
Abstract
Objective:
The HEPAKID index, a novel diagnostic tool with a sensitivity of 82% and specificity of 62% for detecting nonalcoholic fatty liver disease in obese adolescents. Our study aimed to explore the potential relationship between the HEPAKID index and risk factors contributing to the development of cardiovascular disease in obese adolescents with metabolic syndrome.
Methods:
This prospective cross-sectional study, conducted at two medical centers from December 2023 to March 2024, included 208 obese adolescents, with a median age of 14.5 years and an average body mass index (BMI) of 30.57 kg/m2.
Results:
Elevated HEPAKID index values were found in obese adolescents with metabolic syndrome, showing positive associations with BMI, waist and hip circumferences, alanine aminotransferase level, fasting insulin, and homeostasis model assessment for insulin resistance. In those with metabolic syndrome, waist circumference (WC) and homeostasis model assessment for insulin resistance were significant independent variables linked to the HEPAKID index, while WC was the sole influencer in the nonmetabolic syndrome group. Multivariate logistic regression highlighted systolic and diastolic blood pressures, triglycerides, high-density lipoprotein cholesterol, and the HEPAKID index as reliable predictors of metabolic syndrome. A predictive cutoff value of 60.84 for the HEPAKID index showed 61.7% sensitivity and 59.1% specificity in identifying metabolic syndrome.
Conclusions:
Our study highlighted the potential value of the HEPAKID index in combination with other clinical parameters for predicting metabolic syndrome in obese adolescents, underscoring its role as a valuable screening tool. Furthermore, our findings revealed a correlation between the HEPAKID index and insulin sensitivity in this high-risk population.
Introduction
Childhood obesity stands as a significant and escalating public health challenge globally, particularly prevalent among children and adolescents in recent times. Extensive research has firmly established the link between childhood obesity and the co-occurrence of cardiovascular risk diseases, underscoring the critical need for comprehensive intervention strategies. 1 –3 In obesity, the emergence of metabolic syndrome (MetS) is particularly worrying, a complex condition that poses significant health risks. Therefore, the early detection and management of MetS components, especially in obese adolescents, assume paramount importance as a preventive measure against the development of cardiovascular complications in adulthood. 4 MetS comprises a constellation of abnormalities encompassing augmented adiposity, insulin resistance, elevated blood pressure (BP), dyslipidemia, nonalcoholic fatty liver disease (NAFLD), and cardiovascular disease, collectively contributing to the burden of disease in affected individuals. 5 Notably, NAFLD is recognized as a prominent element of MetS, with epidemiological studies indicating a substantially elevated prevalence of NAFLD in children with MetS compared to their counterparts without the MetS. 6
In recent investigations conducted by Oses et al., 7,8 a notable association has been delineated between the HEPAKID index and NAFLD detected via liver magnetic resonance imaging in children. The HEPAKID index, a novel and cost-effective diagnostic tool tailored for primary care physicians, exhibited detection for NAFLD, integrating diverse parameters including anthropometric measurements, sociodemographic elements, and lifestyle factors, thereby establishing its utility as a valuable screening instrument. This facilitates the early recognition of NAFLD, enabling timely therapeutic interventions. Nevertheless, no data exists regarding the correlation between the HEPAKID index and risk factors predisposing to cardiovascular disease development in obese adolescents. Our hypothesis is that the HEPAKID index may serve as a predictive tool for MetS in adolescents, given its efficacy in identifying NAFLD in overweight and obese pediatric populations. Therefore, we aimed to study the potential association between the HEPAKID index and risk factors contributing to the onset of cardiovascular disease in obese adolescents with MetS.
Materials and Methods
Participants
This prospective cross-sectional study was conducted at the outpatient pediatric clinic of Konya Beyhekim Training and Research Hospital and the pediatric endocrinology clinic of Selçuk University Hospital from December 2023 to March 2024. The determination of the sample size for this study was predicated upon an estimated prevalence of obesity in adolescents, as outlined in a prior publication, 9 which reported a prevalence rate of 11.8%. Essential parameters, encompassing a 5% alpha error, a 10% effect size, and a power level of 80%, were defined utilizing G*Power 3.1.9.7 software. The requisite minimum sample size, computed based on these criteria, was ascertained to be 202 adolescents. The number of patients in the study matched the sample size calculated.
A total of 208 obese adolescents were randomly selected from the adolescent population, and subsequently categorized into groups with and without MetS. In this investigation, we assessed MetS in adolescents using the consensus criteria recognized by the International Diabetes Federation (IDF). According to the IDF guidelines, a diagnosis of pediatric MetS necessitates the presence of abdominal obesity [waist circumference (WC) ≥ the 90th percentile or the adult cutoff if lower] and at least two of the following clinical indicators: low levels of high-density lipoproteincholesterol (<40 mg/dL), elevated triglycerides (≥150 mg/dL), increased fasting plasma glucose levels (≥100 mg/dL or a confirmed diagnosis of type 2 diabetes), and elevated BP (systolic BP ≥130 mmHg or diastolic BP ≥85 mmHg). 10
Exclusion criteria for the study encompassed individuals displaying clinical or laboratory signs of systemic illnesses, those undergoing medication regimens, or individuals with known conditions affecting insulin action or secretion. Approval for the study protocol was obtained from the Selcuk University Ethics Committee (approval number 2023/557), with signed informed consent forms acquired from the parents of the participating adolescents.
Sociodemographic definitions
In accordance with the study conducted by Oses et al., 7 the identification of individuals belonging to an ethnic minority was based on specific criteria, including having a mother of foreign nativity from a low or middle-income country. Pertinent perinatal variables and any familial predisposition to obesity and diabetes were collected through a structured questionnaire and review of clinical records. Information regarding the maternal educational attainment and birthplace was gathered through questionnaire responses. In this study, the term sugar-sweetened beverages (SSB) encompasses a variety of products, including soft drinks, energy drinks, and sweetened fruit juices. The evaluation of SSB consumption involved quantifying the daily intake of these beverages, specifically focusing on soft drinks, sweetened juices, and energy drinks. Patients who had consumed a minimum of one serving of any SSB per week in the preceding month were categorized as SSB drinkers. 11 Following this classification, children were grouped based on their SSB consumption status.
The average daily durations of screen time, including activities like watching TV, playing on-screen games, browsing the internet, and using mobile phones, were self-reported by both the adolescents and their families. Postassessment, adolescents were stratified according to their adherence to World Health Organization guidelines on-screen time for adolescents, distinguishing between those meeting (<2 hr/day) and those not meeting (≥2 hr/day) the recommended thresholds. 12
The HEPAKID index
The HEPAKID index, as defined by Oses et al., 7 was computed using the survey data gathered, following the formula detailed in their work. The calculation process for the HEPAKID index was carried out utilizing the designated calculator as specified in the publications by Oses et al. (https://bit.ly/2AQTUPa). Gestational age at delivery, ethnic minority background, waist-to-height ratio (WHtR), screen time, and consumption of SSB were inputted into the designated fields, and the resultant HEPAKID index values were documented. The parameter of cardiorespiratory fitness was not incorporated in our study.
Anthropometric measurements
Anthropometric measurements were conducted for all subjects, with height and weight measurements obtained using a Harpenden stadiometer (Holtain Limited, Crymych, UK) and an electronic scale. Body mass index (BMI) was determined by dividing the individual’s weight in kilograms by the square of their height in meters. Individuals with BMIs at or above the 95th percentile, based on reference curves for Turkish adolescents, were classified as obese. 13 Standard deviation scores for BMI (BMI-SDS) were computed from national growth charts. 14 The measurement of WC was taken at the midpoint between the lowest rib and the iliac crest at the end of a gentle exhalation, while hip circumference (HC) was measured over the great trochanters. Following these measurements, the WHtR and the waist-to-hip ratio (WHR) were calculated as the WC divided by the height, and the WC divided by the HC, respectively. 15 Pubertal developmental stage was assessed using the Tanner criteria, with all patients exhibiting sexual maturation between Tanner stages 2 and 5. BP measurements were obtained from each participant after a standardized rest period of at least 5 min, utilizing a sphygmomanometer equipped with a properly sized pediatric cuff. These measurements were taken while the subjects were in a seated and relaxed state, ensuring standardized conditions for the assessment of BP.
Laboratory assessment
Blood samples were obtained in the morning through venipuncture after an overnight fasting period to analyze serum glucose, insulin levels, and other relevant parameters. The serum lipid levels were measured using standard enzymatic techniques on an Abbott Diagnostics c16000 chemistry analyzer. Serum insulin concentrations were assessed with the IMMULITE immunoassay system from Siemens Healthcare Diagnostics.
Insulin sensitivity measurement
Insulin resistance was assessed by calculating the homeostasis model assessment of insulin resistance (HOMA-IR) using the formula: fasting insulin concentration (mU/mL) multiplied by fasting glucose concentration (mmol/L), divided by 22.5. 16 Insulin resistance was defined as the levels of the HOMA-IR >3.16. 17
Statistical analysis
The assessment of parameter distribution was conducted via the Shapiro–Wilk test. Descriptive statistics were presented as mean ± standard deviation for normally distributed data and as median with interquartile range (IQR) for non-normally distributed data, while categorical variables were summarized using frequency and percentage values. Comparative analyses involved the use of either the Mann–Whitney U test or independent t-test for continuous variables and the chi-squared test for categorical variables. Bivariate associations among continuous variables were explored using Spearman’s rank correlation test. Univariate and multivariate logistic regression analyses aimed to identify potential risk factors associated with MetS, with significant variables from the univariate analysis included in a forward stepwise multivariate logistic regression model. The predictive capability of the HEPAKID index for detecting MetS in obese adolescents was evaluated using the receiver operating characteristics (ROC) curve, determining the optimal cutoff value and calculating the area under the ROC curve for sensitivity and specificity. All statistical analyses were performed using the SPSS software package for Windows, version 21.0. Figures were created in GraphPad Prism 9.0.
Results
Demographic and laboratory characteristics of participants
The study cohort comprised a total of 208 obese adolescents, with 89 females and 119 males, exhibiting a median age of 14.5 years (IQR: 3.15) and a median BMI of 30.57 kg/m2 (IQR: 5.85). Among these participants, 81 individuals (38.9%) were diagnosed with MetS, as detailed in Table 1. Sex, age, and BMI-SDS values of these two groups of obese adolescents, with and without MetS, were similar. Upon comparison between obese adolescents with and without MetS, no significant variations were noted in various factors such as gestational age, birth weight, screen time, prematurity, small for gestational age (SGA) frequencies, and breastfeeding duration. However, a notable difference was observed in the SSB consumption, with obese adolescents with MetS showing higher intake (P = 0.012). In obese adolescents with MetS, hypertension was present in 70.4%, dyslipidemia in 72.8%, and dysglycemia in 61.7%, whereas in obese adolescents without MetS, the prevalence of hypertension was 21.3%, dyslipidemia was 24.8%, and dysglycemia was 31.5%. When comparing the two groups, as expected, hypertension (P < 0.0001, OR: 8.769, 95% CI: 4.604–16.704), dyslipidemia (P < 0.0001, OR: 8.132, 95% CI: 4.305–15.361), and dysglycemia (P < 0.0001, OR: 3.508, 95% CI: 1.957–6.290) were significantly higher in obese adolescents with MetS.
Sociodemographic, Lifestyle, and Clinical Features of Obese Adolescents With and Without Metabolic Syndrome
Values are expressed as mean ± standard deviation or median (IQR). Significance is determined by P < 0.05 and shown with bold characters.
GGT, gamma-glutamyl transferase; HbA1c, glycosylated hemoglobin; IQR, interquartile range; SDS, standard deviation scores; TSH, thyroid-stimulating hormone.
Furthermore, obese adolescents with MetS exhibited distinct metabolic and anthropometric characteristics, including elevated WC, WHR, WHtR, systolic and diastolic BPs, serum ALT, total cholesterol, triglyceride, fasting glucose, insulin levels, and HOMA-IR, along with lower levels of high-density lipoprotein cholesterol compared to their non-MetS counterparts (Fig. 1). Moreover, the HEPAKID index values were significantly higher in the obese group with MetS (Fig. 2). Notably, both MetS and non-MetS groups displayed positive correlations between the HEPAKID index and various parameters such as BMI, WC and HC, ALT level, fasting insulin, and HOMA-IR, as outlined in Table 2, underscoring the interplay between metabolic health indicators and obesity-related factors in this adolescent population.
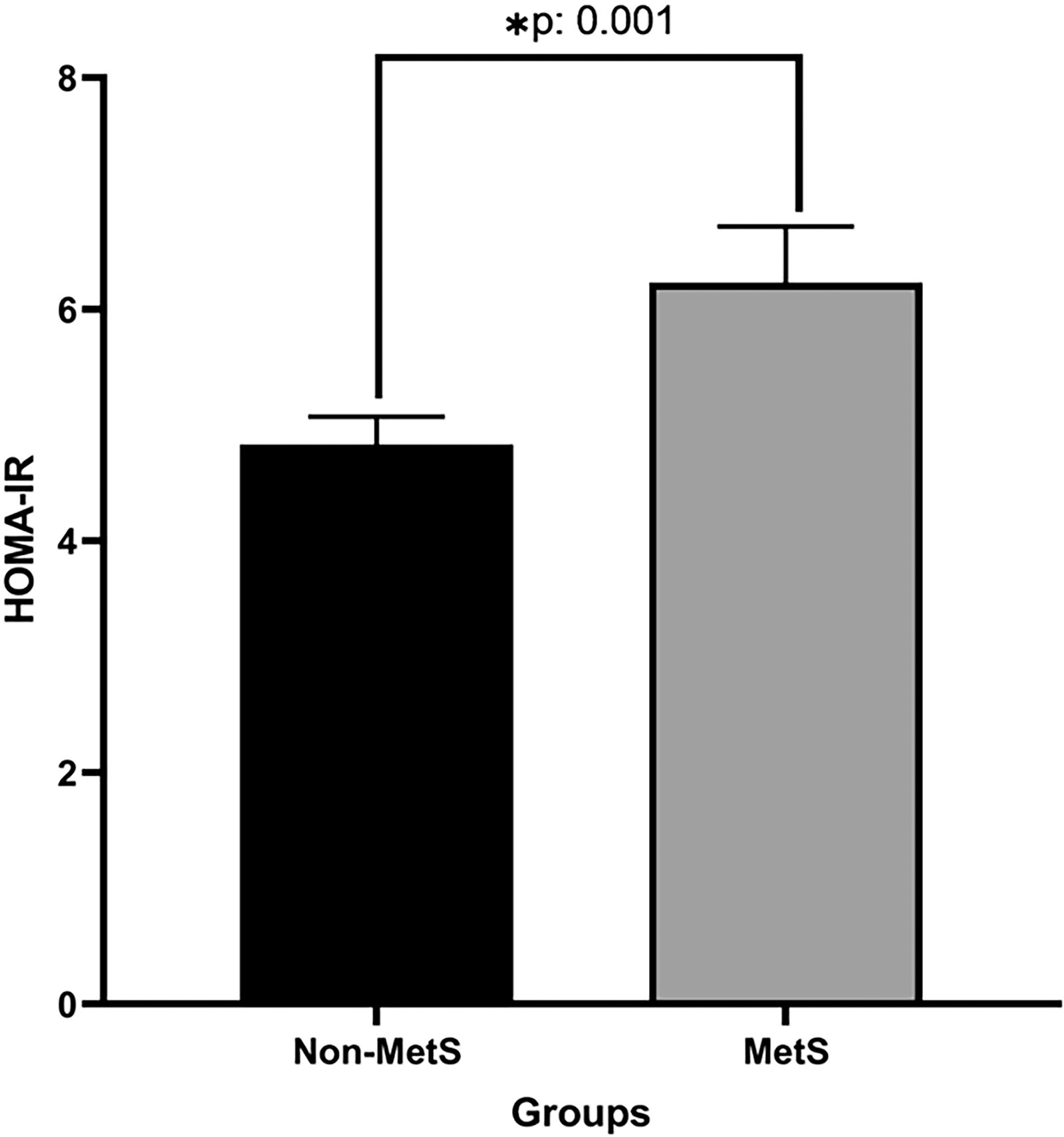
HOMA-IR in obese adolescents with and without metabolic syndrome. HOMA-IR, homeostasis model assessment of insulin resistance.

The HEPAKID index in obese adolescents with and without metabolic syndrome.
Spearman’s Correlations Between the HEPAKID Index and Metabolic Variables in Obese Adolescents
Significance is determined by P < 0.05 and shown with bold characters.
To ascertain the variables independently influencing the HEPAKID index, a multiple regression analysis model was conducted within the MetS group. A stepwise regression revealed that WC (β = 0.487, P < 0.001) and HOMA-IR (β = 0.204, P = 0.038) were the independent variables significantly associated with the HEPAKID index. In the non-MetS group, WC (β = 0.457, P < 0.001) was identified as the only independent variable influencing the HEPAKID index.
Logistic regression of factors for risk of MetS in obese adolescents
In the logistic regression analysis to assess the risk factors for MetS in obese adolescents, variables such as SSB consumption, weight, BMI, WC, WHR, WHtR, systolic and diastolic BPs, fasting glucose and insulin levels, HOMA-IR, triglycerides, high-density lipoprotein cholesterol, ALT, and HEPAKID index were statistically significant predictors. Multivariate logistic regression analysis identified systolic and diastolic BPs, triglycerides, high-density lipoprotein cholesterol, and HEPAKID index as the best independent predictors of MetS in obese adolescents (Table 3).
Results of Univariate and Multivariate Analyses for Risk of Metabolıc Syndrome in Obese Adolescents
Significance is determined by P < 0.05 and shown with bold characters.
Evaluation of ROC curves utilizing the HEPAKID index and insulin sensitivity indexes
The discriminatory potential of the HEPAKID index and HOMA-IR in distinguishing between the MetS and non-MetS groups was found to be reasonably effective. The calculated area under the curve (AUC) for the HEPAKID index was 0.640 (95% CI: 0.562–0.717, P = 0.001), with a corresponding threshold value of 60.84. Sensitivity and specificity metrics for the HEPAKID index were determined to be 61.7% and 59.1%, respectively. Similarly, the AUC for HOMA-IR was computed as 0.643 (95% CI: 0.568–0.719, P = 0.001), with sensitivity and specificity values of 64.2% and 63%, respectively, as depicted in Figure 3.
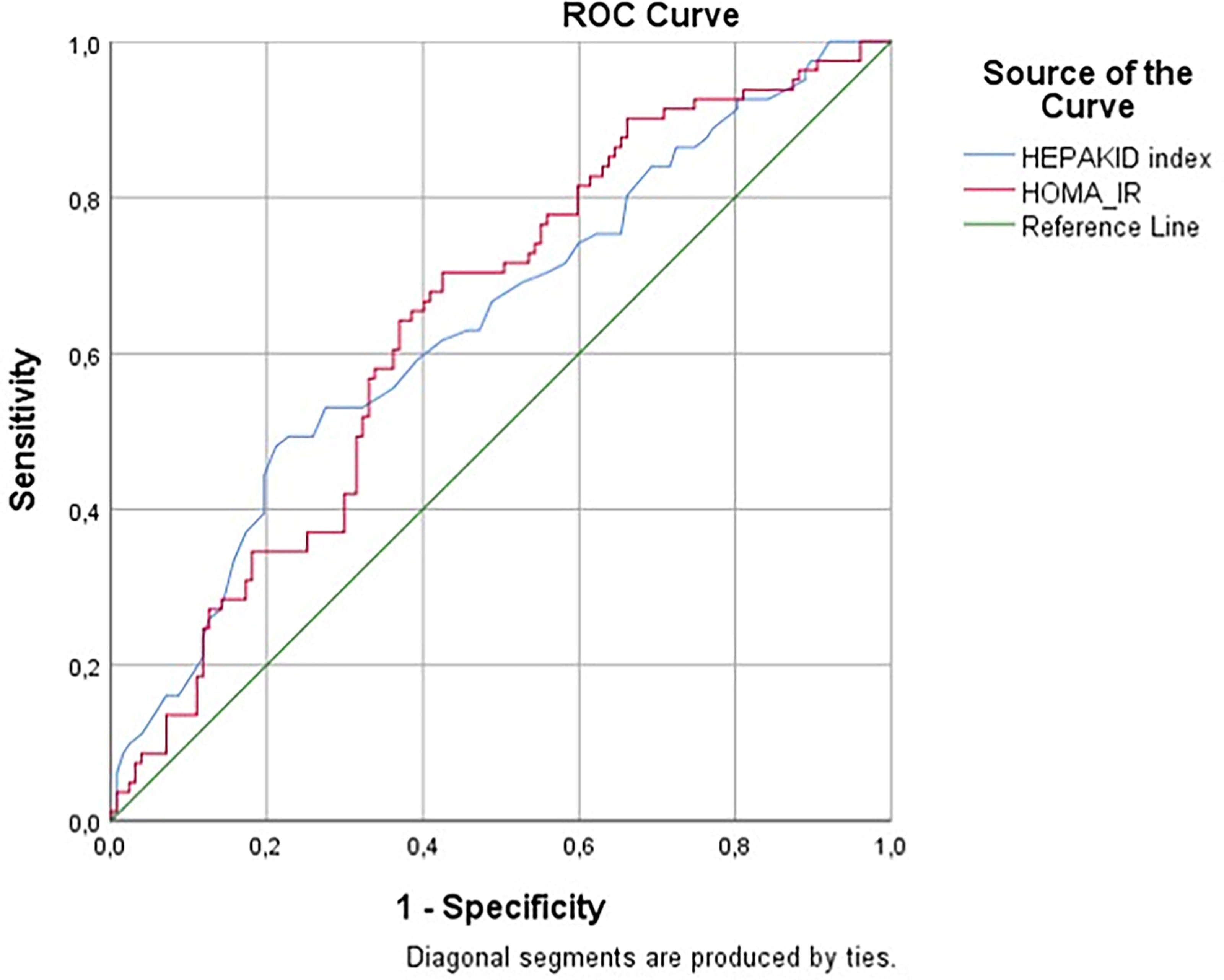
ROC curve analysis of HEPAKID index and HOMA-IR for predicting metabolic syndrome in obese adolescents. ROC, receiver operating characteristics.
Comparative analysis of anthropometric and metabolic parameters in obese adolescents stratified by HEPAKID ındex values ≥60.84 and <60.84
In our study, patients were stratified into two distinct cohorts according to the established HEPAKID index threshold of 60.84, following which a comprehensive evaluation of various parameters was conducted. Upon comparative analysis of the two delineated groups, no statistically significant associations were discerned with respect to gender, hypertension, and dyslipidemia (P > 0.05). However, notable correlations were observed in relation to the presence of SSB consumption, extended screen time exceeding 2 hr, dysglycemia, SGA, and the manifestation of MetS, as elucidated in detail within Table 4.
Comparative Analysis of Significant Parameters in Obese Adolescents Stratified by HEPAKID Index Values ≥60.84 and <60.84
Significance is determined by P < 0.05 and shown with bold characters.
Discussion
Current investigation highlights that obese adolescents diagnosed with MetS exhibit elevated levels of the HEPAKID index. Additionally, our study uncovers significant positive associations between the HEPAKID index and various parameters such as BMI, BMI-SDS, WC and HC, ALT level, fasting insulin, and HOMA-IR. Notably, we have identified a predictive cutoff value for the HEPAKID index above 60.84 to anticipate the presence of MetS in obese adolescents, with a sensitivity of 61.7% and a specificity of 59.1%. Importantly, our study is the first to establish a link between MetS and the HEPAKID index, a prediction score based on sociodemographic, anthropometric, and lifestyle factors in obese adolescents. Furthermore, our findings underscore the significance of the HEPAKID index, alongside traditional cardiovascular risk factors, as a key predictor of MetS onset in this population. We also observed higher consumption of SSB among obese adolescents with MetS compared to those without the MetS.
The HEPAKID index, originally developed in Spain for NAFLD screening in prepubertal children, integrates sociodemographic, anthropometric, and lifestyle parameters and offers ease of application. Prior research has validated that a HEPAKID index value ≥25 effectively indicates NAFLD in children with overweight and obesity. 7 But, to date, the applicability of the HEPAKID index in adolescents and its comparison in obese adolescents with and without MetS remain unexplored. Our study reveals that systolic and diastolic BPs, triglycerides, high-density lipoprotein cholesterol, and the HEPAKID index are independent variables indicating the risk of MetS in obese adolescents. These findings align with previous studies 18 and introduce a novel insight, demonstrating that the HEPAKID index, with a cutoff value of 60.84, is a valuable predictor of MetS in obese adolescents.
The intricate interplay between NAFLD and MetS in pediatric populations remains a subject of ongoing investigation due to its complex and incompletely understood nature. Existing literature has highlighted the coexistence of NAFLD and MetS in children, where NAFLD is often accompanied by key components of MetS such as insulin resistance, central obesity, and dyslipidemia. 19,20 Earlier study has demonstrated a significant relationship between the severity of insulin resistance and histological features of NAFLD, with a higher risk of MetS observed in individuals with severe steatosis. 21 In our current study, we observed that the group of adolescents diagnosed with MetS exhibited substantially elevated HOMA-IR values compared to those without MetS. Furthermore, our findings underscored the significant independent effect of insulin resistance on the emergence of MetS in obese adolescents. Importantly, adolescents with MetS displayed a notably more unfavorable cardiovascular risk profile in comparison to their counterparts without MetS. Notably, a novel discovery in our study was the positive correlation identified between the HEPAKID index and insulin resistance in both obese adolescents with and without MetS. Additionally, our study revealed HOMA-IR as one of the independent predictors of the HEPAKID index.
The HOMA-IR test has been acknowledged for its considerable limitations in accurately predicting insulin resistance and beta-cell dysfunction. A primary challenge associated with this assessment is the nonstandardized nature of its cutoff values, which can exhibit substantial variability influenced by demographic factors, sex, vitamin D deficiency, and the presence of co-morbid conditions such as NAFLD and polycystic ovary syndrome. Furthermore, the reliability of HOMA-IR is notably diminished in specific patient populations, particularly among individuals undergoing insulin therapy, those with complete beta-cell destruction, and patients exhibiting impaired glucose tolerance. In light of these considerations, it has been suggested that utilizing cutoff values for HOMA-IR based on cardiometabolic risk rather than relying solely on population distribution percentiles to define insulin resistance may enhance its clinical applicability in identifying patients with multiple metabolic risk factors who are at an increased risk for metabolic and cardiovascular complications. 22,23 The findings of our study highlight the performance of both the HEPAKID index and HOMA-IR in differentiating between MetS and non-MetS groups among obese adolescents. The calculated AUC values of 0.640 for HEPAKID index and 0.643 for HOMA-IR suggest that both indices possess a reasonable, albeit modest, discriminatory ability. While sensitivities of 61.7% for HEPAKID index and 64.2% for HOMA-IR coupled with specificities of 59.1% and 63%, respectively, indicate their potential to contribute to clinical assessments, these values alone highlight the need for caution when relying solely on these indices for definitive clinical decisions. Although neither index reaches optimal thresholds typical of highly reliable diagnostic tests, they may serve as adjunctive tools within a broader clinical framework. In clinical practice, indices such as HEPAKID could help identify individuals at higher risk of MetS when combined with additional factors such as lifestyle behaviors (e.g., SSB consumption, screen time) and anthropometric measurements. Furthermore, the incorporation of these indices into routine evaluations could facilitate early identification and targeted interventions for at-risk adolescents.
The utilization of the WHtR as a straightforward and efficacious diagnostic tool for evaluating central obesity and cardiometabolic risk has garnered significant attention in both adult and pediatric populations. Notably, the determination of appropriate cutoff values for WHtR varies among different populations, as highlighted in a recent study. This comprehensive examination emphasized the necessity of utilizing population-specific cutoff values for WHtR in childhood rather than relying on the conventional threshold of 0.50. 24,25 A recent study 24 elucidated the importance of establishing international optimal cutoffs for WHtR in expecting cardiometabolic risk in individuals, underscoring the need for tailored approaches in diverse demographic groups. In our current investigation, we observed a notable disparity in the WHtR, a key component of the HEPAKID index, between obese adolescents with and without MetS. Specifically, obese adolescents diagnosed with MetS exhibited significantly higher values for BMI, WC, and WHR compared to their counterparts without the syndrome. Moreover, our study revealed positive associations between various anthropometric measurements, including BMI, WC and HC, and WHR, with the HEPAKID index in both obese adolescents with MetS and those without MetS. These findings underscore the intricate relationship between anthropometric indicators and MetS in obese adolescents, shedding light on the potential utility of these measures in assessing cardiometabolic risk profiles within this population.
MetS, a multifaceted condition characterized by abdominal obesity, elevated BP, dyslipidemia, and increased fasting blood glucose levels, poses a significant health concern in children and adolescents. Despite its clinical relevance, the lack of consensus regarding the precise definition of MetS in this demographic group underscores the complexity of its diagnosis and management. 26 In our investigation, we employed the IDF diagnostic criteria to identify MetS in obese adolescents, aiming to enhance diagnostic accuracy and clinical understanding within this population.
The etiology of MetS is believed to stem from an intricate interplay between genetic predisposition and environmental influences. Notably, many modifiable environmental risk factors, alongside genetic susceptibilities, are implicated in the pathogenesis of MetS. Factors such as gestational age, birth weight, lifestyle choices during adolescence, sedentary behaviors, and the consumption of fructose and SSB have been proposed as contributing elements to the development of MetS. 26 –30 Early studies have highlighted associations between low birth weight, a family history of diabetes, and the onset of MetS in children and adolescents, emphasizing the multifactorial nature of this syndrome. 28,31 In our current study, we explored various factors, including family history of obesity and diabetes, screen time, gestational age, birth weight, and dietary habits among obese adolescents with and without MetS. While no significant disparities were observed in the family history of obesity and diabetes between the two groups, a noteworthy finding emerged regarding higher consumption of SSB among obese adolescents with MetS. Furthermore, our analysis revealed elevated systolic and diastolic BPs, increased serum total cholesterol and triglyceride levels, decreased high-density lipoprotein cholesterol levels, and higher fasting glucose and insulin levels in obese adolescents with MetS compared to their counterparts without the syndrome. Interestingly, our study identified a significant correlation between fasting insulin levels and the HEPAKID index, underscoring the potential utility of this index as a predictive tool for MetS in obese adolescents. Notably, the establishment of a cutoff HEPAKID index value (>60.84) as a predictor of MetS facilitated the identification of key determinants, including SSB consumption, prolonged screen time, dysglycemia, and SGA, in this at-risk population.
The limitations of our study necessitate careful consideration. First, due to the cross-sectional nature of our study, we were unable to explore the temporal dynamics of the relationship between MetS and the HEPAKID index. Prospective studies are indispensable to validate our findings and elucidate potential relations between MetS and the HEPAKID index. Second, as our study sample comprised obese adolescents recruited from outpatient clinics, the generalizability of our results to the broader adolescent population is constrained. Future research endeavors should prioritize determining the cutoff values of HEPAKID index to assess the risk of MetS in adolescents across diverse societal contexts. Last, our study diagnosed MetS based on IDF criteria, with no assessment conducted for NAFLD as it fell beyond the scope of our research focus.
Conclusions
In conclusion, our study underscored the utility of the HEPAKID index in conjunction with other clinical parameters for predicting MetS in obese adolescents. Furthermore, our findings revealed a correlation between the HEPAKID index and insulin sensitivity in this at-risk population. Nevertheless, further prospective studies encompassing larger cohorts with extended follow-up periods are indispensable to elucidate the clinical applicability of the HEPAKID index in obese adolescents. By addressing these research gaps, a more comprehensive understanding of the predictive value and clinical implications of the HEPAKID index in the MetS among adolescents can be achieved. Considering the potential role of the HEPAKID index as a predictive tool for MetS in adolescents, it is essential to evaluate its utility in comparison to targeted treatment strategies for obesity, hypertension, and other cardiovascular risk factors. By comparing the predictive capabilities of the HEPAKID index and HOMA-IR with the outcomes of targeted treatments, we can better understand their clinical relevance and enhance the management of metabolic health in this population.
Footnotes
Authors’ Contributions
S.S. and M.B. provided the study inference, conducted the statistical analysis, and wrote the article. S.S., M.B., and A.F.Y. conducted the study. All authors contributed to interpreting the result and finalizing the article.
Author Disclosure Statement
The authors did not receive support from any organization for the submitted work.
Funding Information
The authors declare they have no financial interests.