
Abstract
The prevalence of metabolic syndrome (MetS) is increasing worldwide. This is becoming a significant public health problem. In Morocco, it is estimated that 94.3% of people aged between 18 and 69 years have at least one risk factor for non-communicable diseases. This systematic review and meta-analysis aimed to measure the overall prevalence of MetS in the Moroccan population. This systematic review included studies published up to March 20, 2024. Data were retrieved from international databases, including EMBASE, Scopus, and MEDLINE/PubMed. Searches were conducted using the keywords “metabolic syndrome,” “prevalence,” and “Moroccan.” The overall prevalence of MetS was calculated using a random-effects model to account for heterogeneity across studies. A total of 32 studies were conducted in Morocco, with a sample of 13 889 participants. The overall prevalence of MetS in the Moroccan population was 34.68%, with 39.66% in women and 30.51% in men. The pooled prevalence in apparently healthy individuals was 29.41%, which increased to 61.84% in patients with type 2 diabetes, 58.81% in patients with general obesity, 47.09% in patients with hypertension, and 28.29% in patients with rheumatoid arthritis. For an average age under 40 years, the pooled prevalence was 25.44%; for an average age between 40 and 50 years, the pooled prevalence was 25.52%; and for an average age of 50 years or more, the prevalence was 43.23%. The results of this study highlight the huge prevalence of MetS in the Moroccan population, with significant variations depending on the subgroups studied, diagnostic criteria used, and age group, highlighting the urgent need to develop and implement effective strategies to tackle this major public health challenge in Morocco.
Introduction
Metabolic syndrome (MetS) is a group of metabolic disorders, which collectively expose to a high risk of developing atherosclerotic cardiovascular disease, insulin resistance, and type 2 diabetes, it is linked to an elevated risk of getting vascular as well as neurological complications such as stroke. 1 MetS is diagnosed when an individual exhibits three or more of the following components: hypertension, hyperglycemia, central obesity, and dyslipidemia. 2 –7 MetS is a significant global health burden having a considerable influence not only on human health but also on health care costs worldwide. 1,8
The prevalence of MetS may vary according to country, geographical location, 9 ethnicity, sex, cultural behavior, lifestyle, age, and the diagnostic criteria and thresholds used in different definitions. 10,11
In Morocco, the population is 36.8 million, 34.7% is aged under 19 and 24.1% aged 50 and over with a sex ratio equal to 0.97. While the average life expectancy is 76 years. 12 Morocco is currently experiencing a nutritional transition, marked by a gradual shift in dietary habits from the traditional Mediterranean diet to a more modern, Western-style diet, which is characterized by high consumption of carbohydrates and fats. 13 –16
This transition is accompanied by significant demographic and epidemiological changes, including an increase in morbidity and mortality related to non-communicable diseases (NCDs). 17 According to the World Health Organization (WHO, 2022), NCDs account for 84% of deaths in Morocco, 18 with 38% of these attributable to cardiovascular diseases. 19
The Stepwise survey (2017–2018) showed that among the Moroccan population the prevalence of hypertension, diabetes, overweight, obesity, and hypercholesterolemia were 29.3%, 10,6%, 33%, 20%, 10,6%, respectively. Whereas 76.5% of people ate less than five fruits and vegetables a day. 20 These statistics highlight the growing public health and economic concerns associated with these transitions. 21,22
Despite several national surveys assessing the prevalence of MetS in various regions of Morocco, an overall national prevalence of MetS among the Moroccan population has yet to be established. For instance, the National Health Survey has been referenced as a source of information on cardiovascular risk factors, although its specific findings on MetS remain unclear. 20 Determining this prevalence is essential, as targeted interventions could help prevent or even reverse its progression. The objective of this survey is to provide an estimation of the pooled prevalence of MetS in Morocco. A systematic review and meta-analysis were carried out according to various criteria, including the National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III), 4 the International Diabetes Federation (IDF), 23 the Revised National Cholesterol Education Program Adult Treatment Panel III (Revised NCEP-ATP III), 7 European Group for the Study of Insulin Resistance (EGIR), 24 the American Heart Association/National Heart, Lung, and Blood Institute (AHA/NHLBI) Scientific Statement, 7 the World Health Organization (WHO) 2,25 the American Association of Clinical Endocrinologists (AACE), 3 and Joint Interim Statement (JIS). 6 The goal is to provide data on the estimated pooled prevalence of MetS and its trends to plan and implement targeted prevention and management strategies as part of the national multi-sectoral strategy for the prevention and control of NCDs.
Material and Methods
Registration
The study has been undertaken by the preferred reporting Items for Systematic Reviews and Meta-Analyses PRISMA standards. 26 This review protocol was entered into the International Prospective Register of Systematic Reviews (PROSPERO, n˚. CRD42021275176).
Eligibility criteria
All relevant original research articles, published up to March 20, 2024, about the prevalence of MetS in the adult population residing in Morocco were eligible. There were no restrictions on study type, or definitions used to determine MetS, clinical status, gender, or publication language. Excluded materials included book chapters, encyclopedias, book reviews, journals, editorials, case reports, case series, letters, commentaries, studies reporting the prevalence of MetS in non-Moroccans or Moroccans living outside Morocco, and replication studies.
Data sources and search strategy
The search strategy and data sources were as follows: Before March 2024, we carried out a systematic search to determine the prevalence of MetS in Moroccan adults. Relevant research articles were identified using EMBASE, Scopus, and MEDLINE/PubMed databases. The search was performed using terms such as: “metabolic syndrome”, “prevalence” and “Moroccan population”. In addition, their equivalents were connected with the prevalence of MetS. No language restrictions were imposed. In addition, one person performed the research, and another checked the results.
Study selection
The eligibility of articles was independently assessed by two reviewers. Initially, they screened titles and abstracts to refine the search strategy. Duplicates identified across various bibliographic databases were removed using Zotero before proceeding with the selection process. Articles were retained if one of the reviewers felt they should be retained or if they were not certain about their eligibility based on the title and abstract alone. To minimize selection bias, a third reviewer arbitrated any disagreements regarding study eligibility during the full-text review stage. The reviewers’ agreement was quantified, and disagreements between reviewers during the initial screening were resolved by consensus. The selected articles were then examined by full-text review. We took into account decided by consent all definitions of MetS. We excluded studies in which the prevalence of MetS was reported in non-Moroccans or Moroccans not living in Morocco, and studies in which the prevalence of MetS was not reported. For studies with replicated results, only the most recent was included. We communicated by e-mail with the corresponding authors of studies that did not give enough information to improve the quality of the study, if possible. In case of disagreements, while selecting a study or extracting data, reviewers resorted to discussion to reach a consensus, however, if this proved ineffective, another author’s point of view was needed to provide a final decision.
Quality assessment (risk of bias)
Study quality was evaluated by the risk of bias calculations independently and blindly by two reviewers using the Joanna Briggs Institute tool for studies reporting prevalence data (JBI Critical Appraisal Checklist for Analytical Cross-Sectional Studies).
27
The checklist includes nine domains for assessing study quality. For each included study, the overall risk of bias was classified based on the following thresholds:
27
≥70% ‘yes’ responses: low risk of bias. ≤50% to 69% ‘yes’ responses: Moderate risk of bias. <50% ‘yes’ responses: high risk of bias.
Two reviewers independently evaluated the risk of bias, and a third reviewer determined any disagreements or discrepancies.
Statistical analysis
Meta-analysis was conducted using MedCalc software. For each of the studies, we extracted the total number of people who took part and the number of people who had the MetS. If the article did not provide any of these data, we obtained it using the prevalence of MetS. In cases with duplicate data, we considered the most recent study. In studies that evaluated the prevalence of MetS by more than two diagnostic criteria in the same population, all available values were aggregated. Random-effect models were used to calculate the weighted prevalence and 95% confidence intervals. 28 This model was chosen over a fixed-effects model because it accounts for both within-study variability and between-study heterogeneity. Given the anticipated differences in study populations, methodologies, and settings, the random-effects model was deemed more appropriate for synthesizing the data. 29 Quantitative exploration of inter-study heterogeneity was conducted using Cochrane’s Q and I 2. 30 Heterogeneity was classified into three categories based on the I 2 index: low heterogeneity (<25%), moderate heterogeneity (25%−75%), and high heterogeneity (>75%). Publication bias was assessed using funnel plots, Egger’s test, 31 and Begg’s ranking test. 32 The significance level was established at a p-value of less than 0.05.
Results
Study selection and study characteristics
A total of 834 articles were extracted from the database using an electronic search. After eliminating 59 duplicates, 775 articles were reviewed based on their titles and abstracts; 726 articles were excluded based on titles and abstracts that were irrelevant to the aim of our study. The full texts of the 52 articles were downloaded and assessed for inclusion. Nineteen articles were excluded after reading for various causes. Ultimately, 32 articles 33 –64 that met the inclusion criteria and provided data on the prevalence of MetS in Morocco were included in our meta-analysis (Fig. 1).
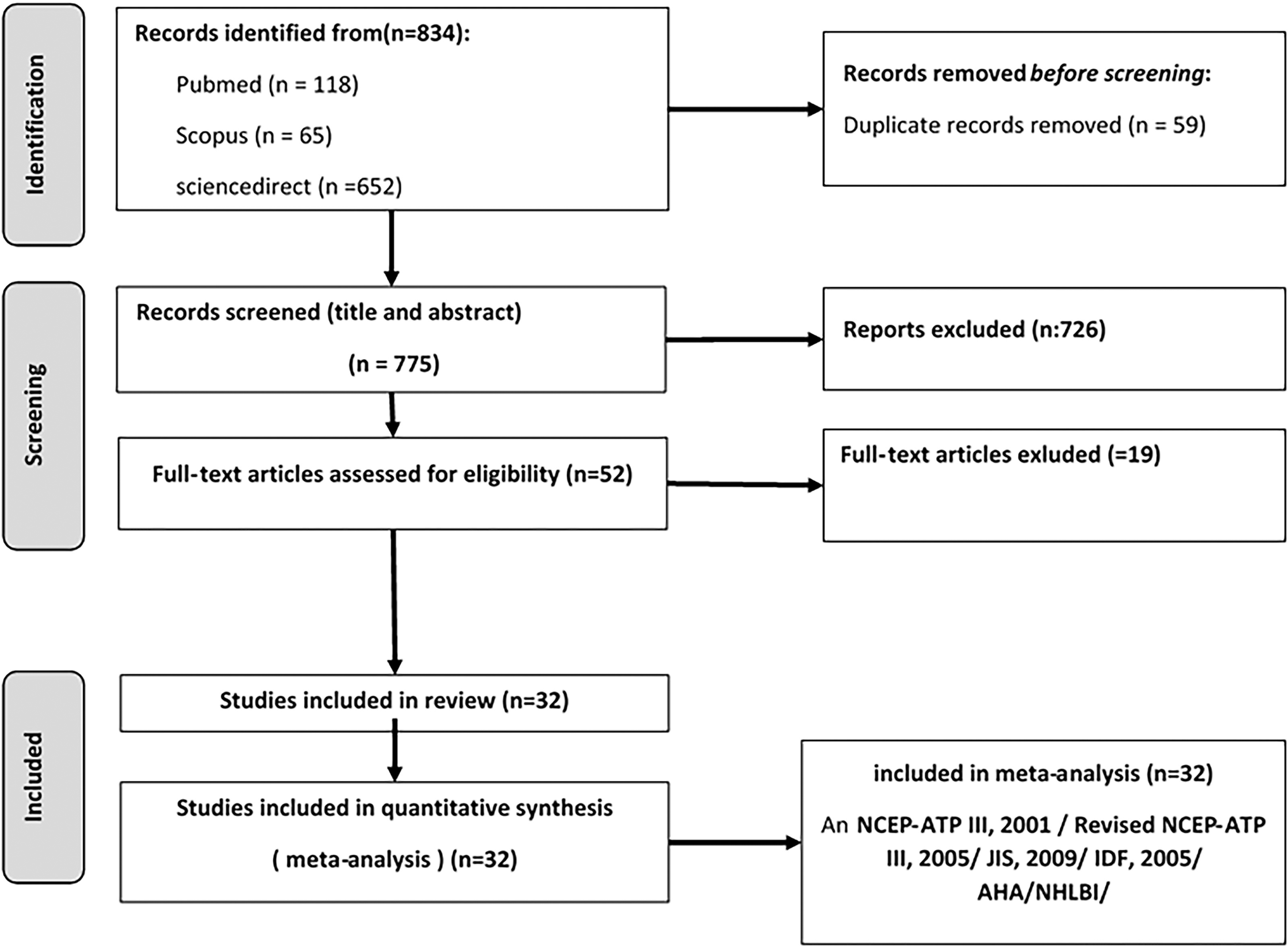
PRISMA flowchart diagram showing the study selection process.
The characteristics of the various studies on the prevalence of MetS in Morocco selected for inclusion in this systematic review are presented in Table 2. The prevalence rates of MetS were estimated according to the following criteria (Table 1): NCEP-ATP III, 4 Revised NCEP-ATP III, 7 IDF, 23 AHA/NHLBI, 7 EGIR, 24 WHO, 2,25 AACE, 3 and Joint Interim Statement 6 in 14, 7, 10, 1,1,1,1, and 5 articles, respectively, according to the 32 studies consulted. It is noteworthy to mention that 15 studies were reported on women; 17 involved a mixed population (men and women), of which 5 reported data including the entire study sample and 12 reported overall prevalence data on the one hand and data by sex (men or women) on the other.
Clinical Diagnostic Criteria for Metabolic Syndrome Based on Various Definitions
Insulin resistance (under hyperinsulinaemic euglycaemic conditions, glucose uptake below lowest quartile for background population under investigation).
Criteria for central obesity (waist circumference) are specific for each population, values given are for Middle East, Mediterranean.
Microalbuminuria (urinary albumin excretion rate ≥20 µg min–1 or albumin:creatinine ratio ≥20 mg g–1 later modified as 30 mg g–1).
AACE: American Association of Clinical Endocrinologists; AHA: American Heart Association; BMI: body mass index; EGIR: European Group for the Study of Insulin Resistance; HDL-C: HDL cholesterol; IDF: International Diabetes Federation; IFG: Impaired Fasting Glucose; IGT: Impaired Glucose Tolerance; JIS: Joint Interim Statement; NCEP-ATPIII: National Cholesterol Education Program’s Adult Treatment Panel III; NHLBI: National Heart, Lung, and Blood Institute; T2DM: type 2 diabetes mellitus; TG, triglyceride; WC: waist circumference; WHO: World Health Organization; WHR: waist/hip ratio.
Characteristic of Studies on the Prevalence of Metabolic Syndrome
In general, the participants were aged between 15 and 100 years old. Most studies have focused on urban areas, with 14 studies in central Morocco, 16 in northern Morocco, two in southern Morocco, and one in eastern Morocco.
The pooled prevalence of MetS in the Morocco population
A total of 13889 participants were included, of which 81.01% were women and 18.90% were men. The reported prevalence of MetS varies greatly, ranging from 2.67% to 77.69%; Table 2. After weighing and pooling the data, the overall prevalence of MetS, regardless of sex, age, and diagnostic criteria, was 34.68%; Figure 2. The results showed significant heterogeneity among studies. There was no significant evidence of publication bias (I 2 = 97.66%; Cochrane’s Q statistic, p < 10−2; Egger’s test, p = 0.444; Begg’s test, p = 0.615; see Table 3).

Forest plot for the pooled prevalence of metabolic syndrome.
Results of a Meta-Analysis of the Prevalence of Metabolic Syndrome in Different Subgroups of the Moroccan Population Based on Different Criteria Such as Geographical Areas, Health Status, Year of Publication, Mean Age, and Diagnostic Criteria for Metabolic Syndrome, Using Random Effect Model
A total of 28 studies reported the prevalence of MetS in women, with a weighted prevalence of 39.66% (Table 3). There was considerable heterogeneity in the prevalence of MetS in women (I 2 = 98.44%; Cochrane’s Q statistic, p < 10−2; Egger’s test, p = 0.833). In contrast, 12 studies reported the prevalence of MetS in men, with a weighted prevalence of 30.51%. Heterogeneity was also observed in the prevalence of MetS in men (I 2 = 82.50%; Cochrane’s Q statistic, p < 10−2; Egger’s test, p = 0.827). These data suggest that MetS is more prevalent in women than in men. However, there is considerable variability in the results between studies, particularly among women. None of the analyses showed significant evidence of publication bias.
Prevalence of MetS according to diagnostic criteria and sex of study participants
This systematic review and meta-analysis of the Moroccan population showed that the prevalence of MetS varies depending on diagnostic criteria and subgroups. Most subgroups exhibited significant heterogeneity between studies, with some demonstrating a significant publication bias (Table 3).
According to studies using the NCEP-ATP III, 2001 thresholds, the weighted prevalence of MetS was 36.17%, independent of sex and age, with significant heterogeneity (I 2 = 97.69%; Cochrane’s Q statistic p < 10−3). The weighted prevalence of MetS in women was 34.57% with a high degree of heterogeneity, while in men, it was 22.44%, with a moderate degree of heterogeneity.
The prevalence of MetS according to the revised NCEP-ATP III, 2005 criteria was 33.42% (95% CI: 22.22% to 45.66%). The prevalence among women was higher (44.27%) than among men (34.27%), with significant heterogeneity.
According to the IDF 2005 criteria, the overall prevalence of MetS was 36.18%. However, women had the highest prevalence at 42.2%, while men had the lowest at 35%, with significant heterogeneity.
The results of studies utilizing the JIS 6 thresholds indicate an overall prevalence of 41.95%. The weighted prevalence for women was 44.43%, while for men it was 25.42%. Notably, considerable heterogeneity was observed between sexes.
Based on the diagnostic criteria and sex, the results showed a variable prevalence of MetS. Additionally, there was significant heterogeneity between studies, indicating variations in the results across different populations and study methodologies.
The pooled prevalence of MetS across the different geographical regions of Morocco
The studies reviewed showed a significant variation in the pooled prevalence of MetS among the geographical regions of Morocco. The lowest pooled prevalence rate was observed in the southern zone of Morocco at 18.93%, whereas the highest rate was found in the central zone of Morocco at 46.52% (Fig. 3).
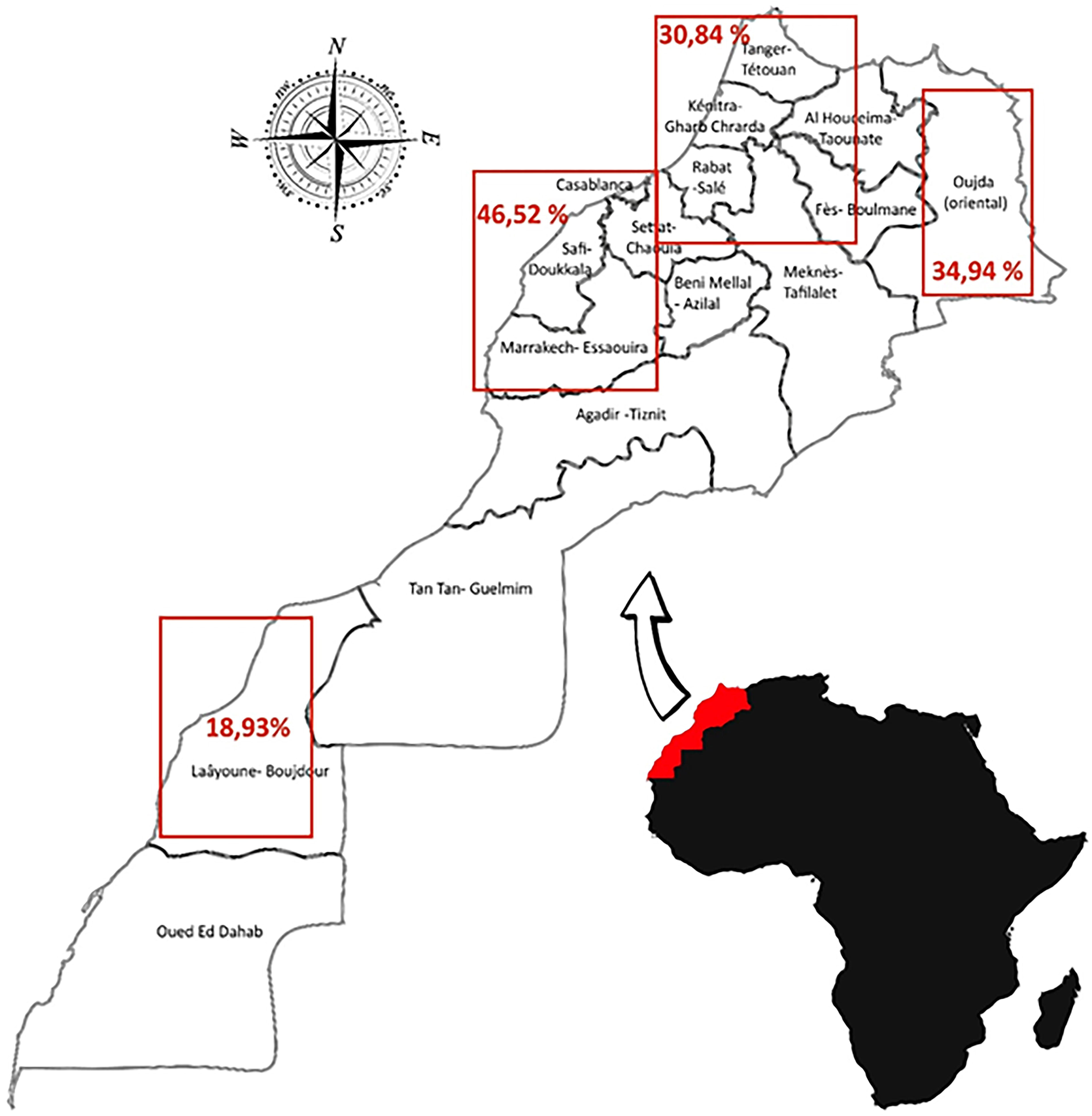
Map of Morocco indicating the prevalence of metabolic syndrome in different regions.
The study results reveal significant heterogeneity among the Northern, Central, and Southern zones, as evidenced by high I 2 values and significant p-values for heterogeneity. However, the evidence of publication bias in any of these zones was not strong, as the p-values of Egger’s and Begg’s tests were not significant (Table 3). As for the Eastern zone, only one study is listed, so no statistical comparison or measure of heterogeneity is provided. Nevertheless, its prevalence is 34.94% (95% CI: 31.19% to 38.82%).
Pooled prevalence of MetS based on year of publication
Stratified analysis by year of study showed a noticeable increase in the prevalence of MetS over time. The pooled prevalence of MetS increased significantly from 28.49% (2000–2014) to 46.88% (2000–2024). Both periods showed very high heterogeneity (I 2 > 96%), reflecting significant variability across studies (Table 3). The Cochrane’s Q test showed a p-value of less than 10−3 for both groups, indicating that there were statistically significant differences between the studies in each group. Egger’s and Begg’s tests showed no significant evidence of publication bias in either group, suggesting that the results of the included trials were not strongly influenced by publication bias.
Pooled prevalence of MetS by age
Analysis of the results showed that the prevalence of MetS varied by age group. The highest prevalence of 43.23% was found in the 50 and over age group, followed by the 40–49 age group 25.52%, and the 30–39 age group 25.44% (Table 3). There was significant heterogeneity across the three age groups, with an I 2 of over 95% and Cochrane’s Q statistic p of less than 10−3, indicating major differences between the studies for each age group. There was no significant evidence of publication bias in any of the age groups using Egger’s test and Begg’s test. This suggests that the results of the included studies were not greatly affected by publication bias.
The pooled prevalence of MetS by the state of health
The prevalence of MetS among apparently healthy individuals was analyzed in 20 studies involving 9232 participants. The results showed a 29.41% prevalence of MetS, with a 95% CI ranging from 23.29% to 35.92% (Table 3). Cochrane’s Q test revealed significant heterogeneity (p < 10−3), with a high I 2 (97.51%), suggesting a high degree of variability between studies. However, the publication bias was insignificant in the Egger’s or Begg’s tests.
Six studies were analyzed, involving 1859 people with general obesity. The prevalence of MetS was 58.81%. Cochrane’s Q test revealed substantial heterogeneity (p < 10−3), with an I 2 of 85.19%, indicating considerable inconsistency between the studies. Using Egger’s and Begg’s tests, insignificant publication bias was found.
Three studies involving 323 patients with type 2 diabetes showed a MetS prevalence of 61.84% (Table 3). Cochrane’s Q test indicated significant heterogeneity (p < 10−3) with a high I 2 value (94.44%), suggesting considerable variability between studies. Egger’s and Begg’s tests showed insignificant published bias. The prevalence of MetS in two studies of 344 people with hypertension was 47.09% (Table 3). Cochrane’s Q test indicated significant heterogeneity (p < 10−3), with a high I 2 value (98.94%), suggesting substantial inconsistency between studies. Egger’s test demonstrated significant publication bias (p < 10−3), whereas Begg’s test did not. Concerning rheumatoid arthritis, three studies involving 429 individuals reported a MetS prevalence of 28.29% (Table 3). Cochrane’s Q test indicated significant heterogeneity (p < 10−3) among the studies (I 2 = 85.89%). Egger and Begg’s tests did not reveal any significant publication bias.
The study results demonstrated a high prevalence of MetS in various populations, with significant heterogeneity among studies.
Publication bias
The results in Figure 4 illustrate a symmetrical funnel plot, while Egger’s and Begg’s tests showed no evidence of publication. The results of the analyses were insignificant with no evidence of significant publication bias in the dataset (Table 3).
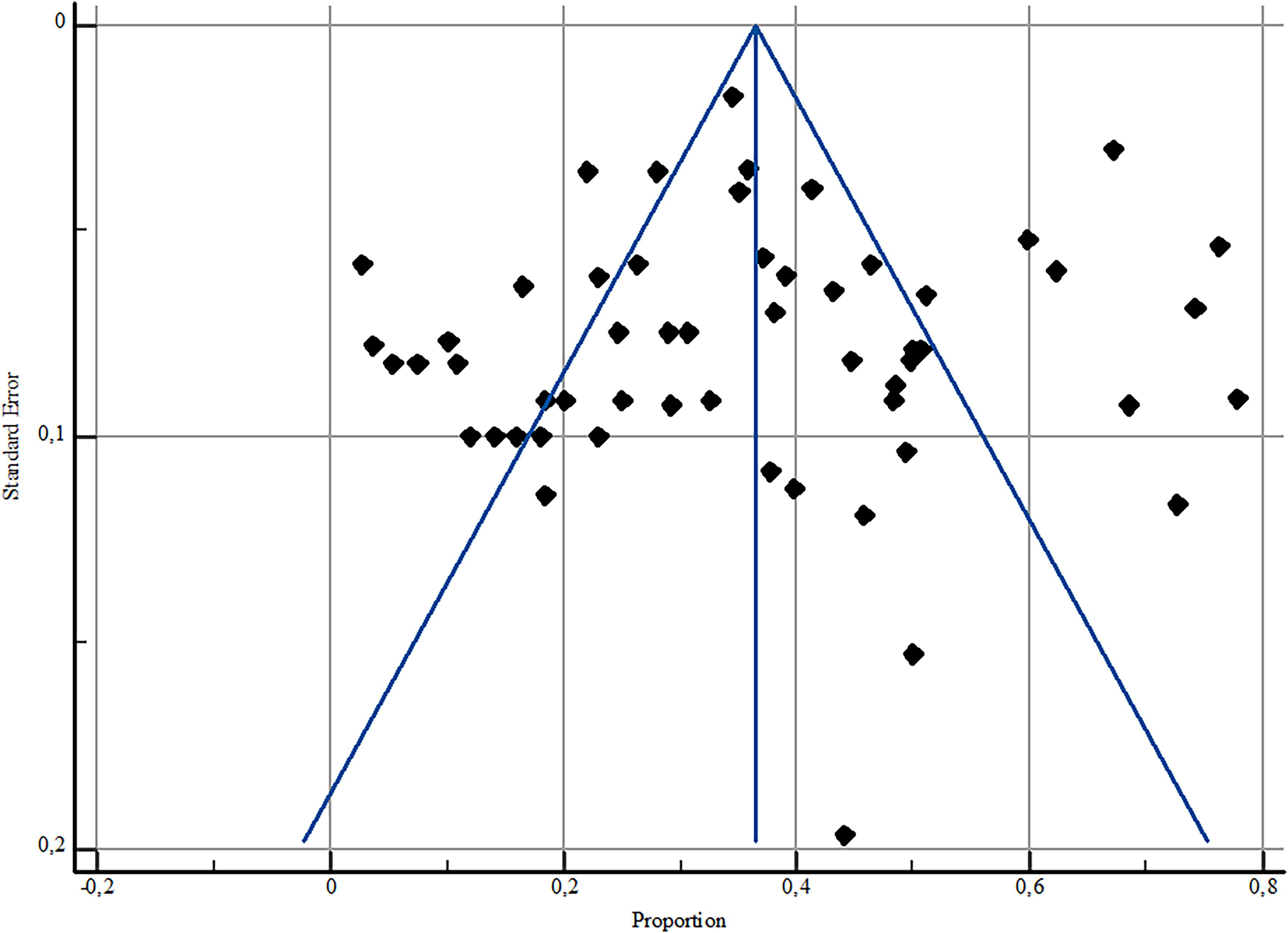
Funnel Plot for the pooled prevalence of metabolic syndrome and standard Error.
Discussion
The objective of this study was to provide an estimation of the pooled prevalence of MetS in Morocco. Studies published between 2000 and March 2024 were analyzed. A total of 32 studies with a total of 13,889 individuals analyzed were included in the final analysis of this systematic review. We used the NCEP ATP III (2005), NCEP ATP III (2001), IDF (2005), and JIS (2009) definitions in our meta-analysis. The overall prevalence, according to this meta-analysis, was 34.68%, which is comparable to the results of other studies conducted worldwide. Another meta-analysis of 28 million people worldwide found that the pooled prevalence of MetS in adults aged ≥18 years ranged from 12.5% to 31.4%. 9 For comparison, these are in North Africa (32.4%), Nigeria (31.7%), 65 Tunisia (23.0% to 36.5%), 66,67 the United States (34.7%), 68 among adults in Brazil (33%), 69 and in the Arab Emirates (33.6%). 70 Comparative data is slightly higher in European countries (from 22.1% to 31.5%), 9 and Iran (30.4%) according to Kalan Farmanfarma, and all 71 and 28% according to Mokhayeri and all. 72 However, studies have shown that the prevalence is higher in some countries than in Morocco. According to Al-Rubeaan K and al., 73 the prevalence is higher in Algeria (43.9%), Sudan (39.8%), Ghana (39.7%), and Libya (>45%) 67 at 42.6%. 74 This finding suggests that MetS is a global problem that requires special attention.
However, it is important to note that the pooled prevalence of MetS may vary among countries owing to differences in lifestyle, diet, genetic factors, and diagnostic standards. Therefore, further research is needed to better understand the pooled prevalence and risk factors associated with MetS. The Pooled prevalence of MetS was higher in women than in men, with global prevalences of 39.66% and 30.51%, respectively. Several systematic reviews and meta-analyses have shown that women are more likely to have MetS than men. 9,67,71,72,75 –77 Other observational studies of different populations have shown, for example, that men are more likely to have MetS than women. Saoudi-Arabia has recorded rates ranging from 31.6% to 39.8%, mainly in men, ranging from 34.4% to 45%, compared to women, with rates ranging from 35.4% to 29.2%. 73 Other observational studies have shown that the prevalence of MetS in men does not differ from that in women, as evidenced by a Tunisian study that found the prevalence to be almost the same in both sexes, at 36.8% and 36.2%, respectively. 66 Another study conducted in China showed that the prevalence of MetS in men (27.9%) was not statistically different from that in women (26.8%). 78 In addition, in 2023, the inactivity rate for Moroccan women was 73%, which is significantly higher than the rate for men, at 7.5%. 79 The higher prevalence of MetS in women in our study can be attributed to abdominal obesity, which is mainly caused by a lack of physical activity, 80 time spent in bed, 81 and hormonal and metabolic changes associated with menopause. 38,82,83 Therefore, women need to be particularly aware of their health and develop healthy lifestyle habits to reduce the risk of developing MetS. The geographical distribution of MetS varied according to geographical zone, with the highest pooled prevalence of 30.84% in the northern region of Morocco. The 30.84% is similar to that found in Europe. 9 The zone with the lowest prevalence, 18.3%, is in the south, whereas the zone with the highest prevalence, 46.52% (36.57 to 56.61), is in the center and is characterized by high industrial activity. Genetic and epigenetic factors 84 –86 linguistic, cultural, economic, socioeconomic, demographic, or related to nutritional circumstances, lifestyle, and dietary practices unique to each region may be the main causes of variation in the pooled prevalence of MetS among Moroccan regions. 87 It would be useful to compare the dietary practices of these regions and investigate the genetic risks associated with MetS.
In the current meta-analysis, the pooled prevalence of MetS changed unevenly over the study period (2000–2024). Between 2000 and 2014, the prevalence was 28.49% (confidence interval 95%: 23.37–33.91%). Between 2015 and March 2024, the pooled prevalence increased significantly to 46.88% (37.58%–56.29%). Several studies indicate an increasing trend in MetS prevalence over time. For instance, in the Chinese elderly population, the prevalence increased from 50.4% in 2001 to 58.1% in 2010. 88 Similarly, a systematic review and meta-analysis of the global prevalence of MetS in patients with type 1 diabetes found that the prevalence of MetS was higher between October 2020 and October 2015 (26.6%) than between 2005 and 2014 (21.8%). 89 Contrarily, some studies suggest a declining or steady trend. A systematic review covering 2005 to 2015 found that the trend of MetS prevalence was declining, although it remained steady in the last decade. 72
In recent decades, the nutritional situation in Morocco has undergone significant changes due to demographic, social, economic, and dietary changes that have affected the country, leading to quantitative and qualitative changes. 90 A higher prevalence of NCDs, such as obesity and MetS, is associated with high consumption of ultra-transformed foods. 91 According to, 17 the nutritional and epidemiological transition in Morocco may explain the significant increase in the prevalence of MetS, which manifests as a shift in the global burden of morbidity and mortality from infectious diseases to non-transmissible diseases and trauma. Based on age-stratified analyses, the estimated pooled prevalence of MetS varies significantly with age, increasing by approximately 70% in older individuals compared with those with an average age of 50 years or older. The conclusions of this study are consistent with data reported in various meta-analyses of different populations, including Ethiopia, 92 Africa, 67 the United Arab Emirates, 70 Saudi Arabia, 73 and Malaysia. 93 The relationship between aging and MetS is complex and involves a variety of physiological changes, factors related to lifestyle choices, and the accumulation of risk factors over time, such as changes in body composition, 94 decline in physical activity, and changes in age-related metabolic changes. 95 According to our results, MetS was present in 58.81% of Moroccans with obesity. We compared our results with those of meta-analyses conducted in several African countries. These data are similar to those observed in the meta-analysis in 29 African countries, with a prevalence of 31.5%, 67 and lower than those observed in observational studies conducted in Arab countries, such as Jordan, 96 Saudi Arabia, 97 and Libya. 98 These studies reported prevalence rates of 84.2% in Jordan, 80% and 85.8% in Saudi Arabia, and 80.8%–92% in Libya. According to our results, MetS was observed in 61.84% of individuals with type 2 diabetes in Morocco. Our results were compared to those of other meta-analyses conducted in Africa. This prevalence is similar to that observed in sub-Saharan Africa, 99 where it is estimated to be 60.8%. However, it is lower than that observed in a meta-analysis of 29 African countries, with a prevalence of 66.9%, 67 and that observed in observational studies conducted in Arab countries such as Jordan, 96 Saudi Arabia, 97 and Libya. 85 These studies estimated the prevalence to be 84.2% in Jordan, 80% and 85.8% in Saudi Arabia, and 80.8%–92% in Libya. In our meta-analysis, the weighted prevalence of MetS in hypertensive patients was 47.09%. This prevalence is relatively high compared with the data found in the literature on MetS in hypertensive patients in Africa (43.8%). 67 Hypertensive patients are particularly affected by this syndrome because arterial hypertension is one of the diagnostic criteria. The association between hypertension and MetS is clinically important because of its significant impact on individual health.
Strengths and limitations of the study
The main strengths of the studies examined in this review are the use of an appropriate cross-sectional model to estimate prevalence, the collection of prospective data to ensure the chronology of exposure and outcomes, and the inclusion of diverse populations with different health problems and demographic characteristics. However, it is important to highlight the limitations of these previous studies. First, we restricted the search to English-language publications, potentially missing relevant studies in other languages. Second, the risk of selection bias associated with consecutive sampling should be considered. In addition, the majority of studies on MetS have been conducted in hospital settings, which may limit the extrapolation of the results to the general population. Furthermore, the variability in the diagnostic criteria for MetS may influence the prevalence observed in each study and make direct comparisons between studies difficult. Furthermore, the risk of bias varies between studies from low to moderate or even high, which may affect the prevalence measured and the validity of the conclusions. Finally, some studies have focused on specific populations, such as healthy relatives or postmenopausal women, while others have examined patients with obesity or diseases such as type 2 diabetes and high blood pressure. This may explain the variability in the observed prevalence rates.
Conclusions
To the best of our knowledge, this paper is the first attempt to estimate the overall prevalence of MetS in Morocco. The findings indicate that the prevalence of MetS in the Moroccan population is similar to the global prevalence, suggesting that Morocco follows a global trend. The prevalence of MetS has increased over time and is influenced by age, with a higher prevalence in people aged 50 years or older than in younger age groups. The prevalence of MetS was slightly higher among women, and regional disparities were observed. The central zone has a higher prevalence, while the northern region has a lower prevalence, and the southern region has the lowest. Patients with type 2 diabetes, obesity, and hypertension have the highest risk of developing MetS.
These variations are influenced by factors such as diagnostic criteria, demographic differences, age, sex, eating habits, and level of physical activity. It is crucial to consider these results when developing prevention and treatment strategies tailored to the specific needs of Moroccan populations. For instance, public health interventions could include targeted awareness campaigns addressing risk factors such as sedentary lifestyles, unhealthy diets, and obesity, particularly in regions with higher prevalence, such as the Central Zone. These efforts could help reduce the incidence of MetS. Community programs promoting physical activity and healthy eating habits, while considering cultural preferences and socio-economic barriers, could also play a crucial role. Early screening initiatives in primary care settings, especially for high-risk groups such as individuals with type 2 diabetes, obesity, or hypertension, would facilitate timely diagnosis and management of MetS. Clinically, health care providers could leverage these findings to refine the identification and management of MetS. For instance, adopting region-specific diagnostic protocols that reflect demographic variations could improve accuracy. Personalized treatment plans combining lifestyle modifications (e.g., diet and exercise) with pharmacological approaches for high-risk patients present a promising strategy for future implementation.
Further research is warranted to expand the understanding of MetS in Morocco. Longitudinal studies could track temporal shifts in prevalence and identify evolving risk factors, while regional studies might investigate underlying causes of disparities, such as differences in health care access, dietary patterns, and physical activity. Intervention studies could assess the efficacy of public health programs targeting high-risk populations. Finally, genetic research may elucidate hereditary factors contributing to MetS, offering new avenues for prevention and therapy.
Footnotes
Authors’ Contributions
H.N., B.R., A.B., and S.C. contributed to the design and implementation of the research. H.N. and S.C. participated in the analysis of the results and the writing of the article. B.R. and S.C. developed the original concept and supervised the project. All authors read and approved the final article.
Ethical Approval
In general, ethical approval is not required for our study, as it does not involve confidential participant data or intervention. We collected and synthesized data from previous studies; therefore, ethical considerations were not applicable.
Author Disclosure Statement
The authors disclose no conflicts of interest.
Funding Information
This work has not received any funding from any public, private, commercial, or non-profit organization.