vs. 5.1 ± 3.2%; P = 0.4) were comparable. Furthermore, both fat mass loss in kilos (4.1 ± 4.5 vs. 3.1 ± 3.7 kg; P = 0.3) and lean mass loss (−0.4 ± 1.7 vs. −1.1 ± 3.7 kg; P = 0.1) were similar between the two groups.
Conclusions:
Despite a greater initial weight and fat mass among postmenopausal women, after 4 months of treatment with semaglutide 1 mg, either fat mass loss or weight loss were similar to premenopausal women.
Introduction
The aging of the world population is about to become one of the most significant social transformations of the 21st century, with a significant impact on almost every aspect of the society, such as occupational, familial, cultural, and health. According to the World Health Organization in 2050, one in six people worldwide will be over 65 years old (16%), even more than the current proportion of 1 in 11 in 2019 (9%). 1 In Spain, as in most Western countries, life expectancy is greater for women. In 2021, life expectancy at birth was 85.8 years for women and 80.2 years for men. 2
On the contrary, overweight and obesity are defined as abnormal or excessive fat accumulation that presents a risk to health. Obesity is a complex, multifactorial, and relapsing disease that is associated with multiple co-morbidities, not only metabolic but also mechanical and psychological. In fact, more than 650 million people worldwide live with obesity. 3 In Spain, more than 20% of adult women live with obesity. 4
In this sense, menopause is a complex period in women’s life, when weight gain and predisposition to obesity are frequent. An average weight gain of 0.5–0.7 kg/year might occur, independent of their initial body weight or ethnicity. Besides this weight gain, postmenopausal women also experience changes in body fat distribution, mainly a greater tendency of central accumulation, with an increased risk of metabolic syndrome and cardiovascular disease. Moreover, even during menopause transition, women begin to lose lean mass up to 0.5% and, therefore, an increase in the percentage of fat mass. Several factors are associated with this tendency to fat accumulation, some of them are nonmodifiable, such aging and hormonal changes. However, efforts to prevent both fat accumulation and maintain lean mass should be focused on changing modifiable factors. In this sense, sleep disturbances, a decrease in physical activity, a predisposition to mood disorders and emotional eating, and preference for consuming high calorie and processed foods should be identified and treated. 5 –8
Therefore, physicians caring for women in their menopause should routinely screen for metabolic syndrome and, particularly, obesity and offer an individualized weight management program. The cornerstone should be lifestyle modifications, promoting regular physical activity, predominantly resistance exercise to preserve lean mass, as well as a caloric restriction. 6,9 Also, individualized nutritional education by a specialist should be encouraged as long as there is no “one-size-fits-all diet.” 10 However, the long-term effectiveness of lifestyle habits alone is a challenge. Besides, weight loss and maintenance are frequently slower and harder and require an additional effort among postmenopausal women related to physiological changes, such as estrogen deficiency and loss of lean mass. This is the reason why a pharmacological approach is on the rise. 7
In this sense, GLP-1 analogs, such as liraglutide and semaglutide have been shown to act, not only on homeostatic hunger-satiety brain areas but also on the mesolimbic system, which is related to hedonic overeating. 11 FDA approved weekly semaglutide 2.4 mg for the treatment of patients with obesity as an adjunctive therapy to lifestyle intervention. The Semaglutide Treatment Effect in People with obesity (STEP) trials have shown the efficacy on weight loss and safety of semaglutide among people with obesity, even greater than with the treatment with liraglutide 3 mg. 12,13 STEP 4 showed that weight loss achieved during the run-in period with semaglutide 2.4 weekly, not only was sustained but continued, reaching a plateau approximately at week 68 and resulting in a reduction of 17.4%. 14 Besides, semaglutide could also improve emotional eating, diminish ad libitum energy intake, and reduce food cravings, very frequent among postmenopausal women. 15 However, until May 2024, it has been approved in Spain only when type 2 diabetes is associated with obesity, being the usual dose 1 mg per week. Moreover, it is not well studied whether semaglutide in postmenopausal women is as effective in losing weight as in general population.
Therefore, we aimed to study the efficacy on weight loss and changes in body composition as well as gastrointestinal tolerance of semaglutide 1 mg among women in their postmenopausal period compared with premenopausal women.
Material and Methods
Subjects
This observational prospective study included 100 women attending an obesity clinic. These patients failed to achieve or maintain a significant weight loss despite lifestyle interventions, such as a tailored and hypocaloric diet and a minimum of 150 min of exercise per week. Also, most of these patients were prescribed liraglutide 3 mg previously but it was stopped for different reasons, with the main ones being lack of efficacy, its cost, and its lack of supply. After starting semaglutide, there was a throughout shared decision process involving the patient, in which understandable information regarding potential benefits and harms of subcutaneous semaglutide use were reviewed. All patients were prescribed weekly sc semaglutide with an out-of-label indication for weight reduction in Spain. This treatment was an adjunctive therapy of a lifestyle intervention program and regular follow-up office visits. Eligibility criteria were as follows: (1) Women older than 18 years with a body mass index (BMI) equal or greater than 27 kg/m2 with co-morbidities related to obesity other tan type 2 diabetes or a BMI equal or greater than 30 kg/m2. (2) Patients without a personal history of medullary thyroid carcinoma and acute or chronic pancreatitis. (3) Patients who were able to understand the given information and capable to maintain a regular follow-up. (4) Patients who did consent to participate in the study. This study was conducted according to the World Medical Association Declaration of Helsinki. The study was approved by the Ethics Committee of the hospital. Informed consent was obtained from all subjects prior to study participation.
Interventions
Diet counseling included a tailored and structured quantitative diet with an average of 500 kcal/day reduction from calculated baseline metabolic rate adjusted by physical activity. Besides, a minimum of 150 min of exercise per week, encouraging resistance training, was also prescribed. To measure the exercise per week performed by the subjects included in the study, the step counters of the smartphones were used. About 10,000 steps usually correspond to 5 km and, in general conditions, such distance is completed in 1 hr. In this way, we calculate the minutes of aerobic exercise per week. We also used self-reported agendas to determine training indoor sessions.
Regarding semaglutide titration, patients started with a dose of 0.25 mg per week for the first 2 weeks and, depending on the tolerance and side effects, mostly gastrointestinal, this dose was titrated up to 0.5 mg after 2 weeks of treatment. This dose was increased to 1 mg once weekly after a minimum of 4 weeks of treatment when there was no significant improvement in abnormal eating patterns.
Patients were evaluated baseline, and after 4 months since the beginning with semaglutide.
Body weight and composition
Height and weight were measured while each participant was wearing indoor clothing without shoes. BMI was calculated as weight divided by height squared. Waist circumference was measured at the midpoint between the lowest rib and the iliac crest. Body composition was assessed with a bioimpedance device (InBody 270). Patients were advised not to eat, drink, or exercise within 4 hr prior to taking the bioimpedance test.
Assessment of abnormal eating patterns and psychological well-being
To rule out binge episodes, emotional eating, food cravings (sweet and salty), as well as the psychological interference of obesity on daily activities, a structured interview was performed baseline and after 4 months of treatment with semaglutide.
Statistical analysis
Main outcomes in this study were body weight loss as well as the effect on other anthropometric measures and body composition parameters after 4 months of treatment with semaglutide 1 mg among women in their postmenopausal period and whether these changes differed from the ones observed from premenopausal females. Menopause was defined as the absence of menstruations for 12 consecutively months or FSH levels greater than 25 UI/L or whether a hysterectomy had been previously performed.
Statistical analyses were performed using the IBM® SPSS® Statistics Version 23.0. Initial analyses were descriptive and included calculation of mean, median, and standard deviation for continuous variables and frequencies for categorical variables. The distribution of the sample was analyzed by the Kolmogorov–Smirnoff test. Comparison between the two groups was analyzed by an unpaired Student’s test. Wilcoxon test was used to compare changes after treatment with semaglutide in pre- and postmenopausal women. A P value of <0.05 on the two-tailed test was considered to indicate statistical significance.
Results
Of the 100 women included, 45% were in their postmenopausal period. As expected, postmenopausal women were older than premenopausal females (53.6 ± 5.9 vs. 38.4 ± 7.9 years; P < 0.0001). Importantly, only 2 out of 45 postmenopausal women were on hormone replacement therapy, whereas 16% of premenopausal women were using hormonal contraceptives. No differences were seen in terms of the prevalence of family history of obesity among postmenopausal and premenopausal women (37.7% vs. 54.5%; P = 0.4).
Baseline weight and BMI were significantly greater among postmenopausal women (95 ± 23.4 vs. 86.4 ± 12.8 kg and 35.9 ± 7.3 vs. 32.9 ± 4.7 kg/m2; P = 0.02 and P = 0.03, respectively). When taking into account body composition parameters at baseline, fat mass was significantly higher among postmenopausal women compared with the premenopausal ones (45.2 ± 17.1 vs. 38.2 ± 9.8 kg; P = 0.03). However, the percentage of fat mass and lean mass were comparable between the two groups (43.2 ± 8.1% vs. 40.9 ± 7.1% and 29.6 ± 5.5 vs. 32.4 ± 8.4 kg; P = 0.2 and P = 0.08, respectively). These data are shown in Table 1.
Baseline Anthropometric Parameters in Premenopausal and Women in Their Postmenopausal Period
Data are expressed in mean ± SD or absolute numbers and %. Student’s t-test (unpaired) was used to compare the differences.
BMI, body mass index.
Regarding co-morbidities related to obesity, postmenopausal women had more hypertension (31.1% vs. 5.5%; P = 0.001). Both groups were comparable in terms of the frequency of dyslipidemia (8.9% vs. 1.8%; P = 0.06), depression (18.9% vs. 5.5%; P = 0.08), or binge eating disorder (2.2% vs. 3.6%; P = 0.8). Also, sweet (68.9% vs. 36.4%; P = 0.8) and salty cravings (31.1% vs. 65.4%; P = 0.7) as well as the prevalence of emotional eating (84.4% vs. 83.6%; P = 0.2) were similar between the two groups. However, the frequency of patients who referred worries about their problem with obesity was significantly greater among premenopausal women (80% vs. 23.6%; P = 0.001).
As shown in Tables 2 and 3, after 4 months of treatment with low doses of semaglutide both groups experienced significant reductions in weight and improvements in body composition parameters as well as in abnormal eating patterns.
Changes in Anthropometric Parameters in Premenopausal after 4 Months of Treatment with Semaglutide 1 mg
Data are expressed in mean ± SD or absolute numbers and %. Student’s t-test (paired) was used to compare the differences.
BMI, body mass index.
Changes in Anthropometric Parameters in Postmenopausal After 4 Months of Treatment with Semaglutide 1 mg
Data are expressed in mean ± SD or absolute numbers and %. Student’s t-test (paired) was used to compare the differences.
BMI, body mass index.
When we compared the evolution of anthropometric parameters between the two groups after 4 months of treatment with semaglutide 1 mg, either weight loss (5.9 ± 5.2 vs. 4.5 ± 3.5 kg; P = 0.1) or percentage of weight loss (5.8 ± 4.7% vs. 5.1 ± 3.2%; P = 0.4) were comparable. Furthermore, both fat mass loss in kilos (4.1 ± 4.5 vs. 3.1 ± 3.7 kg; P = 0.3) and lean mass loss (−0.4 ± 1.7 vs. −1.1 ± 3.7 kg; P = 0.1) were similar between the two groups.
These data are represented in Fig. 1.
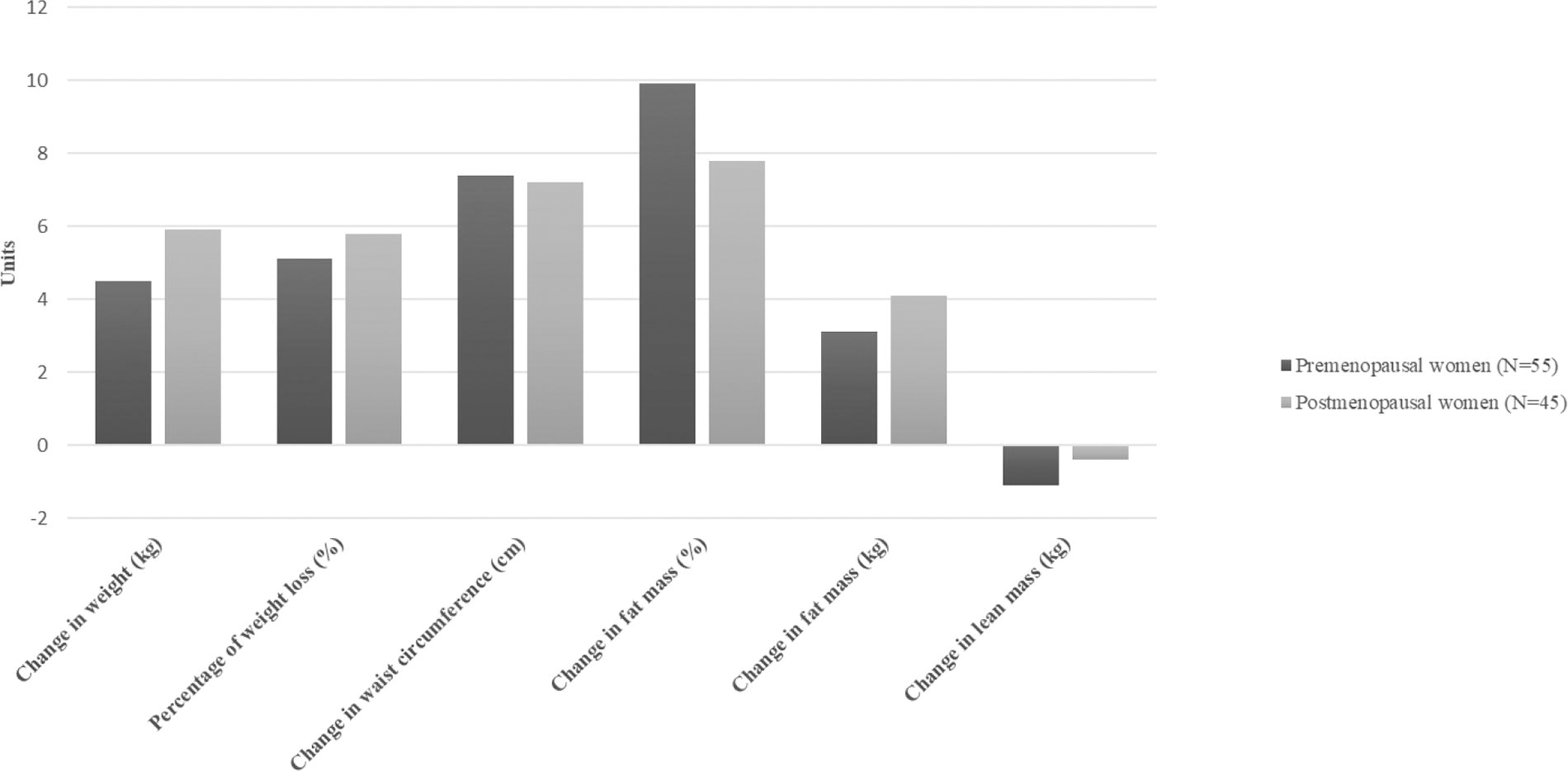
Changes in anthropometric parameters between pre- and postmenopausal women after 4 months of treatment with semaglutide 1 mg: *No significant differences were seen between pre- and postmenopausal women.
No differences regarding gastrointestinal side effects and treatment discontinuations were seen between the two groups. No discontinuations were seen during the follow-up period.
Discussion
We found that, despite a greater initial weight and fat mass among women in their menopause, after 4 months of treatment with weekly semaglutide, either fat mass loss or weight loss were similar to premenopausal women. Moreover, lean mass loss was also comparable between the two groups.
Once weekly semaglutide has shown positive effects on weight among people with obesity. Across all SUSTAIN trials (Semaglutide Unabated Sustainability in Treatment of Type 2 Diabetes), semaglutide consistently demonstrated significantly greater weight reductions versus all comparators. Mean weight loss was 4.5–6.5 kg with semaglutide 1 mg for 30 weeks. 16 Furthermore, the Semaglutide Treatment Effect in People with obesity (STEP) clinical trials evaluated the effect, safety, and tolerability profile of semaglutide 2.4 mg once-weekly to obtain regulatory approval of this long-acting GLP-1 analog for weight management regardless of type 2 diabetes. 12 Mean weight loss across STEP trials was 17% for 68 weeks of treatment. 12 These data were also confirmed in two meta-analyses published so far. 17,18 To date, no specific data on women in their menopause have been published. We found that mean weight loss was around 5% either with menopausal or premenopausal women, a percentage similar to the one achieved among patients included in the STEP program when they were at week 16 when mean dose was 1 mg, and despite the fact that the dose was lower in our study. 19 In a subpopulation from STEP trials, a DEXA was performed baseline and at the end of treatment with semaglutide. Total fat mass was significantly reduced and the proportion of lean body mass relative to total body mass increased in the semaglutide group. Besides, weight loss with semaglutide was accompanied by greater improvements in other cardiovascular risk factors as well as in quality of life. 19
At least a third of a woman’s life is spent after menopause. Not only estrogen deprivation but also age are responsible for anthropometric changes, particularly lean mass loss and increased abdominal fat deposition, which predispose to the onset of cardiovascular risk factors, such as obesity and insulin resistance. 8 These changes usually negatively affect mood and quality of life, increasing sedentary behaviors, predisposing to emotional eating and other abnormal eating patterns, and impairing mood. In this sense, and despite the neurobiological basis of depression is not completely understood, fluctuation levels of estrogens during premenopause and menopause could play a role by impairing neurotransmitters. In fact, estrogen is involved in the modulation of serotoninergic, noradrenergic, and dopaminergic systems, which control mood. 20,21 The combination of all these factors predisposes atherogenic mechanisms to emerge and, therefore, cardiovascular risk increases significantly. For this reason, menopause is an important period in a woman’s life for screening all these negative physical and emotional changes and interventions when necessary. Some studies have shown the positive effect of lifestyle factors on weight gain and other cardiovascular risk factors. In fact, metabolic syndrome could be reversed by 16% only with diet and regular exercise. 22,23 However, there is still a significant risk left to solve. Despite lifestyle changes remain the cornerstone of obesity treatment, it should be considered that weight loss is frequently less rapid and effective and requires an extra and sustained effort among menopausal women. 5,8 Moreover, weight loss maintenance can be a real challenge due to the physiological responses to weight loss at any age. 24 For this reason, it should be considered pharmacological treatment as an adjuvant therapy to lifestyle modifications.
However, it is known that during the transition to menopause there is a loss of lean mass, with a potential risk of decreased basal energy expenditure that makes weight loss and weight maintenance difficult. 5,6 Furthermore, preservation of muscle mass should encompass an adequate protein intake and resistance exercise, especially when there is rapid weight loss, 7 such as when antiobesity drugs such as semaglutide are prescribed. In this sense, we tailored an individualized nutritional plan with an adequate protein intake and resistance exercise was prescribed. However, we could not accurately quantify daily physical activity or protein intake, but it seems that they were sufficient to prevent significant lean mass loss. It has been shown that persons with obesity have more total fat-free and muscle mass than those with normal weight. Weight loss decreases both fat and lean body mass. However, in people with obesity, fat-free mass contributes only to 20–30% to total weight loss. 25 It has been shown that females experience lean mass reductions with voluntary calorie reduction of about 1–1.5 kg per 10-kg weight loss, as in our study. 26 Furthermore, prolonged moderate caloric restriction and 5–10% weight loss increase the rate of muscle protein synthesis. Therefore, the loss of muscle mass during calorie restriction is mediated by increased muscle proteolysis rather than suppressed protein synthesis. 25
Besides, it is well known that a 5–10% reduction in weight results in significant amelioration of metabolic, mechanical, and psychological co-morbidities of obesity. 27 However, during menopause, as there is a significant increase in cardiovascular events, treatment should be addressed not only for weight loss purposes, but also for the reduction of cardiovascular risk. In this sense, with the recent preliminary results from SELECT, where treatment with semaglutide 2.4 mg among subjects with obesity reduced cardiovascular events by 20%, could be a promising treatment among women in their menopausal period. 28,29
Previously, daily liraglutide, the first-line antiobesity treatment in Spain, 27 has shown positive results among women in their menopause. Vazquez et al. studied the effect of liraglutide for 12 months among 123 postmenopausal women with obesity. They found that more than 70% of these women lost more than 5% of their initial weight as well as a significant amelioration of other cardiovascular risk factors. 30 However, it should be noted that once-weekly regimen may improve treatment adherence.
Besides, psychological well-being and abnormal eating patterns are frequent among women in their menopause. It is known that liraglutide exerts positive effects not only on hypothalamic centers of satiety but also on mesolimbic systems, related to cravings and emotional eating. 31 We found that both groups were comparable in ameliorating these abnormal eating patterns irrespective of menopause.
We acknowledge that our study has several limitations. Baseline weight and BMI were not comparable between the two groups. As it was performed in a single institution, results may not be generalizable to other populations and settings. In Spain, antiobesity treatments are not reimbursed by the national health system and, therefore, people who attend a weight loss clinic may have a higher sociocultural status and result in a selection bias. Furthermore, in Spain, until May 2024, semaglutide was used as off-label indication, but since it has already been approved by the FDA and many European countries, and results from the clinical trials have already been published, it is important to collect real-world data. However, both the sample size and the follow-up of the study, despite relatively short, was long enough to achieve significant results. We also added body composition parameters to the traditional BMI, which is unable to show fat distribution and lean mass, important in this setting. However, in our analysis, we did not register resistance exercise, which could have biased our results. We acknowledge, and in order to confirm our results, that further studies should also collect the effects of semaglutide on metabolic parameters or inflammatory markers among menopausal women compared with premenopausal. Also, whether these changes would be similar with higher doses of semaglutide deserve further research.
Menopause is a complex period in a woman, not only related to metabolic changes but also psychological. Aging of the population and the increase in life expectancy in developed countries increase the number of women in their menopause. In fact, there are approximately 1 billion women worldwide past the age of menopause. 8 A multidisciplinary approach is mandatory to reduce metabolic complications and, thus, diminish cardiovascular risk, but also to preserve self-esteem, mood, and quality of life.
In conclusion, 1 mg weekly semaglutide as adjunctive therapy to lifestyle interventions among women in their menopause period is as effective as in premenopausal women in reducing body weight and fat mass, without losing significant lean mass.
Authors’ Contributions
J.N. wrote the article, researched data, and gave final approval of the version. J.N. and J.J.F.-J. made the statistics and reviewed the article. A.B. performed a psychological structured interview. A.G.-P. contributed to the discussion, reviewed the article, and gave final approval of the version.
Compliance with Ethical Standards
All studies performed involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. All participants included in the study understood the information related to the study, understood, and signed a written informed consent. All authors signed that there is no current or potential conflict of interest in relation to this article.
Footnotes
Acknowledgements
Data Availability Statement
Data analyzed during the current study are available from the corresponding author on reasonable request.
Author Disclosure Statement
The authors report there are no competing interests to declare.
Funding Information
No funding was received for conducting this study.