
Abstract
Purpose:
We conducted an observational study on how profound hypothyroidism affects circulating citrate, a potential biomarker of mitochondrial dysfunction linked to mortality.
Methods:
Sixteen differentiated thyroid carcinoma patients were first studied during hypothyroidism, i.e., 4–6 weeks after total thyroidectomy, and subsequently after 20 weeks of thyroid hormone supplementation. 5 patients were also studied during euthyroidism, i.e., before total thyroidectomy. Circulating citrate and total ketone bodies were measured by nuclear magnetic resonance spectroscopy.
Results:
During profound hypothyroidism (mean thyroid stimulating hormone [TSH] 106 ± 77 mU/L), circulating citrate was 72% higher (95% CI: 48%–96%), reaching 157 ± 48 µmol/L, compared to 93 ± 25 µmol/L during thyroid hormone administration (mean TSH 0.20 ± 0.53 mU/L). This increase remained significant after adjusting for estimated glomerular filtration rate (eGFR) (P < 0.001) and body mass index (BMI) (P < 0.001). Citrate during hypothyroidism was also higher compared to five euthyroid patients studied before total thyroidectomy (P = 0.014). Total ketone bodies did not significantly change during hypothyroidism (P = 0.62).
Conclusion:
Short-term profound hypothyroidism gives rise to a major increase in circulating citrate, also when adjusted for changes in eGFR and BMI, conceivably attributable to hypothyroidism-related mitochondrial dysfunction. It is suggested that thyroid function status should be taken into consideration when evaluating the association of circulating citrate with adverse health outcomes.
Introduction
Hypothyroidism is a highly prevalent condition, particularly in women and in the elderly. 1 Long-term hypothyroidism may be implicated in many health issues, including dyslipidemia, atherosclerotic cardiovascular disease, heart failure, stroke, renal function impairment, insulin resistance, metabolic dysfunction-associated steatotic liver disease, and possibly also deterioration in glucose tolerance. 2 –4
Thyroid hormones, especially triiodothyronine, are well known to affect energy expenditure via effects on mitochondrial function and substrate cycling, 5,6 and hypothyroidism has been linked to mitochondrial dysfunction. 7 Citrate is a pivotal metabolite of the tricarboxylic acid cycle (also known as the Krebs or citric acid cycle), an essential pathway for energy production through mitochondrial oxidation of acetyl-CoA. 8 Using nuclear magnetic resonance (NMR) spectroscopy, emerging evidence suggests that plasma citrate, which conceivably represents a proxy of mitochondrial dysfunction, is associated with all-cause and cardiovascular mortality. 9 –11
Total thyroidectomy creates a unique state of profound hypothyroidism, offering insight into its effects on circulating biomarkers. 12 Given the lack of prior data, this study aimed to investigate the short-term impact of post-thyroidectomy hypothyroidism on NMR-determined circulating citrate.
Materials and Methods
Participants and study design
The current observational study was performed among patients with newly diagnosed non-metastasized differentiated thyroid carcinoma (DTC), aged 18–75 years, as described in detail elsewhere. 12 The study was approved by the Medical Ethics Committee of the University Medical Center Groningen (registration number 2015/116; Netherlands Trial Register [NTR ID 7228]). All participants provided written informed consent, and inclusion was between November 2016 and April 2019.
A total of 16 DTC patients were included. The study comprised two outpatient study visits for all participants, following Dutch guidelines of DTC treatment. 13 First, they were studied under circumstances of hypothyroidism, i.e., 4–6 weeks after total thyroidectomy on the day before ablative radioactive iodine treatment. This procedure was carried out with thyroid stimulating hormone (TSH) levels being considerably elevated to enhance uptake of radioactive iodine in any potentially remaining thyroid tissue. Shortly thereafter, liothyronine (n = 14; 75 µg daily, divided in 3 doses) or levothyroxine (n = 2; 175 or 200 µg daily) administration was started. Second, they were studied after 20 weeks of thyroid hormone administration. In 5 patients, we had the opportunity of an extra visit before the total thyroidectomy, i.e., during euthyroidism. Supervised by a dietician, study subjects were advised to keep their nutrient intake unchanged from 5 days onwards before each study visit. The presence of distant metastases, diagnosed by extrathyroidal radioactive iodine uptake, was an exclusion criterion.
Body mass index (BMI) was calculated as weight divided by length squared (kg/m2). Venous blood, drawn from an antecubital vein, was obtained after an overnight fast.
Laboratory methods
TSH (reference range 0.27 to 4.20 mU/L) and free thyroxine (reference range 12–22 pmol/L) were measured using the Roche Modular E170 Analyzer (Roche Diagnostics, Mannheim, Germany). Plasma glucose and serum creatinine were measured using routine procedures at the Department of Laboratory Medicine of the University Medical Center Groningen, The Netherlands. Estimated glomerular filtration rate (eGFR) was calculated using the creatinine-based Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation. 14
Ethylenediaminetetraacetic acid (EDTA)-anticoagulated plasma was prepared by centrifugation at 4°C and stored at −80°C until analysis. EDTA-plasma samples were shipped frozen to Labcorp, Morrisville, NC, USA, and then thawed, with the biomarkers of interest being subsequently measured using a Vantera® Clinical Analyzer (Labcorp, Morrisville, NC, USA), a fully automated, high-throughput, 400 MHz proton (1H) NMR spectroscopy platform. 15 Plasma citrate was determined using NMR spectroscopy as described. 16 The stability of citrate has been established in samples that were frozen for up to 12 years at temperatures below −70°C. Inter-assay precision for citrate, expressed as coefficients of variation, ranged from 5.2% for high-concentration samples to 9.6% for low-concentration samples. 16 Total ketone bodies were calculated as the sum of β-hydroxybutyrate, acetoacetate, and acetone, which were also measured in EDTA-plasma samples using the Vantera Clinical Analyzer, as detailed elsewhere. 17 For total ketone bodies, intra-assay and inter-assay precision were <5% and <9.4%, respectively.
Plasma total cholesterol and triglycerides were determined using the LP4 algorithm obtained from lipoprotein measured from the Vantera® Clinical Analyzer. 15
Statistical analysis
SPSS 28 (version 28.0, IBM Corp., Armonk, NY, USA) and R version 4.3.0 (Vienna, Austria) (http://cran.r-project.org/) were used for data analysis. Results are given in mean ± SD (range). Ketone bodies were Ln transformed for calculations. Changes are presented with 95% confidence intervals. Changes in variables between hypothyroidism and thyroid hormone supplementation were determined by paired t-tests. To confirm statistical validity, Wilcoxon signed-rank tests were additionally caried out, which confirmed that all significant results remained unchanged.
Pearson correlation coefficients were calculated by linear regression analysis with 95% confidence intervals. Two-sided P-values <0.05 were considered to be significant.
Results
We included 16 DTC patients (15 women, aged 46 ± 11 [range 29 to 66] years), of whom 13 had papillary thyroid carcinoma and 3 had follicular thyroid carcinoma. Concomitant drug use, i.e., oral contraceptives (n = 8) and prednisolone (5 mg daily, n = 1), was unchanged during the study. None of the participants were current smokers. Mean TSH was 106 ± 77 (range 59 to 371) mU/L during hypothyroidism and decreased to 0.20 ± 0.53 (range 0.01 to 2.15) mU/L during thyroid hormone administration (P < 0.001).
As shown in Table 1, BMI was higher during hypothyroidism, but blood pressure was unchanged. Serum creatinine was higher and eGFR was lower during hypothyroidism. Plasma total cholesterol and triglycerides were also considerably higher during hypothyroidism, whereas plasma glucose and total ketone bodies did not significantly change (Table 1).
Clinical and Laboratory Variables of 16 Patients during Hypothyroidism and after 20 Weeks of Thyroid Hormone Administration
Data in mean ± SD. Changes are expressed with 95% confidence intervals (CI) during hypothyroidism vs. thyroid hormone administration. Statistical comparisons were done by paired t-tests. Toal ketone bodies were ln transformed for calculations.
BMI, body mass index; CI, confidence interval; eGFR, estimated glomerular filtration rate.
Circulating citrate was 72% (95% CI, 48% to 96%) higher during hypothyroidism. Also, when expressed as the citrate/eGFR ratio or as the citrate/BMI ratio, thus accounting for changes in eGFR and BMI, citrate was similarly higher during hypothyroidism (Table 1 and Fig. 1). When comparing these values to those obtained before total thyroidectomy, i.e., during euthyroidism (n = 5), citrate, the citrate/eGFR ratio, and the citrate/BMI ratio were higher during hypothyroidism (161 ± 54 vs. 101 ± 29 µmol/L, P = 0.014; 2.9 ± 1.5 vs. 1.0 ± 1.0, P = 0.036, and 6.3 ± 2.4 vs. 4.0 ± 1.4, P = 0.017, respectively).
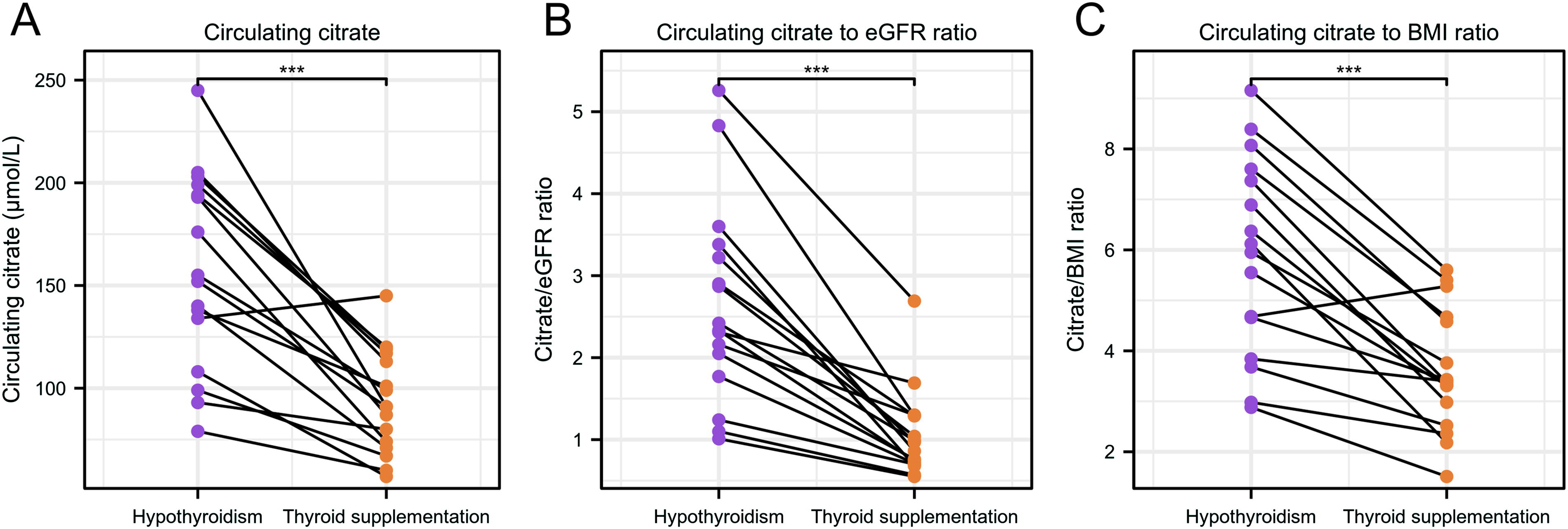
Circulating citrate concentration
Although statistical significance was not reached, citrate tended to be correlated with eGFR (r = −0.35 [95% CI, −0.72 to 0.17], P = 0.18) during hypothyroidism and during thyroid hormone administration (r = −0.41 (95% CI, −0.75 to 0.11), P = 0.12). The relationship of citrate with BMI was r = 0.09 (95% CI, −0.42 to 0.56), P = 0.73) during hypothyroidism and r = −0.22 (95% CI, −0.64 to 0.31), P = 0.41) during thyroid hormone administration. Citrate tended to be correlated with total ketone bodies during hypothyroidism (r = 0.46 (95% CI, −0.04 to 0.78), P = 0.07), but not during thyroid hormone administration (r = 0.06 (95% CI, −0.45 to 0.54), P = 0.83).
Discussion
The present study show to our knowledge for the first time, that circulating citrate, a conceivable biomarker of mitochondrial dysfunction, is considerably elevated during profound short-term hypothyroidism consequent to total thyroidectomy. Our findings may have clinical relevance since circulating citrate is increasingly recognized as a biomarker that is associated with all-cause mortality, as found in the general population, type 2 diabetes, and end-stage liver disease. 9 –11 Moreover, plasma citrate is part of a multimarker algorithm, which predicts all-cause and cardiovascular mortality, in subjects with multiple co-morbidities, including high risk of cardiovascular disease. 18
The currently documented NMR-measured plasma citrate concentration, averaging 157 µmol/L during hypothyroidism, is indeed higher than the mean value of 106 µmol/L as reported among community-dwelling subjects. 11 Additionally, in type 2 diabetic subjects who died during follow-up, mean citrate was 138 µmol/L vs. 120 µmol/L who remained alive. 10 Participants from these studies were also recruited from the north of the Netherlands, and plasma citrate was measured using the same NMR technique and deconvolution procedure. 10,11 Urinary citrate excretion may be coupled to chronic kidney disease progression. 19 Moreover, plasma citrate was inversely associated with eGFR in end-stage liver disease, 11 with a trend for such a relationship in the current report. We also evaluated whether the increase in circulating citrate during hypothyroidism persisted even after adjusting for expected changes in eGFR and BMI. Citrate was similarly higher during hypothyroidism when expressed as the citrate/eGFR ratio and the citrate/BMI ratio. Combined, these findings strengthen our conclusion that thyroid hormone status affects circulating citrate.
Thyroid function is in a complex manner involved in ketogenesis. TSH and triiodothyronine have opposing effects on substrate availability for ketone body production. 5,20 Plasma total ketone bodies were unaffected during hypothyroidism. Nonetheless, ketone bodies tended to be positively correlated with citrate, but only during hypothyroidism. Like citrate, ketone body levels could be regarded as a proxy of mitochondrial dysfunction. We hypothesize that their relationship during hypothyroidism might reflect abnormalities in mitochondrial function. 6,7
Our study has strengths and limitations. Data collection was carried out following the sequence of interventions as indicated by Dutch treatment guidelines for DTC. 13 Hence, potential effects of more prolonged thyroid hormone withdrawal could not be assessed. In addition, TSH levels were on average below the reference range, though not fully suppressed during thyroid hormone supplementation, indicating mild oversupplementation. To some extent, this could have overestimated the observed effects on citrate. However, in a small subset of patients who were also studied before thyroidectomy, i.e., in the euthyroid state, changes in citrate compared to those during hypothyroidism were of similar magnitude.
In conclusion, short-term profound hypothyroidism gives rise to a major increase in circulating citrate, which may be attributable to hypothyroidism-related mitochondrial dysfunction. We suggest that thyroid function status should be taken into consideration when evaluating the association of circulating citrate with adverse health outcomes.
Footnotes
Acknowledgments
Plasma citrate, ketone bodies, and lipids were measured at Labcorp, Morrisville, NC, USA, at no cost.
Authors’ Contributions
T.P.L. and R.P.F.D.: Developed and formulated the research questions, have full access to the study data and take responsibility for its integrity and the data analysis. Y.L. and R.P.F.D.: Wrote the article. Y.L., M.H.L., A.P., M.A.C., T.P.L., and R.P.F.D.: Contributed to the acquisition of data, contributed to discussion, draft revision and edited the article. All authors approved the final version of the article.
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Medical Ethics Committee of the University Medical Center Groningen (registration number 2015/116).
Consent to Participate
Written informed consent was obtained from the parents.
Author Disclosure Statement
M.A.C. is an employee of Labcorp and owns stock in Labcorp. The other authors declare that they have no conflicts of interest.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.