
Abstract
Introduction:
Hashimoto’s thyroiditis is a common endocrinological disorder that often coexists with obesity. Thyroid hormones interact with the regulation of sex steroids, and thyroid autoimmunity has a negative impact on female fertility. There are studies showing when euthyroid state is achieved with hormone replacement therapy (HRT), the reproductive hormone profile is improved but they usually compare the reproductive hormones before and after HRT in the same individuals. Studies comparing patients with Hashimoto’s thyroiditis in an euthyroid state receiving HRT with individuals having normal thyroid function are limited. Here, it was aimed to search the impact of euthyroid Hashimoto’s thyroiditis on reproductive hormone profile in women living with obesity.
Materials and Methods:
Sixty-one randomly selected female patients with Hashimoto’s thyroiditis were included as the case group and 60 patients without Hashimoto’s thyroiditis were included as the control group, from our obesity center. The case group included patients who had menstrual cycles and were euthyroid under
Results:
A total of 121 patients were included in the study. Mean age was 41.8 ± 8.5 years in case and 38.6 ± 8.9 years in control group. There was no significant difference in weight, height, BMI, WC, or accompanying diseases between Hashimoto’s thyroiditis and control group. fT4, anti-TPO, cortisol levels were higher in Hashimoto’s thyroiditis group when compared with control group, but there was no significant difference for TSH, insulin, FSH, LH, E2, prog, T, DHEAS, or PRL.
Conclusion:
In women living with obesity, it is important to screen for Hashimoto’s thyroiditis and achieve euthyroidism through effective LT4 treatment to promote a healthy reproductive system and improve fertility rates.
Introduction
Obesity is a globally growing public health problem burdened with several complications and accompanying diseases. 1 Thyroid dysfunction; especially Hashimoto’s thyroiditis is a common endocrinological disorder that often coexists with obesity. Also, thyroid peroxidase antibody (anti-TPO) positivity is found associated with obesity. 2,3
Thyroid hormones affect uterine and ovarian tissues, modulating their development and metabolism. Thus, they are vital for the normal functioning of the female reproductive system. The relationship of hypothroidism with altered ovarian functions, menstrual irregularity, increased abortion, and subfertility supports the idea of the involvement of thyroid dysfuntion in abnormalities in the female reproductive system. 4,5
Thyroid autoimmunity is the most common thyroid dysfunction among women at reproductive age. TPOAb or TPOAb/TgAb positivity has a negative impact on female fertility even in the absence of thyroid dysfunction. 6
Thyroid hormones [TRH, thyroid stimulating hormone (TSH), T3, and T4] play facilitative roles at each level of the hypothalamic-pituitary-gonadal (HPG) axis. TSH appears to influence the HPG axis both directly with involvement in the HPG axis and indirectly through its relationship with leptin hormone. The effect of T3 and T4 on HPG axis is not completely clear but the indirect effects of gonadotropin-inhibiting hormone, insulin, or glucocorticoids offer possible pathways through which T3 and T4 may be regulating these neurons. Thyroid hormones interact with the regulation of upstream metabolic signals and the secretion and transport of downstream sex steroids indirectly. Hypothyroidism causes an increase in TRH levels and this in TSH and prolactin (PRL). And PRL inhibits the production and secretion of gonadotropins. 5
There are studies showing when euthyroid state is achieved with hormone replacement therapy (HRT), the reproductive hormone profile is improved but those studies usually compare the reproductive hormones before and after the thyroid hormone therapy in the same individuals. Studies comparing patients with Hashimoto’s thyroiditis in an euthyroid state receiving HRT with individuals having normal thyroid function are limited. 7,8 Here, it was aimed to search the impact of euthyroid Hashimoto’s thyroiditis on the reproductive hormone profile in women living with obesity.
Material and Methods
The study was conducted at the obesity center, which is part of the internal medicine clinic in a training and research hospital. With a 5% margin of error and 80% power, the standard effect size was measured as 0.52, and each group required 58 subjects. Sixty-one patients with Hashimoto’s thyroiditis, randomly selected by record numbers, served as the case group, while 60 patients without Hashimoto’s thyroiditis served as the control group in the study. Participants were chosen based on inclusion and exclusion criteria from our hospital’s obesity center. Data on weight, height, body mass index (BMI), waist circumference (WC), free thyroxine (fT4), TSH, anti-TPO, cortisol, insulin, PRL, follicular stimulating hormone (FSH), luteinizing hormone (LH), estradiol (E2), progesterone (prog), testosterone (T), dehydroepiandrosterone sulfate (DHEAS) levels,
Inclusion criteria
BMI ≥30 kg/m2
Being female
Having menstrual cycles
Having Hashimoto’s thyroiditis diagnosis
Being euthyroid under
Having a file with full results of research parameters in obesity center
Exclusion criteria
Not having Hashimoto’s thyroiditis diagnosis
Having Hashimoto’s thyroiditis but not being euthyroid
Having any other diagnosed thyroid disease
Being menopausal
Having polycystic ovary syndrome (PCOS) or other gynecological disorder affecting hormone profile
Having malignancy
Having severe organ failure (e.g., end-stage of renal, hepatic, and cardiac disease)
Ethical approval
Ethics committee approval was received for this study from the Ethics Committee of Istanbul Training and Research Hospital (06/14.06.2024). All participants provided written informed consent. All procedures performed in the study were in accordance with the 1964 Helsinki Declaration.
Statistical analysis
Mean, standard deviation, median, minimum, maximum value frequency, and percentage were used for descriptive statistics of the data. The distribution of variables was evaluated with the Kolmogorov-Simirnov, Shapiro-Wilk test. Independent samples t-test and Mann–Whitney U test were used for the comparison of quantitative data. The chi-square test was used for the comparison of qualitative data. SPSS 28.0 was used for statistical analysis.
Results
From our hospital’s obesity center, 61 female patients with Hashimoto’s thyroiditis who have been euthyroid at least for 6 months on
General Characteristics of the Entire Study Group
1: diabetes mellitus; 2: hypertension; 3: hyperlipidemia; 4: chronic renal failure; 5: coronary artery disease/heart failure.
Anti-TPO, thyroid peroxidase antibody; BMI, body mass index; DHEAS, dehydroepiandrosterone sulfate; FSH, follicular stimulating hormone; fT4, free thyroxine; LH, luteinizing hormone; PRL, prolactin; SD, standard deviation; TSH, thyroid stimulating hormone; WC, waist circumference.
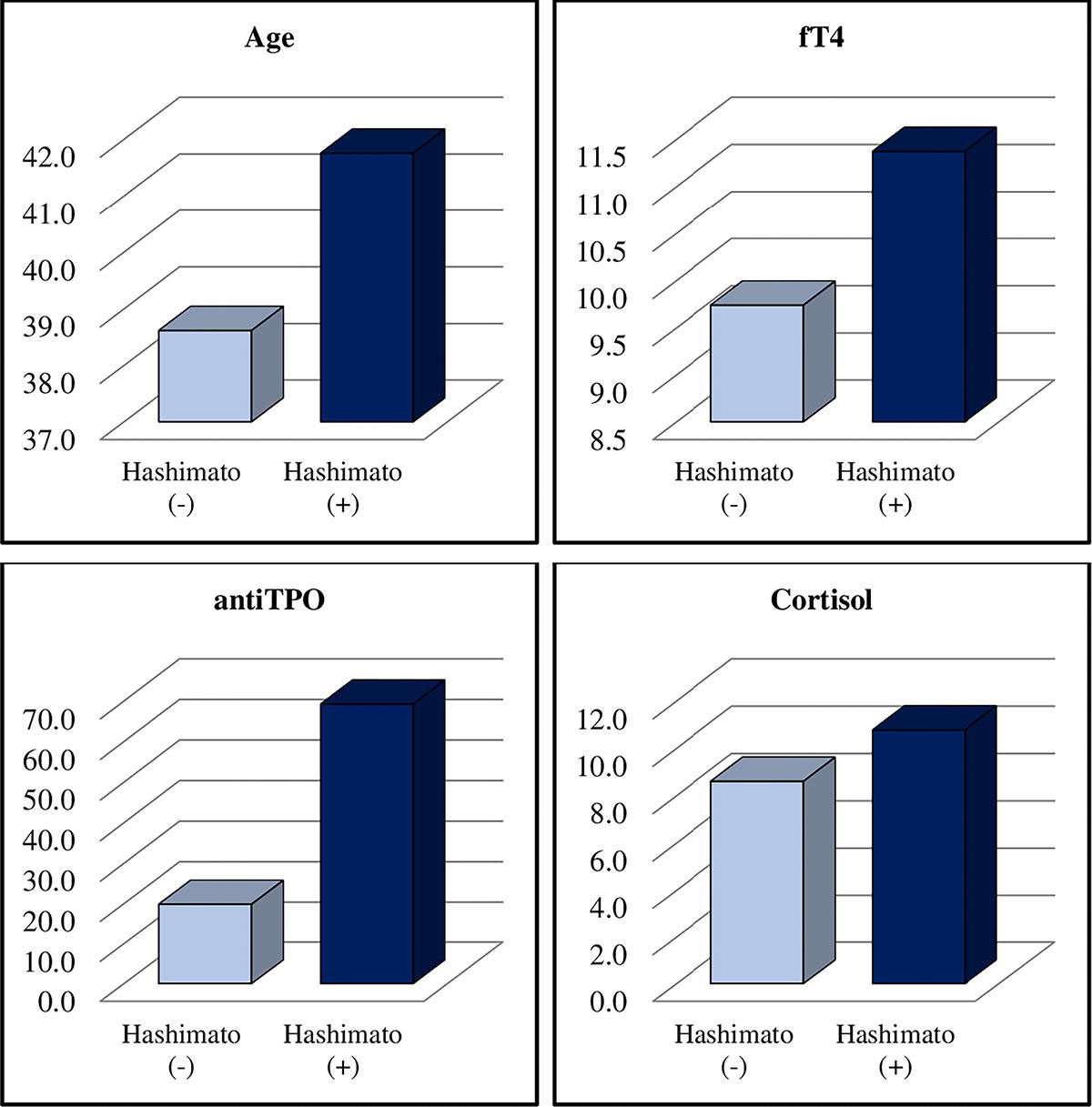
Mean age of Hashimoto’s thyroiditis group was 41.8 ± 8.5 years and control group was 38.6 ± 8.9 years. Mean age of Hashimoto’s thyroiditis group was higher than control group (P < 0.05).
Mean weight was 99.6 ± 17.3 kg in Hashimoto’s thyroiditis group and 103.2 ± 16.8 kg in control group. Mean height was 158.7 ± 6.1 cm in Hashimoto’s thyroiditis group and 159.0 ± 6.2 cm in control group. Mean BMI was 39.6 ± 7.0 kg/m2 in Hashimoto’s thyroiditis group and 40.8 ± 6.0 kg/m2 in control group. Mean WC was 111.4 ± 14.2 cm in Hashimoto’s thyroiditis group and 113.8 ± 13.1 cm in control group. A total of 47.5% (n = 29) of patients with Hashimoto’s thyroiditis and 40% (n = 24) of control patients had one or more accompanying diseases. There was no significant difference for weight, height, BMI, WC, or accompanying diseases between Hashimoto’s thyroiditis and control group (P > 0.05) (Table 2).
Comparison of Research Parameters Between Study Groups
The statistical significance level was regarded as P < 0.05.
Mann–Whitney U test.
Independent sample test.
Chi-square test.
Mean fT4 was 11.4 ± 3.4 mg/dL in Hashimoto’s thyroiditis group and 9.7 ± 4.1 mg/dL in control group. Mean TSH was 3.1 ± 2.4 mg/dL in Hashimoto’s thyroiditis group and 2.4 ± 1.0 mg/dL in control group. Mean anti-TPO was 69.2 ± 102.2 mg/dL in Hashimoto’s thyroiditis group and 19.8 ± 39.1 mg/dL in control group. Mean cortisol was 10.8 ± 7.4 µg/dL in Hashimoto’s thyroiditis group and 8.6 ± 3.5 µg/dL in control group. fT4, anti-TPO, cortisol levels were higher in Hashimoto’s thyroiditis group when compared with control group (P < 0.05) (Table 2, Fig. 1). There was no significant difference for TSH, insulin, FSH, LH, E2, prog, T, DHEAS, or PRL between Hashimoto’s thyroiditis and control group (P > 0.05) (Table 2).
Parameters with statistically significant difference between Hashimoto’s thyroiditis and control group.
Discussion
Obesity is a chronic inflammatory process, and its presence is associated with the exacerbation of various autoimmune diseases, as well as the progression of these conditions and impaired treatment response. 9 Therefore, the coexistence of autoimmune diseases such as Hashimoto’s thyroiditis warrants extra attention during obesity follow-up and treatment.
Autoimmunity has been identified as a component of polycystic ovarian syndrome. A strong association of anti-TPO antibodies with PCOS was found. Hashimoto’s thyroiditis is three times more common in women with PCOS when compared with non-PCOS women of reproductive age. 10
In a study conducted by Ott et al. among women diagnosed with premature ovarian failure, those testing positive for thyroid autoantibodies exhibited lower levels of DHEAS and DHEAS levels showed an inverse correlation with anti-TPO antibodies. 11 A strong association between infertility, miscarriages, and disturbed thyroid profile was found in pregnant women. 10
Anti-TPO positivity may influence fertility outcomes in both natural and assisted conception. In women with infertility, the presence of positive antithyroid autoantibodies can indicate a generalized immune response. 12 This concept is supported by the POSTAL 13 and TABLET 14 studies. Even in a euthyroid state, women experiencing infertility and testing positive for anti-TPO antibodies are typically offered LT4 treatment. 15
In our study, anti-TPO levels were higher in Hashimoto’s thyroiditis group, as expected, compared with the control group. Despite all patients with Hashimoto’s thyroiditis being euthyroid at the time of the study, the mean fT4 levels were higher in the Hashimoto’s thyroiditis group, likely due to replacement therapy. Similarly, a study by Studen et al. found higher thyroid hormone levels in women with Hashimoto’s thyroiditis compared with a healthy control group. 16
Glucocorticoids serve as major suppressors of the immune system and may play a protective role in certain types of autoimmunity. In our study, cortisol levels were found to be higher in Hashimoto’s thyroiditis group compared with the control group. Similar findings were reported in a study by Agha-Hosseini et al., where they suggested that the presence of corticotropin-releasing hormone in thyroid lesions could account for the hyperproduction of cortisol in patients with Hashimoto’s thyroiditis. 17
Women with Hashimoto’s thyroiditis at reproductive age are at a higher risk of diminished ovarian reserve. However, in contrast, a meta-analysis conducted by Li et al. revealed no significant difference in ovarian reserve parameters between women with Hashimoto’s thyroiditis and healthy control groups. Nonetheless, women within the reproductive age range in Hashimoto’s thyroiditis group exhibited decreased anti-Müllerian hormone levels and increased FSH levels. Premature ovarian aging was associated with anti-TPO (TPOAb) positivity in this group. 18 Additionally, studies have indicated an association between Hashimoto’s thyroiditis and hyperprolactinemia. 19
Saran et al. demonstrated that E2 and T levels decreased, while TSH and PRL levels increased in hypothyroid women. However, upon achieving euthyroidism, E2 and T levels increased, and TSH and PRL levels decreased. Although FSH and LH levels also increased after reaching a euthyroid state, this difference was not found to be statistically significant. 20
In our study, we found no significant difference in TSH, insulin, FSH, LH, E2, prog, T, DHEAS, or PRL levels between the euthyroid Hashimoto’s thyroiditis group and the control group. Reproductive hormone levels remained within the normal range when a euthyroid state was achieved. Thus, consistent with Brown et al.’s findings, the use of LT4 treatment shows potential benefits for both pregnant and non-pregnant women in the presence of thyroid autoimmunity. 5
Conclusion
In women living with obesity, it is important to screen for Hashimoto’s thyroiditis and achieve euthyroidism through effective LT4 treatment to promote a healthy reproductive system and improve fertility rates.
Footnotes
Acknowledgments
The authors thank Mr. Ertan Koc for his contribution to statistical analysis.
Authors’ Contributions
F.A.: Software, resources, investigation, writing—original draft, writing—review and editing, project administration. Z.B.T.: Software, resources, investigation, visualization, writing—review and editing, project administration. V.C.C.: Conceptualization, methodology, software, visualization, writing—review and editing, project administration. H.Z.: Conceptualization, methodology, software, visualization, writing—review and editing, project administration. All authors listed have contributed sufficiently to the project to be included as authors, and all those who are qualified to be authors are listed in the author byline.
Author Disclosure Statement
The authors declare no conflicts of interest (financial or other).
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.