
Abstract
In this study, we explored the effect of moderate hypothermia on brain tissue oxygenation following acute intracranial hypertension in micropigs. Twenty healthy juvenile micropigs weighting 4–6 kg were randomized into two groups: a normothermia group (n = 10) and a moderate hypothermia group (n = 10). The animals were intravenously anesthetized with propofol (4 mg/kg), an endotracheal tube was inserted, and mechanical ventilation was begun. Autologous arterial blood was injected into the left frontal lobe to establish acute intracerebral hematoma and intracranial hypertension (intracranial pressure [ICP] >40 mm Hg) in all animals. Cooling was initiated at 30 min after injection of the blood, and was achieved via the use of an ice bath and ice packs. In the hypothermia group, the brain temperature decreased to 33–34°C. Brain temperature was maintained at 37 ± 0.3°C in the normothermia group. The ICP, cerebral perfusion pressure (CPP), brain tissue oxygen pressure (PbrO2), brain tissue carbon dioxide pressure (PbrCO2), and brain tissue pH value (pHbr) were continuously monitored for 3 h in all animals. Compared to normothermia group, ICP values significantly decreased and CPP markedly improved in the hypothermia group (p < 0.05). Further, pHbr also markedly increased and PbrCO2 decreased significantly in the hypothermia group (p < 0.05). However, PbrO2 did not statistically significantly improve in the hypothermia group (p > 0.05). In sum, moderate hypothermia significantly decreased ICP, reduced PbrCO2, and increased pHbr values, but did not improve cerebral oxygenation following acute intracranial hypertension.
Introduction
S
Previous laboratory studies have demonstrated that mild to moderate hypothermia significantly reduces mortality and morbidity in traumatically brain-injured rats (Clifton et al., 1991; Jiang et al., 1991). Recent clinical trials have also shown that moderate hypothermia significantly improves the outcome of patients with cerebral ischemia due to cardiac arrest (Bernard et al., 2002; The Hypothermia after cardiac arrest study group, 2002). It is believed that the beneficial effects of mild to moderate hypothermia occur due to metabolic and biochemical processes. These mechanisms include temperature-dependent reductions of cerebral metabolic rate of oxygen consumption (CMRO2), decreases in free radical production (Hagerdal, 1979; Vink et al., 1987), attenuation of disruption of the blood–brain barrier (Jiang et al., 1992; Smith and Hall, 1996) and brain edema (Shiozaki et al., 1993), attenuation of ionic disruption (Welsh et al., 1990), decreased excitatory amino acid release (Busto et al., 1989; Mitani and Kataoka, 1991), reduced cerebral lactate accumulation (Jiang et al., 2004), increased fractional glucose metabolism shunting (Kaibara et al, 1999), and inhibition of excessive neuronal calcium uptake and intracellular calcium overloading (Mitani et al., 1991).
The measurement of brain tissue oxygen pressure (PbrO2), brain tissue carbon dioxide pressure (PbrCO2), and brain tissue pH value (pHbr) may also provide additional insight into the influence of CMRO2 on the cellular oxygen supply after TBI or intracranial hypertension (Meixensberger et al., 2003). With the development of continuous monitoring techniques of PbrO2, PbrCO2, and pHbr, we are better positioned to explore the status of brain tissue oxygenation following brain injury, and to demonstrate the effect of hypothermia on PbrO2 following traumatic or ischemic brain injury or acute intracranial hypertension.
Burger and associates demonstrated that intra-ischemic hypothermia significantly improves PbrO2, while reducing the associated ischemic tissue damage and hippocampal neuronal cell injury in an extra-axial mass lesion model (Burger et al., 2004). However, there have been no reports of hypothermia's effect on PbrO2, PbrCO2, and pHbr values following acute intracranial hypertension in an intracranial hematoma model. The aim of this study was to assess the effects of moderate hypothermia on PbrO2, PbrCO2, pHbr, ICP, and CPP values following acute intracranial hypertension in an intracranial hematoma model in pigs.
Methods
Animal preparation
After approval by the Institutional Animal Care and Use Committee of the Animal Institute, Chinese Academy of Science, 20 healthy micropigs 2 months of age and weighing 4.5–5.5 kg received humane care in compliance with the principles of laboratory animal care formulated by the National Committee of Medical Research, and the “Guidelines for the Use of Laboratory Animals” issued by the Institute of Laboratory Animal Resources of China.
The micropigs were randomized into two groups: a normothermia group (n = 10), and a moderate hypothermia group (n = 10). The animals were initially anesthetized by an IM injection of ketamine hydrochloride (10 mg/kg), followed by propofol (4 mg/kg) administered IV and continuously maintained for 3 h. A tracheotomy was performed and an endotracheal tube was inserted. The animals were then mechanically ventilated. Both the femoral artery and vein on the right side were cannulated with polyethylene tubing for monitoring arterial blood pressure and to facilitate blood gas analysis.
Acute intracerebral hematoma model
After surgical exposure of the skull, a cranial burr hole (5 mm) was drilled 5 mm anterior to the coronal suture and 15 mm to the left of the sagittal suture. The dura mater was opened and a polyethylene catheter was inserted into the left frontal lobe to a depth of about 10 mm. The burr hole was then sealed with dental cement. Fresh autologous blood was drawn from the femoral artery catheter with a 10-mL syringe, and it was immediately placed in a microinjection pump. Approximately 5 mL of non-heparinized fresh blood was infused into the cranium at a rate of 0.5 mL/min to increase the ICP (>40 mm Hg).
Intracranial pressure monitoring
A cranial burr hole (5 mm) was drilled 5 mm posterior to the coronal suture and 10 mm to the right of the sagittal suture, and a transcranial bolt was placed. The dura mater was opened and a calibrated intracranial pressure probe with pressure sensor (Camino Laboratories, San Diego, CA) was placed in the frontal lobe. The burr hole was then sealed and ICP was continuously monitored for 3 h.
Brain tissue oxygen, carbon dioxide, and pH monitoring
A cranial burr hole was drilled 5 mm posterior to the coronal suture and 15 mm to the right of the sagittal suture. The dura mater and arachnoid membrane were opened. Then a Neurotrend multiparameter monitoring sensor was inserted into the frontal lobe (Neurotrend, Diametric Corp., United Kingdom), and the sensor was connected to a Neurotrend multiparameter monitoring system. Prior to the insertion of the catheter, the sensor was calibrated using sterile precision gases bubbling in a digitally controlled fashion through the calibration chamber. All values measured by the sensor were displayed on a monitor and stored in the on-board computer of the device.
Temperature measurement and manipulation
Frontal cortex brain temperature was monitored with a digital electronic thermometer (model DP 80; Omega Engineering, Inc., Stamford, CT) with a temperature probe 0.15 mm in diameter (model HYP-033-1-T-G-60-SMP-M; Omega Engineering) inserted 6 mm ventral to the surface of the skull. Rectal temperature was measured with an analog electronic thermometer (model 43 TE; YSI Telethermometer, San Jose, CA) and a temperature probe (YSI series 400). Cooling was initiated 30 min after injection of the blood into the cranium, and was achieved via the use of an ice bath and ice packs as previously described (Jiang et al., 1991). Approximately 15 min were required to reach the target brain temperature (33–34°C), which was maintained for 3 h under general anesthesia on room air by intermittent application of ice packs as needed. A brain temperature of 37 ± 0.3°C was achieved under general anesthesia with a heating blanket in the normothermia group.
All animals were sacrificed at 6 h after the injection of blood into the cranium. The brain was removed, fixed in 10% formaldehyde, and examined with light microscopy with hematoxylin and eosin stain.
Statistical analysis
Physiological data including ICP, CPP, PbrO2, PbrCO2, and pHbr were analyzed using a repeated-measures analysis of variance (ANOVA) for differences between time points and groups, followed by Fisher's post-hoc test. Statistical significance was set at p < 0.05. Data are expressed as absolute values (means ± SD).
Results
Effects of acute intracranial hypertension on physiological parameters and cerebral oxygenation
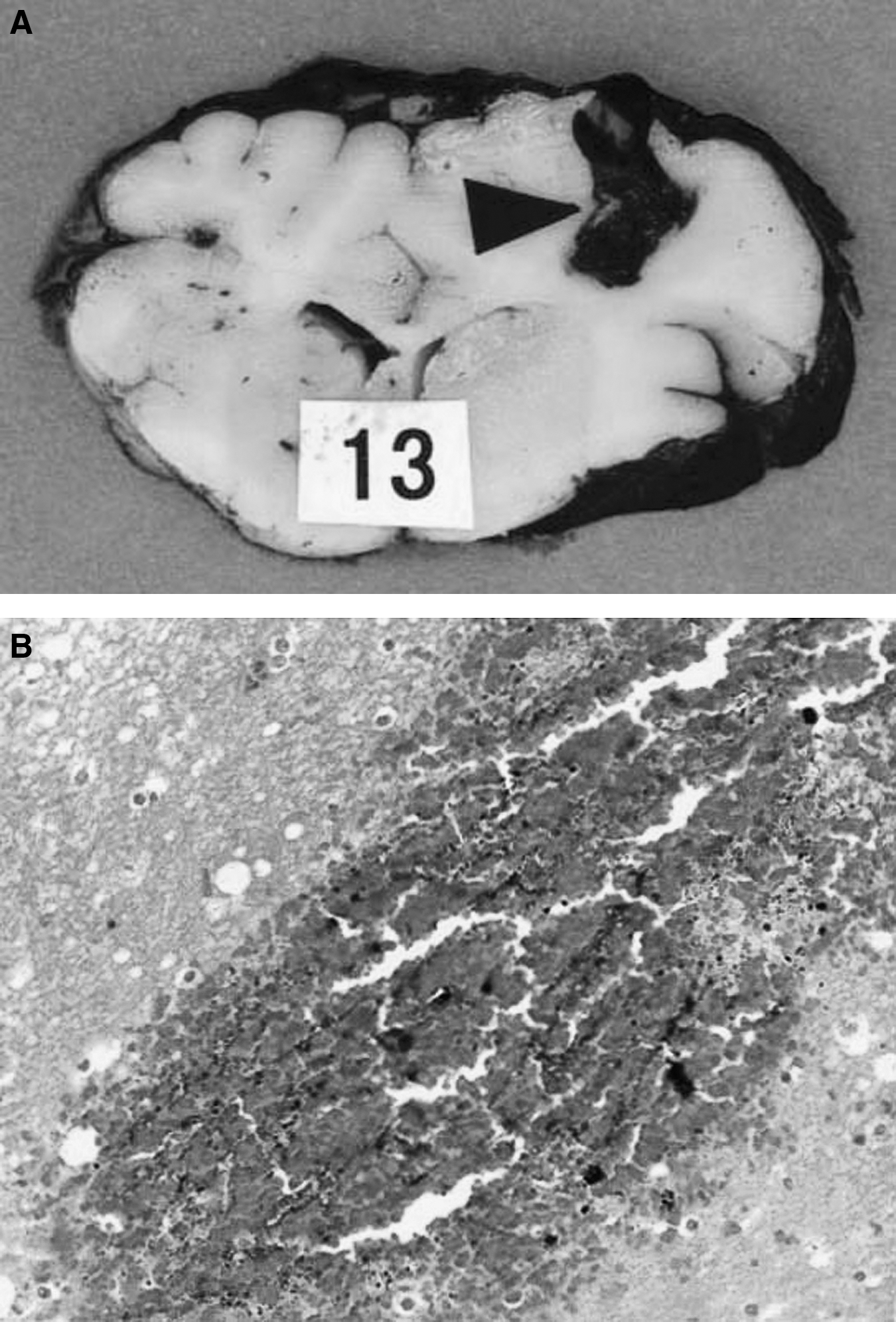
The acute intracranial hematoma model generated consistent results (Fig. 1A and B). None of the monitored parameters were significantly different between the two study groups prior to cooling (Table 1). ICP was significantly elevated and CPP was decreased following acute intracranial hypertension. PbrO2 and pHbr values were significantly decreased, and the PbrCO2 value was markedly elevated during acute intracranial hypertension (p < 0.01) (Fig. 2).
(

Changes in the monitored parameters after blood injection in the two study groups. After injection of blood into the cranium, intracranial pressure (ICP) was significantly elevated, cerebral perfusion pressure (CPP) was decreased, and brain tissue oxygen pressure (PbrO2) and brain tissue pH value (pHbr) were significantly decreased, and brain tissue carbon dioxide pressure (PbrCO2) was markedly elevated (p < 0.01). The ICP, PbrO2, PbrCO2, and pHbr values were no different between two groups before cooling. After cooling to 33–34°C, the ICP decreased, the CPP significantly improved, the PbrCO2 decreased, and the pHbr increased in the hypothermia group compared to the normothermia group (p < 0.05). However, the PbrO2 value in the hypothermia group was not statistically significantly different from the normothermia group (p > 0.05; *statistically significant).
CPP, cerebral perfusion pressure; ICP, intracranial pressure; MBP, mean blood pressure; Pa
Histological findings
Macroscopic slice preparation verified that hematoma was localized in the left frontal lobe. Light microscopic examination showed massive hemorrhage and neuronal cell loss in the brain tissue in and around the hematoma. The probe, however, did no harm to the brain tissue (Fig. 1A and 1B).
Effects of moderate hypothermia on ICP, CPP, PbrO2, PbrCO2, and pHbr values
In the hypothermia group, the ICP decreased from 40.1 ± 6.6 mm Hg to 28.6 ± 4.8 mm Hg at 3 h after cooling. In contrast, in the normothermia group, the ICP values ranged from 40.9 ± 7.1 mm Hg to 40.5 ± 8.1 mm Hg in the same time frame (p < 0.05). In the hypothermia group, the CPP values significantly improved, from 81.9 ± 16.4 mm Hg to 87.0 ± 16.3 mm Hg at 3 h after cooling, while in the normothermia group, the CPP decreased from 78.5 ± 15.1 mm Hg to 57.7 ± 11.4 mm Hg in the same time frame (p < 0.05). In the hypothermia group, the PbrCO2 value decreased from 69.9 ± 7.4 mm Hg to 56.6 ± 11.3 mm Hg at 3 h after cooling, while in the normothermia group, the PbrCO2 values ranged from 70.5 ± 9.2 mm Hg to 72.4 ± 14.4 mm Hg in the same time frame (p < 0.05). In the hypothermia group, the pHbr value increased from 7.29 ± 0.16 to 7.37 ± 0.15 at 3 h after cooling, while in the normothermia group, the pHbr value decreased from 7.30 ± 0.17 to 7.19 ± 0.14 in the same time frame (p < 0.05). In the hypothermia group, the PbrO2 values ranged from 17.8 ± 3.6 mm Hg to 15.8 ± 3.7 mm Hg at 3 h after cooling, while in the normothermia group, the PbrO2 values were from 17.1 ± 3.3 mm Hg to 13.2 ± 2.6 mm Hg in the same time frame, but this difference was not statistically significant (p > 0.05; Fig. 2).
Discussion
In present study, we found that moderate hypothermia significantly decreases ICP, increases brain tissue pHbr, and reduces PbrCO2 (p < 0.05), but does not statistically significantly improve PbrO2. This indicates that the cerebral protection provided by moderate hypothermia most likely is not related to an improvement of cerebral oxygenation following intracranial hypertension.
The effects of moderate hypothermia on PbrO2 values following brain injury were inconsistent (Burger et al., 2004; Gupta et al., 2002). Burger and colleagues assessed the effects of moderate intra-ischemic hypothermia on cerebral oxygenation using an epidural balloon compression model in rats, and found that PbrO2 in the hypothermic animals was 19% higher than that of normothermic animals (p = 0.042). Further, they found that moderate hypothermia attenuated a secondary increase in ICP (p < 0.05), and electroencephalographic findings indicated a trend toward faster recovery (p > 0.05). Lesion size was reduced by 35% in MRI volumetric evaluations, and by 24.5% in histological morphometric analyses (Burger et al., 2004). Gupta and associates, investigating the effects of hypothermia on PbrO2 in 30 patients with severe TBI, demonstrated that brain parenchymal oxygenation was maintained with hypothermia to 35°C. However, they observed a significant decrease in PbrO2 below 35°C (p < 0.05), with a highly significant reduction seen below 34°C (p < 0.001) compared with 37°C, whereas PaO2 was increased below 37°C. PbrCO2 and arterial CO2 both decreased when brain temperature was reduced to 34°C. Their results imply that the neuroprotective effects of induced hypothermia may be most beneficial at a temperature of 35°C, as hypothermia to temperatures below 35°C may result in impaired cerebral oxygenation (Gupta et al., 2002). This shows that moderate hypothermia (33–34°C) does not significantly affect brain tissue oxygenation following acute intracranial hypertension after intracranial hematoma in pigs.
The differential effect of hypothermia on brain tissue oxygenation is not clear. Brain tissue oxygenation depends on the balance between oxygen delivery and consumption. Moderate hypothermia undoubtedly reduces cellular metabolism and oxygen consumption of brain tissue, which suggests that moderate hypothermia may increase PbrO2 values. However, moderate hypothermia may also cause a leftward shift of the oxygen dissociation curve, which enhances the affinity of oxygen to hemoglobin, causing reduced oxygen release, thereby reducing the availability of oxygen to diffuse into brain cells. Further, an oxygen delivery/metabolism mismatch may develop after head injury (Menzel et al., 1999), as a result of a combination of diffusion abnormalities (microvascular failure), arteriovenous shunts directing flow away from capillaries, increased diffusion distances because of cytotoxic edema, or mitochondrial abnormalities resulting from membrane alterations. All of these factors may contribute to the effect of moderate hypothermia on brain oxygenation following brain injury.
Our results clearly show that acute intracranial hypertension significantly decreases brain tissue pH, and that moderate hypothermia markedly attenuates decreases in brain tissue pH. In previous studies, researchers have found that cerebral lactate accumulation and acidosis occur following brain injury. Yang and colleagues performed tissue biochemical analyses, and found elevations of brain tissue lactate levels at 1 h after mild percussion injury (Yang et al., 1985). Inao and associates demonstrated a rise in brain tissue lactate content and a reduction in brain tissue pH, providing evidence for mild brain tissue acidosis caused by excessive lactate accumulation (Inao et al., 1988). Unterberg and co-workers also reported transient brain tissue pH reductions after severe fluid percussion injury as assessed by 31P MRS, confirming a mild tissue acidosis (Unterberg et al., 1988). Andersen and Marmarou demonstrated that whole brain lactate, as well as CSF lactate, increased after fluid percussion TBI, although the simultaneously measured cerebral blood flow was unchanged, suggesting that TBI itself, rather than secondary ischemia, caused this lactate increase (Andersen and Marmarou, 1992). They proposed the energy compartmentalization hypothesis to explain these findings, suggesting that mitochondrial function is depressed after brain injury, and that anaerobic glycolysis is facilitated. Further, Jiang and colleagues found that cerebral extracellular fluid lactate levels significantly increase following fluid percussion brain injury. Pre-injury mild hypothermia completely inhibits cerebral lactate accumulation, and early post-injury mild hypothermia significantly blunts the increases in cerebral lactate levels seen following fluid percussion injury (Jiang et al., 2004). Thus reductions in cerebral lactate content induced by moderate hypothermia may be related to the attenuation of decreased brain pH, and this may reduce brain acidosis following acute intracranial hypertension.
Footnotes
Acknowledgments
This work was supported by the National Key Basic Research Project (grant no. 2005CB522604), a National Science and Nature Grant (no. 30571908), the Science and Technology Committee of Shanghai (grant no. 04DZ14005), and the Program for Shanghai Outstanding Medical Academic Leader.
Author Disclosure Statement
No competing financial interests exist.