
Abstract
In severe pediatric traumatic brain injury (TBI), a common focus of treatment is raised intracranial pressure (ICP). The aim of this investigation was to test whether raised ICP is associated with later prefrontal executive deficits and regional brain tissue loss, consistent with an anterior vascular compartment syndrome. Thirty-three participants were assigned to one of two severe TBI groups based on whether or not they had increased ICP complicating their critical illness. At follow-up (average 3.9 years), the participants underwent magnetic resonance imaging and a battery of neuropsychological testing focused on prefrontal function. The ICP group had white matter loss that was diffuse as well as regional in the corpus callosum, periventricular tissue, and frontal region. Loss of gray matter in the ICP group was more regionally specific, with bilateral loss in the caudate nuclei and frontal regions, including the right dorsolateral region, right supplementary motor area, and the left orbitofrontal cortex. Both groups had normal intelligence quotients (IQs), but the ICP group showed long-term deficits on various measures of attention and executive function such as working memory, decision-making, and impulsivity. These findings suggest that raised ICP leads to diffuse brain injury and a predilection to hypoperfusion in, at least, the distribution of the anterior cerebral artery. Furthermore, since voxel-based morphometry (VBM) and measures of attention and executive function are sensitive to the phenomenon of raised ICP, we consider that these techniques warrant inclusion in trials assessing ICP-directed therapy.
Introduction
O
This failure to identify clinically useful therapies may be related to a failure to use appropriate assessments of outcome that specifically relate to the late consequences of acutely raised ICP, which is the physiology being targeted during the acute stage of illness. There is considerable literature on the structural and functional neuropsychologic effects of TBI that points to vulnerability of the frontal region. In children, severe injury can result in both focal and diffuse changes on magnetic resonance imaging (MRI). Focal lesions most commonly involve frontal and temporal lobes, the body and splenium of the corpus callosum, and the corona radiata. In the cortex, contusions frequently involve the inferior, lateral, and anterior aspects of the frontal and temporal lobes (Mendelsohn et al., 1992). In adults, an acute frontal lobe compartment syndrome is suggested by reports of frontal hypoperfusion (Prayer et al., 1993) and frontal metabolic crisis (Marcoux et al., 2008). Later, loss of gray matter in the frontal area is considered to relate to focal injury, whereas white matter loss is considered to relate to both diffuse and focal injury (Wilde et al., 2005; Kraus et al., 2007). At a functional level, frontal tissue is linked to executive cognition, and deficits in these areas of performance are well described after severe TBI in childhood (Levin et al., 1993; Garth et al., 1997; Slomine et al., 2002).
In this study we assessed neuropsychological measures of attention, memory, and executive function, and combined this with cerebral MRI morphometry late after severe TBI in childhood. Our aim is to test whether those individuals suffering raised ICP during the acute ictus exhibit dysfunction in prefrontal executive tasks and regional brain tissue loss consistent with an anterior vascular and frontal compartment syndrome. An additional intent of this research is to provide new tools for outcome assessment in clinical trials.
Methods
Patient recruitment and clinical characterization
The Institutional Review Board (IRB) for Human Studies (ethics review committee) of the Cambridge University Teaching Hospitals Trust approved this study, and informed consent was obtained from all participants and their families. All participants were survivors of TBI severe enough to necessitate endotracheal intubation, mechanical ventilation, and admission to our pediatric intensive care unit (PICU). Families were first approached during the acute ictus, and all potential participants had a record of investigations, monitoring, and treatment. These data included age at injury, post-resuscitation, preintubation Glasgow Coma Scale (GCS) score (Teasdale and Jennett, 1974), and whether neurosurgery was performed. Acute cranial computed tomography (CT) imaging was used to identify those with abnormal findings, particularly the presence of focal lesions in the frontal or temporoparietal regions. Exclusion criteria for this study were previously diagnosed neuropsychiatric disorder, previous hospitalization for TBI, clinically evident status epilepticus during acute ictus, subsequent epilepsy or anticonvulsant therapy, or developmental disorder.
All 33 participants were assigned, a priori, to a non-ICP or an ICP group using the duration of mechanical ventilation criterion developed in our previous study (Tasker et al., 2005). Twenty patients were in the non-ICP group; all of these patients were removed from mechanical ventilation within 3 days of admission. Thirteen patients were in the ICP group; they all underwent invasive ICP monitoring. The Pediatric Index of Mortality (PIM) score was used to describe overall pediatric critical illness risk-of-mortality (Pearson et al., 2001). The intensity of ICP-reduction therapies used in each case was scored using the Pediatric Intensity Level of Therapy (PILOT) scale (Shore et al., 2006). In the current analysis, the maximum daily score during admission was used as the summary measure.
A description of patients at the time of follow-up comprised the period of time after injury when they were unable to go to school (two categories: less than or greater than 2 months), age at follow-up, and a score using a pediatric adaptation of the Glasgow Outcome Scale: the King's Outcome Scale for Childhood Head Injury (KOSCHI) (Crouchman et al., 2001). In this description, ”favorable” outcome includes patients with either KOSCHI 4b (moderate disability with age-appropriate independence), KOSCHI 5a (mild deficits that do not interfere with function), or KOSCHI 5b (complete recovery). Height, weight, and occipitofrontal head circumference (OFC) were measured using standard procedures (Child Growth Foundation 1996 Growth Charts: Child Growth Foundation, London). Age- and gender-specific standard deviation scores (SDS) for all measurements were calculated using United Kingdom reference data (Freeman et al., 1995; Cole et al., 1998).
Neuropsychological assessment
Neuropsychological testing covered both general measures as well as prefrontal functions. The testing was divided into two sessions each lasting 1.5 h, separated by at least 1 week (Salmond et al., 2005a,b). The examiner was blinded to the ICP grouping and background data concerning the participants who were assigned to one of two groups of a differently randomized order of tasks. Several of the computerized tasks were taken from the Cambridge Neuropsychological Test Automated Battery (CANTAB, Cambridge Cognition Ltd., Cambridge, UK). Other tests included stop signal reaction time (Logan, 1994; Aron et al., 2003; Turner et al., 2003), information sampling task (Clark et al., 2006), Cambridge gamble task (Rahman et al., 2001; Turner et al., 2003), digit span (Wechsler, 1992 and 1997), and Rivermead Behavioral Memory Test (Wilson et al., 2003). In the analysis of the gamble task, a test-specific risk adjustment score was also calculated in order to assess the extent to which betting behavior was moderated by the ratio of boxes (Clark et al., 2008). An impulsivity index was calculated as the difference in percentage bet in descending versus ascending conditions (DeVito et al., 2008). Two participants from the non-ICP group had to be excluded from analysis of stop signal reaction time (SSRT) because their probability to inhibit response on stop tasks, p(inhibit), was either <0.4 or >0.6. By race-model estimation, this task allows a variation of the stop signal delay around an individual p(inhibit) = 0.5. However, these two participants responded either too fast (i.e., hardly having time to inhibit response should a stop-signal occur) or too slow (i.e., waiting too long even on Go trials in case a stop-signal occurred). Therefore, their SSRT would not provide a reliable measure of response inhibition.
Computerized tasks were run on a personal computer (model PPC-120T-RT; Advantech Taipei, Taiwan), and responses were registered either via the touch-sensitive screen or a response key, depending on the task. Participants were seated 0.5 m from the computer screen and asked to make responses with the index finger of their dominant hand. To familiarize the participants with the touch-sensitive computer screen and the procedures, the computerized tests were preceded by a “sensorimotor” task.
In order to evaluate any co-morbidity, participants or their parents completed the following: the Beck Depression Inventory-Youth (BDI-Y), by participants (Beck et al., 2001); the Conners' Rating Scales-Revised Short-Version (CRS-R:S) to assess symptoms of attention-deficit/hyperactivity disorder (ADHD), by parents (Conners, 2003); and the problem scales of the Child Behavior Checklist (CBCL/4-18), by parents (Achenbach, 1991). Intellectual ability was pro-rated from four tests (Vocabulary, Similarities, Block Design, and Picture Completion) of the Wechsler Adult Intelligence Scale (WAIS)-IIIUK (Wechsler, 1997) or the Wechsler Intelligence Scale for Children (WISC)-IIIUK (Wechsler, 1992) in those older or younger than 16 years, respectively (Clarizio and Veres, 1984; Kelly and Eyre, 1999). Three individuals were disabled in one hand and could not perform the block design task. Their full-scale intelligence quotient (IQ) was pro-rated from the three available scores.
Magnetic resonance imaging data acquisition and post-processing
A subgroup of the population (15 in the non-ICP group and 11 in the ICP group) underwent MRI scans performed on a Bruker Medspec 30/100 spectrometer (Bruker Medical, Ettlingen, Germany) attached to an Oxford 3.0-Tesla (T), 910-mm-bore whole-body, actively shielded, magnet (Oxford Magnet Technology, Oxford UK). A multi-oblique three-dimensional spoiled gradient-echo (3D SPGR) sequence was acquired using a repetition time (TR) of 19 ms, an echo time (TE) of 5 ms, a flip angle of 25°, a field view of 256 × 220 × 180 mm, and a matrix size of 256 × 220 × 180 (giving a spatial resolution of 1 × 1 × 1 mm).
One investigator, who was blinded to the patient information, made the volumetric measurements using ANALYZE software (Mayo Foundation, Rochester, MN). Reproducibility, as measured by intraclass correlation coefficient, was >95%. We used previously reported methods for the assessment of intracranial volume (ICV) and ventricular volume (Van Paesschen et al., 1997; Dalton et al., 2002). Ventricle-to-brain ratio (VBR%) was calculated as follows: VBR% = 100 × [ventricular volume]/[ICV] (Blatter et al., 1995). Hemisphere VBR% was calculated using hemisphere volumes, which were calculated from ICV measurements. A single mid-sagittal SPGR slice (defined by the septum pellucidum, an open third ventricle, and the absence or smallest size of the thalami) was used to measure corpus callosum area. After manually outlining the boundaries, the corpus callosum was divided into seven subregions as defined by Witelson et al. (1989) using ImageJ software (National Institutes of Health, Bethesda, MD). The hippocampus was measured with the SPGR slices re-orientated orthogonally to the longitudinal axis of the right hippocampus using our previously described method (Tasker et al., 2005).
The 3D SPGR scans were analyzed using Statistical Parametric Mapping software (SPM5, Wellcome Department of Cognitive Neurology, University College London, London, UK). Each scan was pre-processed in accordance with the protocol that has become known as “optimized VBM” (Ashburner and Friston, 2005). Briefly, voxel-based morphometry (VBM) is an automated technique that seeks to find significant differences between the brain tissue distribution between subject populations using structural MRI data. The algorithm comprises the following elements: coregistration of the brain into a standard space, i.e., normalization; segmentation of the brain into gray and white matter; and statistical comparison of these segments to find local differences. The optimized model of VBM that we used involves alternating among segmentation (tissue classification), bias correction, and spatial normalization (registration), all in the same model. Due to this optimized pre-processing, we decided that it was not necessary to create our own child template when using SPM5 (Wilke et al., 2002; M. Wilke, personal communication). However, in order to avoid inappropriate elimination of focal individual differences (e.g., regional deformities after TBI) that would reduce the sensitivity of the analysis, we limited non-linear normalization by using a high wrap frequency cut-off of 1000 (Eriksson et al., 2001). White and gray matter segmented images were smoothed with 12-mm isotropic Gaussian kernels, which render the voxel values as an index of the amount of gray (or white) matter per unit volume under the smoothing kernel. Inferences from the statistical parametric maps were made at the false discovery rate (FDR) and family-wise error (FWE) statistical threshold level, which is corrected for multiple comparisons across the entire brain (Genovese et al., 2002).
Statistical analysis
Analyses were carried out using the Statistical Package for Social Sciences (SPSS) version 15.0 (SPSS Inc., Chicago, IL). Statistical significance was set at p < 0.05.
The data describing clinical features and anthropometry were summarized using non-parametric statistics, presented as median and interquartile range. Comparison between groups was made using the median test for continuous and ordinal data, and the Chi-square (Fisher's exact) test for differences in proportions or categories. In the neuropsychological dataset, before the analysis, the raw data were tested for conformity to the normal distribution by using the Kolmogorov-Smirnov test, and were transformed in order to decrease skewness and stabilize variances where normality was violated. In the cases where normality was violated, non-parametric Mann-Whitney U-test results replicated the findings in the transformed data. Pass rates and gender differences were analyzed using the Chi-square test. Most other neuropsychological measures were analyzed using univariate or repeated measures analysis of variance (ANOVA) treating group and order as between-subject variables. Since many of the test measures varied with age, gender, and IQ, all analyses were performed with covariation for these three variables using analysis of covariance (ANCOVA). Data are presented as mean and standard error of the mean (SEM).
In the cerebral morphometry dataset, analyses of hippocampal volume, corpus callosum cross-sectional area, and ICV were undertaken on raw and corrected data. ICV values were corrected for OFC by multiplying the measured volume by a factor, whereby the fOFC = [mean OFC for entire population]/[observed OFC for the participant] (Kraus et al., 1990). Hippocampal volume was corrected for ipsilateral hemisphere volume—from which it was a part—by multiplying the measured volume by a factor, whereby fHC = [mean hemisphere volume of the entire population]/[observed hemisphere volume for the participant, left or right] (Blatter et al., 1995). Corpus callosum area was corrected by a factor, whereby fCC = [mean ICV for entire population]/[observed ICV for the participant]. Last, as left VBR% violated normality, VBR% data were analyzed using the Mann-Whitney U-test. All other data were analyzed by unpaired t-tests.
Correlations between the cognitive measures and values of gray and white matter were carried out within SPM. Correlations between the cognitive measures and the data obtained from cerebral morphometry were carried out within SPSS.
Results
Clinical characteristics
Table 1 summarizes the characteristics of the whole cohort and the two groups. In this series, median age at injury was 11.5 years. When the two groups (non-ICP and ICP) are compared, there was no difference in age at injury, sex, mechanism of injury, and proportion undergoing operation. The proportion of patients with abnormal CT scan was similar in the two groups. The proportion with focal lesions was also similar in the two groups: non-ICP versus ICP group with frontal lesions, 4/20 versus 5/13, p = 0.43; temporoparietal lesions, 9/20 versus 4/13, p = 0.49. At the time of injury, the ICP group underwent longer duration of ICP monitoring and more intense use of ICP-reduction therapies as shown by higher maximum PILOT scores.
Values shown for each variable are either median (interquartile range) or the proportion for each group. CT, cranial computed tomography; GCS, Glasgow Coma Scale; ICP, raised intracranial pressure; KOSCHI, King's outcome scale for childhood head injury; LOS, length-of-stay on the intensive care unit; MV, mechanical ventilation; OFC, occipitofrontal head circumference; PILOT, pediatric intensity level of therapy for intracranial pressure; PIM, pediatric index of mortality; RTA, road traffic accident; SDS, standard deviation score; yrs, years; mo, months.
After injury, those in the ICP group had taken longer to return to school. At the time of testing and MRI, the whole cohort were either employed, or in full-time education or vocational training. The median age at follow-up was 15.2 years, and the median interval between injury and assessment was 3.9 years. (There was no significant difference between the two groups, and the minimum interval between injury and assessment was 2.1 years.) Overall outcome was considered favorable in all 33 participants (i.e., KOSCHI 4b, 5a, or 5b). There was no difference in OFC, OFC-SDS, and height-SDS.
Neuropsychological assessment
There was no difference in IQ in relation to category of severe TBI: 98.0 ± 3.3 and 98.9 ± 2.7 in ICP and non-ICP groups, respectively. The results of individual tests are summarized in Table 2.
Values shown for each variable are the mean and standard error mean for each group. ANCOVA, analysis of covariance; ICP, raised intracranial pressure.
The key findings related to executive functions were as follows. In the test of spatial memory capacity, the ICP participants more often selected a box that was not at all in the sequence being recalled (total user errors: F(1, 28) = 4.950, p = 0.034). In spatial working memory performance, univariate ANCOVA revealed a higher strategy score in the ICP group compared with the non-ICP group, which indicates that ICP participants were applying a less effective search strategy. As expected, the amount of between errors increased per stage; i.e., the task was getting increasingly difficult with more boxes displayed. Repeated-measures ANCOVA revealed a main effect of group on between errors (F(1, 28) = 23.560, p < 0.001) and an interaction of group per stage (F(1, 28) = 9.037, p = 0.001). Further post hoc analysis showed that participants in the ICP group made more between errors on the more difficult stages (Fig. 1). There was no effect of group in the amount of within errors.
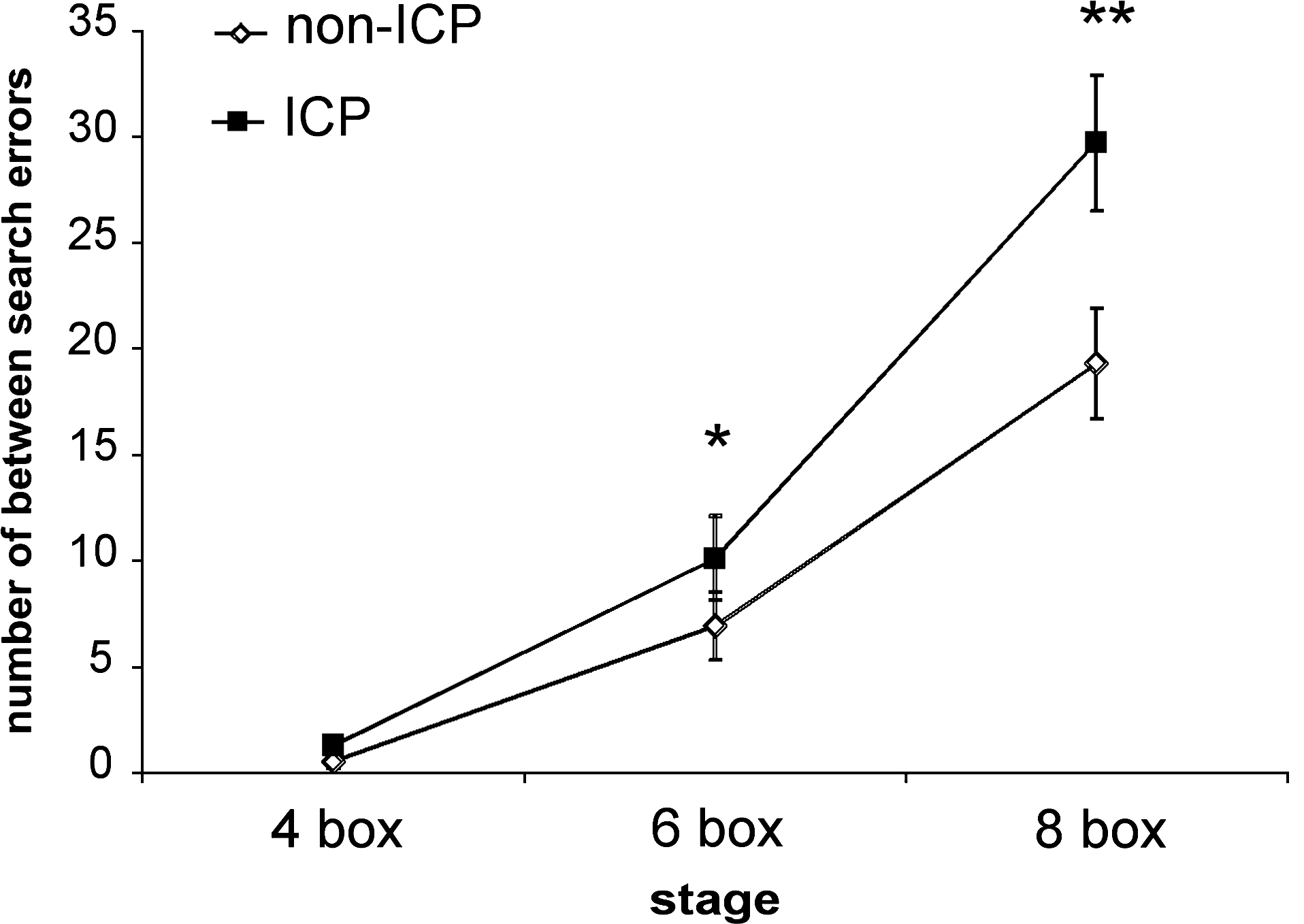
Results of spatial working memory task showing number of between search errors of the non—ICP (open diamond) and ICP (closed square) groups on the four-, six-, and eight-box stages. Values shown are the mean and standard error of the mean for each group (*p < 0.05, **p < 0.001). ICP, intracranial pressure.
In the test of pre-potent response inhibition, the two groups performed similarly on the Go task (median Go reaction time and Go discrimination errors). However, SSRT in the ICP group was significantly slower. We also found that SSRT was correlated with measures of spatial working memory: SSRT and strategy, Pearson correlation 0.431, p = 0.0167; SSRT and between errors, Pearson correlation 0.547, p = 0.001; and SSRT and within search errors, Pearson correlation 0.550, p = 0.001. In the information sampling task, a test of reflection impulsivity, using repeated-measures ANCOVA, revealed a main effect of order and a trend in group-and-order interaction on sampling errors (Fig. 2). The findings suggested that ICP participants tended to make more sampling errors than the non-ICP participants if they started with the decreasing-win situation.
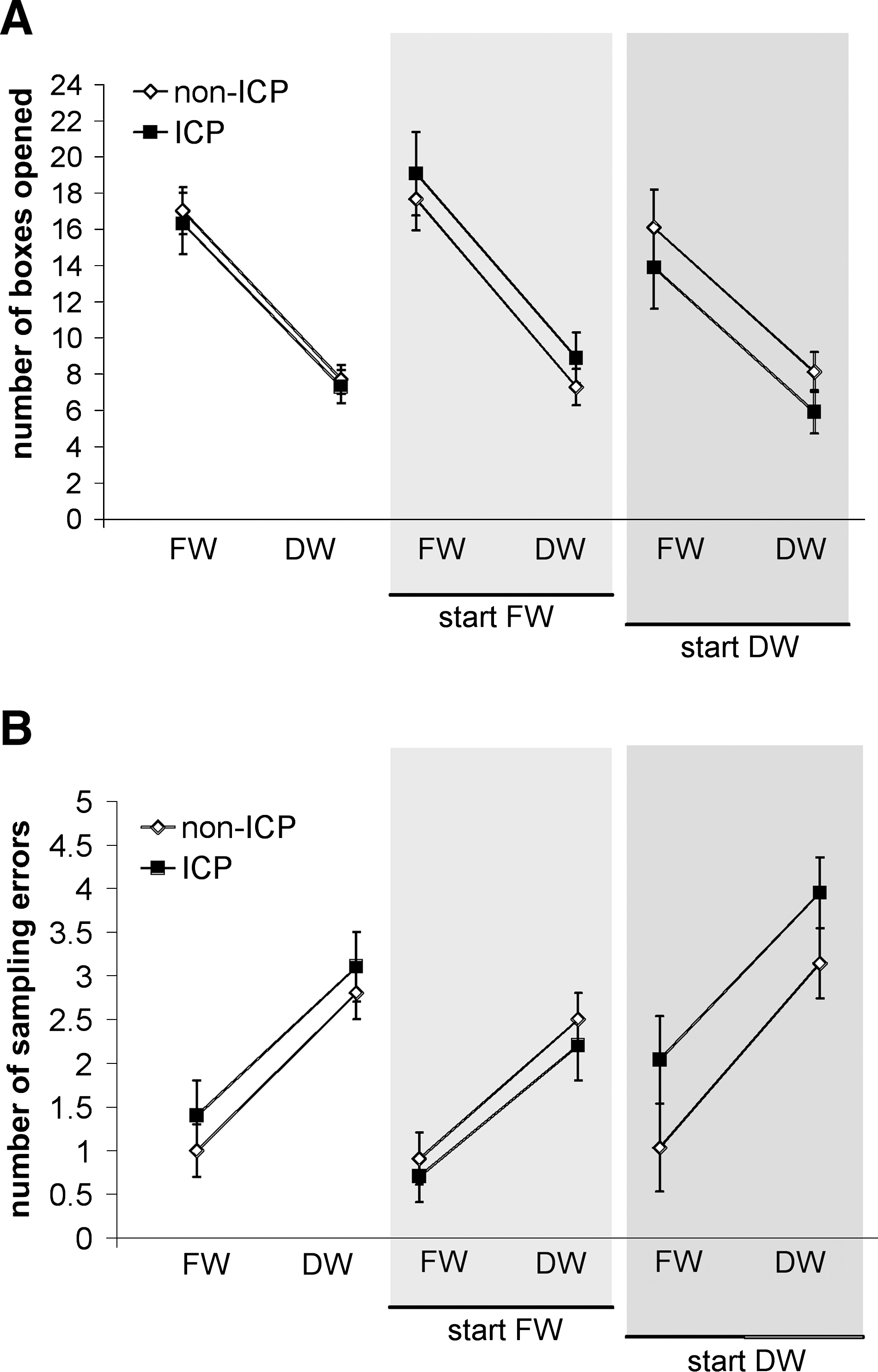
Results of information sampling task showing the effect of order on performance of the non—ICP (open diamond) and ICP (closed square) groups. Number of boxes opened (
In the Cambridge gamble task, a test of decision-making, the two groups behaved similarly regarding the probability of choosing the most likely outcome and the deliberation time. However, repeated-measures ANCOVA revealed a group-and-stage interaction on the percent bet (Fig. 3). Post hoc analysis showed that, on the most difficult stage (ratio 6:4), the ICP group placed higher bets, which occurred in both the ascending and the descending bets condition. The risk adjustment score was not lower for the ICP group for the Ascend task condition (ICP versus non-ICP: 69.97 ± 10.01 versus 90.40 ± 11.56, F(1, 28) = 2.7, p = 0.11), but it was lower for the ICP group on the Descend task condition: 41.61 ± 11.04 versus 71.05 ± 13.62, F(1, 28) = 7.0, p = 0.013. The impulsivity index was not significantly different in the two groups.
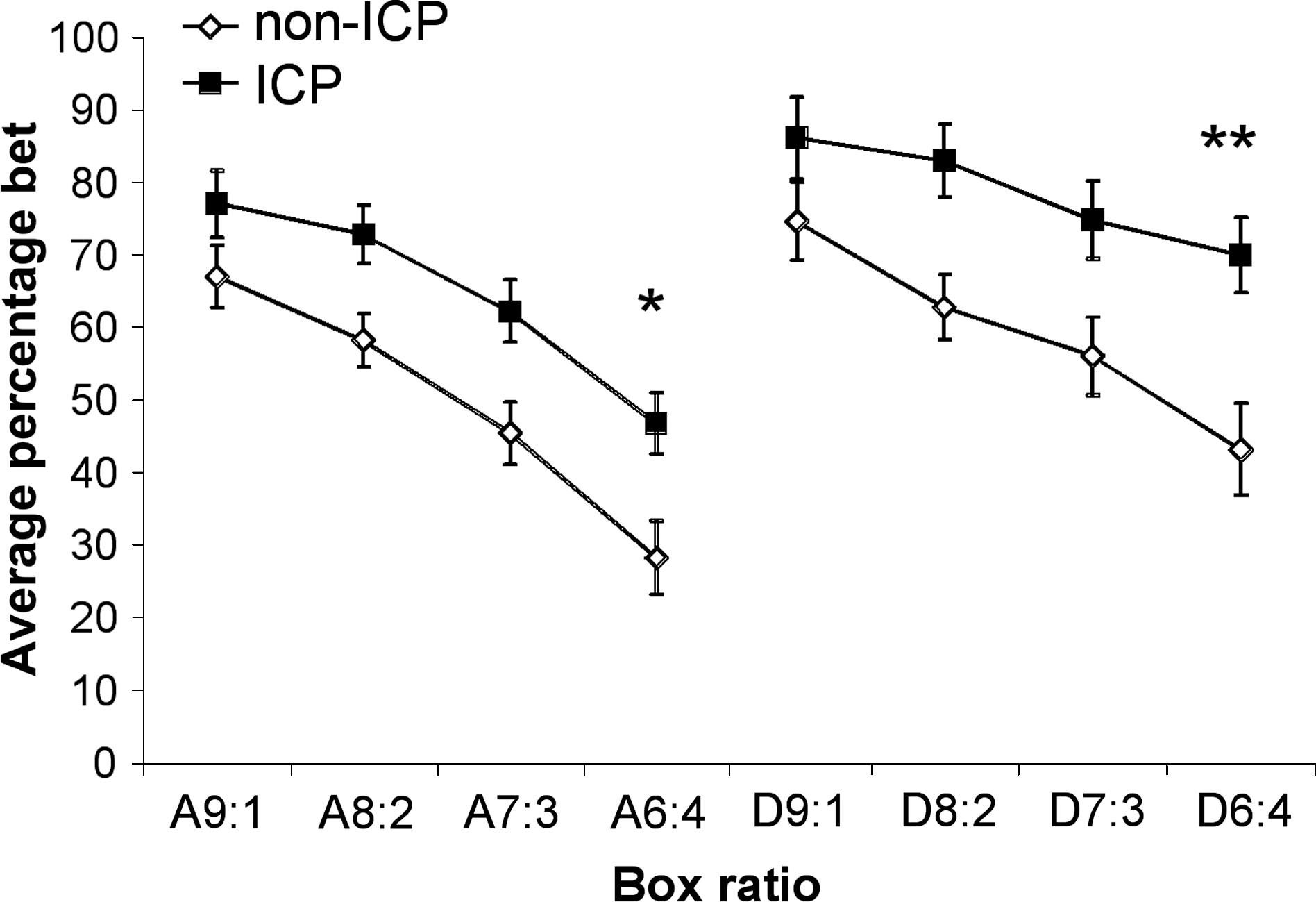
Results of Cambridge gamble task showing average percentage bet of the non—ICP (open diamond) and ICP (closed square) groups on different stages of the ascending and descending bets condition. Values shown are the mean and standard error of the mean for each group. p (group-and-stage interaction) = 0.006. *Ascending bets condition, stage 6:4; p (group) = 0.035. **Descending bets condition, stage 6:4; p (group) = 0.006. ICP, intracranial pressure; A, ascending; D, descending.
In the test requiring participants to learn a visual discrimination between two stimuli, the pass rate for the acquisition stage was no different between the groups. However, ICP participants had more difficulties with this stage than non-ICP participants. They made more errors before reaching criterion and needed significantly more trials before reaching criterion (26.0 ± 2.9 versus 14.2 ± 2.3 for ICP and non-ICP participants, respectively, F(1, 28) = 9.780, p = 0.004). In keeping with the increased number of errors before reaching criterion, ICP participants were more prone to respond to immediate negative reinforcement throughout the whole task, as reflected by higher probability matching score.
Last, in the test of everyday memory function using the Rivermead Behavioral Memory task, the mean score of the non-ICP participants was within the normal range, but performance of the ICP participants was in the range of poor memory (i.e., mild impairment, F(1, 28) = 10.106, p = 0.004).
Behavioral questionnaires
There were no group differences in total and sub-scores of the CBCL and of the CRS, which screen for a variety of behavioral problems. Mann-Whitney U testing of the CBCL scores revealed a trend towards higher T-scores for thought problems in the ICP group (57.8 ± 2.7 versus 52.0 ± 1.4, p = 0.052). On the CRS, the Chi-square test revealed a trend towards more ICP participants having scores that indicate significant attention problems (inattention six out of 13 versus two out of 20, p = 0.061).
There were no group differences in BDI-Y scores. Two participants in the ICP group had indication of moderate and severe depression, and two participants of the non-ICP group had indication of mild and severe depression. When these individuals were excluded from the analysis, the pattern of results for the whole sample remained the same as reported above, with the exception that there was no difference in the probability matching score of the probabilistic reversal task (F(1, 24) = 3.704, p = 0.066). In the gamble task, there was still a group-and-stage interaction, and ICP participants placed higher bets on the 6:4 stage of the descending bets condition, but not of the ascending bets condition (group-and-stage interaction: F(1, 24) = 3.873, p = 0.013; stage 6:4: ascending bets F(1, 24) = 3.713, p = 0.066; descending bets F(1, 24) = 8.373, p = 0.008).
Cerebral morphometry
Seven participants did not have a MRI scan because of metallic implants or anxiety. Consequently, 26 participants were scanned (11/13 of the ICP group and 15/20 of the non-ICP group). The neuropsychological profiles of the scanned subgroups were similar to the overall group profile as described above. However, differences between errors on the six-box stage of the spatial working memory task (p = 0.193), SSRT (p = 0.302), and the probability matching score in the probabilistic reversal task (p = 0.093) were not significant in this subgroup. Because of poor image quality, one subject from the non-ICP group had to be excluded from the more detailed measurements of hippocampal volumes and VBM.
In keeping with the follow-up anthropometry data (Table 1), the two groups did not differ in raw and OFC-corrected ICV (ICP versus non-ICP, mean ± SEM cm3): raw data, 1476.74 ± 32.24 versus 1472.81 ± 40.26, p = 0.943; and corrected data, 1457.26 ± 25.53 versus 1495.46 ± 28.28, p = 0.345. Table 3 shows that the two groups had differences in brain morphometry. In particular, ICP participants had increased VBR% in both hemispheres. Corpus callosum area was decreased in total and in most subregions, including anterior regions such as the genu and the anterior midbody. Figure 4 shows some representative images of the corpus callosum cross-sectional area, which illustrates thinning from anterior to posterior. There was no difference in hippocampal volume between the groups.
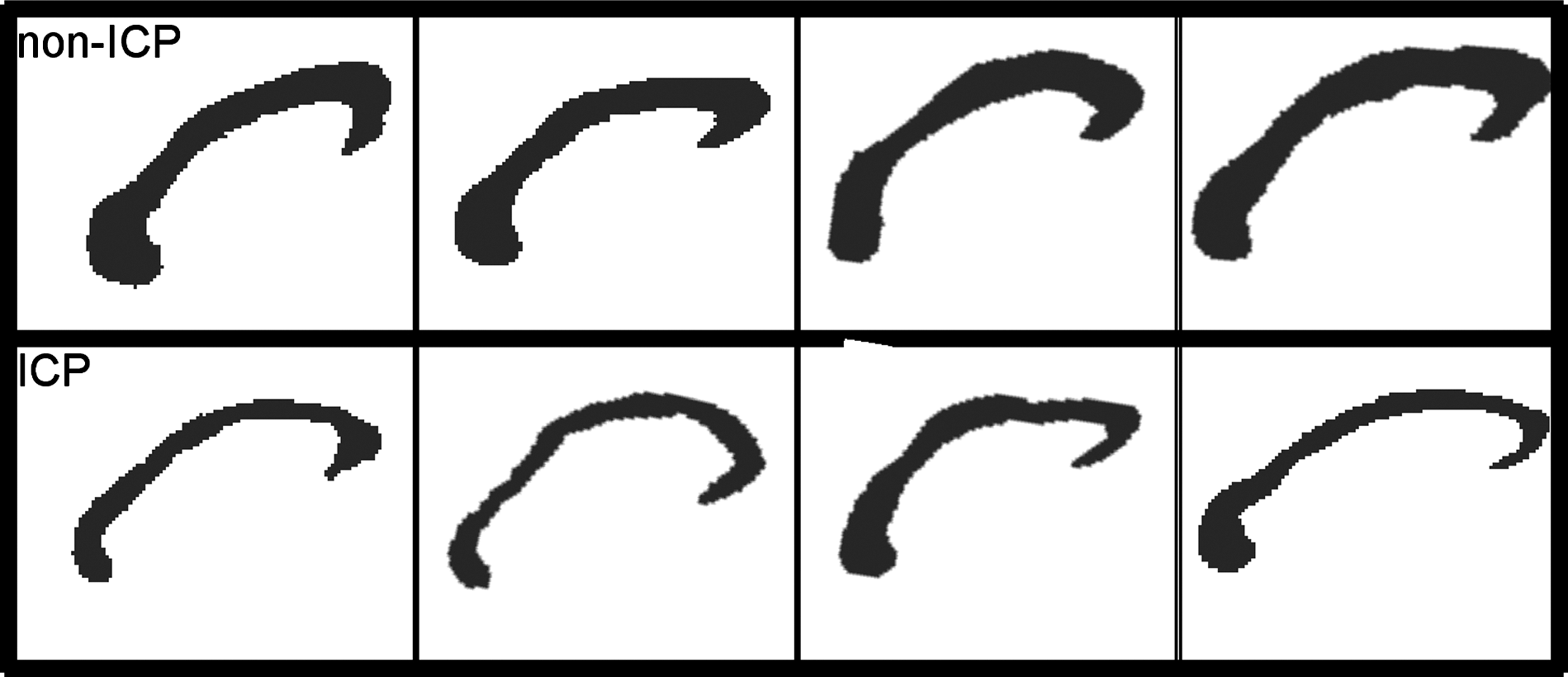
Representative corpus callosum cross-sectional areas at the midsgittal slice. (
Values shown for each variable are the mean and standard error mean for each group. Hippocampal volume and corpus callosum cross-sectional area are given as corrected values. ICP, raised intracranial pressure; VBR%, ventricle-to-brain ratio.
Table 4 summarizes the areas of brain where significant decreases in gray matter were identified in the ICP group using VBM. A highly significant decrease of gray matter was located in the right dorsolateral region. This area remained significant at FWE, p < 0.05. There were also significant decreases in other regions of the right and left frontal lobes, i.e., in the right supplementary motor area and the left orbitofrontal region. Another highly significant decrease was found in the left caudate, which extended to the right caudate (Fig. 5). Using a T-contrast for gray matter increases of the ICP group (compared with the non-ICP group) did not reveal any significant results. White matter differences are summarized in Table 5. The ICP group exhibited decreases in the corpus callosum, internal capsule, periventricular white matter tracts, and various association fibers underlying cortex in the frontal (particularly the right), parietal, temporal, and occipital lobes, including in the cerebellum (Fig. 6). A T-contrast for white matter increases of the ICP group (compared with the non-ICP group) did not reveal any significant differences.
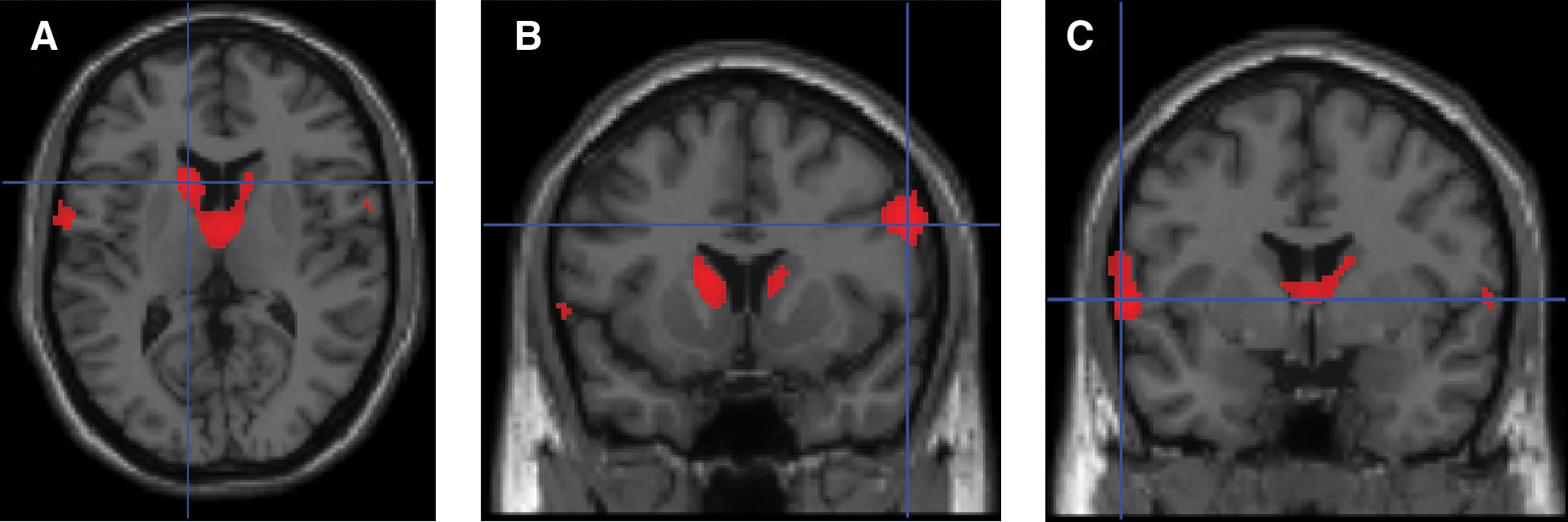
Voxel-based morphometry (VBM) analysis of gray matter density. Red indicates areas of decreased gray matter density. Images thresholded at false discovery rate (FDR); p < 0.01. (
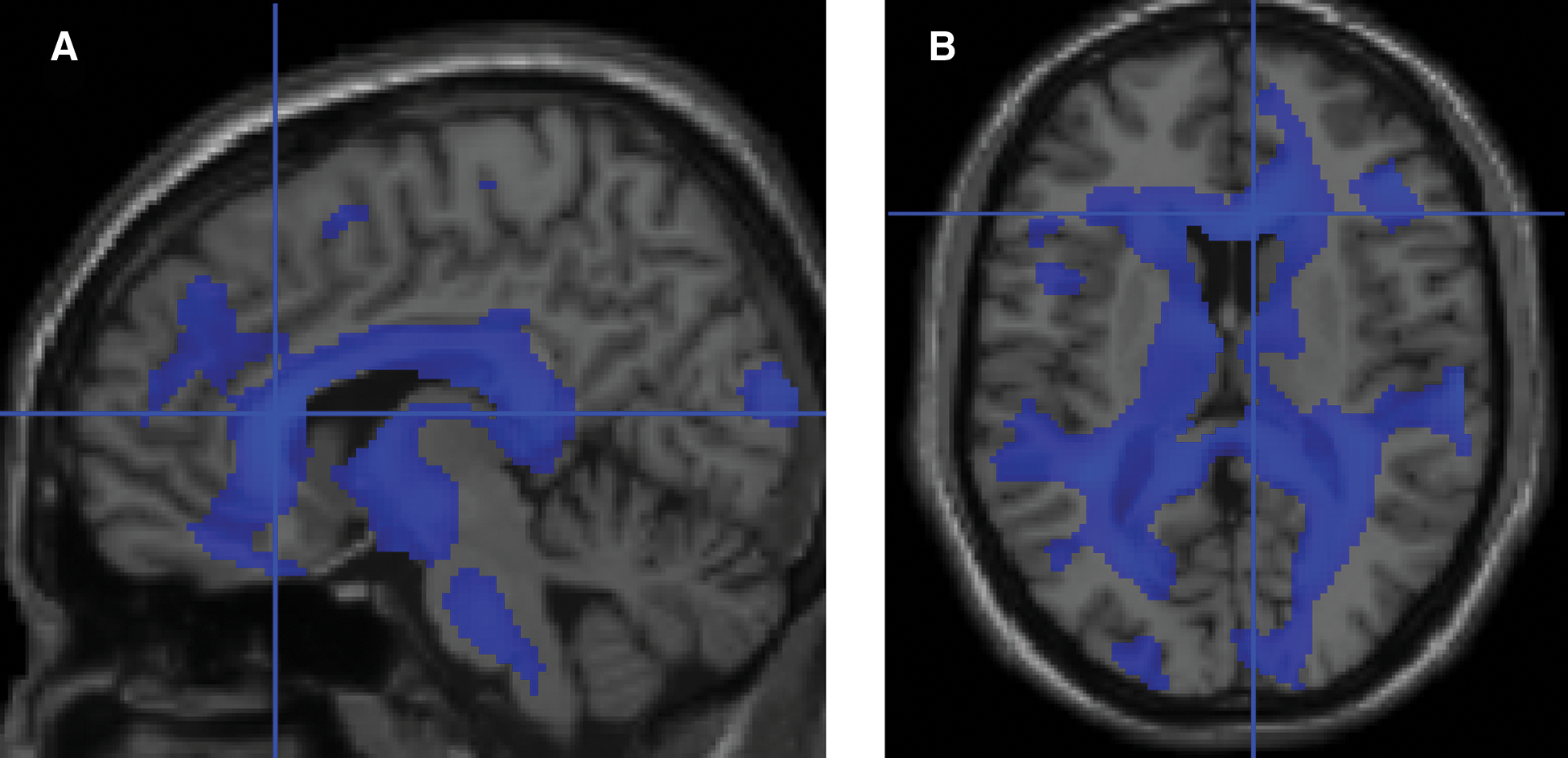
Voxel-based morphometry (VBM) analysis of white matter. Blue indicates areas of decreased white matter density. Images thresholded at false discovery rate (FDR); p < 0.05. (
Additional peaks in same anatomical regions not listed.
There were no significant correlations between cognitive indices and the cerebral morphological data independent of ICP grouping.
Discussion
This study shows that severe TBI in early adolescence, complicated by intracranial hypertension, results in a distinct cerebral morphometric pattern and neuropsychological profile. The cerebral morphometry showed increased VBR%, which is evidence of global brain tissue loss. Consistent with this finding, whole-brain image analysis showed white matter loss that was diffuse, with specific changes in the anterior one-third of the corpus callosum, periventricular tissue, and frontal regions. Loss of gray matter was more regionally specific, with bilateral loss in the caudate nuclei and frontal regions, including the right dorsolateral region, right supplementary motor area, and left orbitofrontal cortex. In both methods that were applied, there was no gray matter loss in the hippocampus. The neuropsychology showed impaired executive function and only mild deficit in episodic memory. These findings are consistent with the idea that raised ICP in severe TBI leads to diffuse brain injury and a predilection to hypoperfusion in, at least, the distribution of the anterior cerebral artery (ACA).
Before discussing our findings, we need to consider three areas where there may be limitations to our study. First, in studying sequelae of raised ICP complicating TBI, we have, by definition, selected young people who have suffered injury resulting from a range of accidents, with a variety of secondary insults and heterogeneous intracranial pathologies. Despite these potential problems, we have still found that, late after injury—almost 4 years—a distinct pattern of intracranial vulnerability emerges. Second, our study population may be considered small, and at an age when maturation and development are continuing, even though the participants were seen late in adolescence. This limitation could mean that any potential findings are still evolving or recovering. However, the fact that these age-related changes are occuring renders adolescence a critical period for frontal brain structural and cognitive functional development. We have tried to control for this bias by seeing subjects a minumum of 2 years after injury. Even though the size of the study is small, the composite analyses and concurrence of neuropsychological and morphological results are internally consistent. Third, there may have been the following technical limitations in the image analysis.
Partial volume effects may have influenced the measurement of corpus callosum cross-sectional area. However, this source of error would have been common to both groups, and it is unlikely to explain the gross findings that were consistent in the two techniques we used (Figs. 4 and 5). As an alternative, measurement of corpus callosum volume might have added further confirmatory evidence of this diffuse white matter injury. Errors may have been introduced during VBM analysis. For example, all of the scans are coregistered in stereotactic space using an automated algorithm that minimizes a measure of difference between the image and a template. We did not have a child template for SPM5, and the use of an adult template in young children and infants is certainly problematic (Wilke et al., 2003). However, the median age of our subjects at the time of MRI was ∼15 years, which is late in brain development. Creating our own custom-made template for this age group, with our limited “controls,” would not have captured enough variance, and so we would have been at risk of over-identifying differences. It is possible that the accuracy of normalization in the ICP group was compromised by the presence of focal lesions in some of the patients. We minimized these errors by not using non-linear transformations, which are especially vulnerable to inappropriate distortions (Brett et al., 2001; Eriksson et al., 2001). It is also possible—since VBM segmentation is primarily driven by the intensity level in the structural image—that lesioned areas are inappropriately classified as gray or white matter. We did not find this to be the case on visual inspection of the data. We also confirmed that the normalized images did not contain distortions. Last, there is the possibility that the gray matter decrease in the caudate nuclei in the ICP group is an artefact produced by VBM analysis when enlarged ventricles are present. However, if this anomaly were present, it would also have led to significant gray matter increase in the ICP group in the regions around the caudate nuclei, which we did not find.
Raised ICP complicating severe TBI and ACA hypoperfusion
This report is about the effect of raised ICP complicating TBI severe enough to warrant endotracheal intubation, mechanical ventilation, and treatment on an intensive care unit, rather than the effect of moderate-to-severe (i.e., GCS score ≤12) head injury per se. Modern resuscitation practices in TBI now mean that the definition of severe TBI using GCS ≤8 is unreliable in the patient undergoing emergency endotracheal intubation and supportive mechanical ventilation (Ghajar, 2004; Saatman et al., 2008). We have therefore separated our TBI patients according to the duration of mechanical ventilation, which is a surrogate marker of raised ICP in this population (Tasker et al., 2005). The actual presence of raised ICP is further demonstrated in this study by the duration and intensity of ICP-reduction therapies using the PILOT scale. This scale has been validated in children with extracranial trauma, mild-to-moderate TBI (GCS 9–12), and severe TBI (GCS ≤ 8) (Shore et al., 2006). The highest daily PILOT scale scores (∼12) are seen in severe TBI, and other categories of patients have a score of ∼2. A daily PILOT scale score of >8 denotes use of second tier ICP therapies (e.g., aggressive hyperventilation, barbiturates, or hypothermia); of ≥5 to 8 denotes use of the range of first tier ICP therapies (e.g., sedation, analgesia and neuromuscular blockade, mannitol and hyperosmolar therapy, and mild hyperventilation); and of 1–4, the initiation of neurocritical care (Adelson et al., 2003). The median PILOT scale score in our ICP group was 10, and in the non-ICP group it was 4. Our patients, therefore, can be classed as severe cases receiving ICP-directed therapy at two different levels: first tier in the non-ICP group and second tier in the ICP group. More severe GCS is linked to the increased likelihood of developing raised ICP and more intense therapies, but by focusing selection on raised ICP, rather than on some measure of the acute injury such as GCS, we have identified a unique distribution of deficits in cerebral morphology and neuropsychology, which together indicate a causative hemodynamic substrate.
Anatomical findings at the higher tier of therapy (i.e., raised ICP group) show diffuse cerebral white matter pathology, including the corpus callosum, compounded by regional gray matter pathology, particularly in the anterior cranial fossa. We have previously reported diffuse white matter loss in TBI related to a complex interaction between the side of the head sustaining impact, ictal hemisphere edema, and focal hemorrhage, in cases where cerebral atrophy was evident (Tasker et al., 2005). On further inspection, we found that the white matter loss was most likely a result of regional perfusion failure rather than swelling, because there was ipsilateral hippocampal, and not peri-hippocampal, tissue loss, which indicates a hypoxic-ischemic mechanism. This same perturbation and effect in the end-arterial borderzone between centripetal and centrifugal vessels supplying the centrum semiovale (Van Den Bergh, 1969; Van Der Eecken, 1969) may have been present in our current series, but the new subjects differ from those in our previous study. They were older at the time of injury, and the bicyclists wore protective helmets. The absence of hippocampal tissue loss and marked deficit in episodic memory in the current group of ICP subjects may, therefore, reflect a difference in age and localization of injury. Rather than experiencing a similar type of focal injury, the current ICP group may have had a more dissipated hemisphere injury at the time of impact, as reflected by the temporal and parietal morphometric findings observed on follow-up.
It has been suggested that frontal loss of white matter is related to both diffuse and focal injury, whereas loss of gray matter is attributable to focal injury (Mendelsohn et al., 1992; Wilde et al., 2005). This explanation could account for the regional decreases in gray matter found in the ICP group. However, at the time of injury, there was no difference between the two groups in the proportion with abnormal scans or the proportion with frontal lesions. As an alternative explanation, we should consider hypoperfusion as a cause of both white and gray matter changes (Prayer et al., 1993; Berryhill et al., 1995). That is, hemodynamic failure in the distal and perforating branches of the ACA is a common link between corpus callosum thinning and frontal gray matter loss (Tables 4 and 5). For example, the pericallosal and callosomarginal arteries and other branches originating from the ACA A2-A5 segments supply the anterior four-fifths of the corpus callosum and precuneus. Perforators arising from A1 and A2 segments supply the orbitofrontal and supplementary motor areas of the frontal lobe. The Heubner artery, originating from the A2 segment, supplies the anterior limb of the internal capsule and head of caudate. Penetrating branches of the anterior communicating artery (origin at the junction of the A1 and A2 segments, in close proximity to the origin of the Heubner artery) supply structures including the anterior part of the corpus callosum, the inferior frontal lobe, and the cingulum (Brust and Chamorro, 2004). The ACA distribution does not explain all of the VBM findings, but it raises the possibility that a diffuse problem (as evidenced by the diffuse white matter loss) was further compounded by tissue hemodynamics related to raised ICP in the anterior cranial fossa. This idea is consistent with the vulnerability of the basal forebrain (supplied by the ACA and anterior communicating artery) in moderate-to-severe head-injured adults (Salmond et al., 2005a) and children (Herskovits et al., 1999).
Neuropsychological outcome of severe TBI in relation to level of raised ICP
All of the participants were successfully rehabilitated into further education or employment. Using a dichotomous grading system (similar to that applied to outcomes assessment in randomized controlled trials of interventions used to limit raised ICP in severe TBI), all of the participants would also have been classed as having “favorable“ outcome (Lu et al., 2008). Furthermore, IQ was normal, with no difference between the groups. These observations highlight a potential problem underlying trials in severe TBI in children. The outcome measurement used, although indicative of functional integration into the community, is not a sensitive measure of mechanism causing secondary pathology (i.e., raised ICP), nor does it correlate with the degree of cerebral pathology induced by this mechanism. Therefore, the following discussion will focus on the deficits consistent with the anatomical topography observed in the ICP group. In this report, we found that adolescents with severe TBI requiring more intense ICP-reduction therapies showed long-term deficits on various measures of attention and executive function such as working memory, decision making, and impulsivity.
Participants in the ICP group had impaired spatial working memory such that they made more between search errors and had a less efficient strategy. They also had significant decrease in gray matter in the right dorsolateral prefrontal cortex (PFC). Working memory functions are key features of the PFC, and in particular, the dorsolateral PFC is considered to be responsible for the executive component of working memory, i.e., monitoring and allocating processing resources (Owen et al., 1996). In addition to other areas such as the ventrolateral PFC, cingulate gyri, and parietal cortex, the basal ganglia and the white matter tracts in the anterior part of the corpus callosum are also involved in the neural circuitry of working memory (Herskovits et al., 1999; Castellanos, 1997). Loss of white matter in these regions occurred in the ICP group. Deficits in spatial working memory, including higher between search errors and a less efficient strategy, have been demonstrated in adults with large frontal (including ventral and dorsal parts) or dorsolateral lesions (Manes et al., 2002). In contrast, subjects with temporal lesion or amygdalohippocampectomy show no impairment in strategy and between search errors except at the most difficult stage (Owen et al., 1996). Functional imaging studies suggest that the dorsolateral PFC in the right hemisphere—which was a region of injury in our ICP group—is activated in tasks of non-verbal, spatial working memory (McCarthy et al., 1996; D'Esposito et al., 1998).
The ICP group also exhibited risky decision-making on the Cambridge gamble task, particularly when the likelihood of winning was reduced. Such a profile has also been shown in adults with subarachnoid hemorrhage of the anterior communicating artery (Mavaddat et al., 2000) or with frontal variant of frontotemporal dementia, and in cases with large frontal lesions, but not with lesions restricted to either orbitofrontal, dorsolateral, or dorsomedial areas (Rahman et al., 2001; Manes et al., 2002; Clark et al., 2008). These observations make it unlikely that dorsolateral gray matter loss causes this deficit, but at the same time it seems to be attributable to frontal dysfunction. The difficulties in risky decision-making may be consistent with the ACA A1-A2 pattern of vascular lesion we observed. An alternative possibility is that the finding represents a non-specific effect of side-of-injury (i.e., right hemisphere), since increased betting has been shown in subjects with right frontal, but not left frontal lesions (Clark et al., 2003). Survivors of severe TBI during adulthood also have difficulties in decision-making on the gamble task, although the effect of raised ICP has not been assessed (Salmond et al., 2005b). A recent study in adults with insular lesions shows a similar patttern of placing higer wagers only when the ratio of boxes was 6:4, which is when the probability of losing is greatest (Clark et al., 2008). However, the risk adjustment score in this group of subjects was much poorer, whereas that of our ICP group was more in the range of the comparison group in the Clark et al. (2008) study, i.e., adults with ventromedial frontal lesions. Others have reported that this region of brain is frequently affected in TBI in children (Berryhill et al., 1995; Wilde et al., 2005, 2007).
In adults, deficits in stop-signal inhibition have been closely linked to reduced volume of the right inferior frontal gyrus (Konishi et al., 1998; Aron et al., 2003). We also found impaired response inhibition associated with decreased gray matter in the right inferior frontal gyrus in the ICP group. A study in adults with right frontal lesions and ADHD showed that the volume of the right inferior frontal gyrus is critical for both response inhibition and spatial working memory function (Clark et al., 2007). In keeping with this observation we also found that SSRT was correlated with measures of spatial working memory. Impaired response inhibition after severe TBI in childhood is a measure of impulsiveness (Konrad et al., 2000; Levin et al., 2004), and it would appear that impaired response inhibition is only a consequence of TBI when the child manifests high levels of secondary ADHD symptoms (Schachar et al., 2004). We did not find any correlation between SSRT and parental ratings for ADHD symptoms (data not shown). Rather, it appeared to be a general feature of the ICP group.
Conclusion
In young adolescent survivors of severe TBI—requiring one of two levels-of-intensity in ICP-reduction therapy during the acute ictus—the topography of later cerebral tissue loss and neuropsychological profile indicates previous anterior vascular compartment syndrome complicating the physiology of raised ICP. This late finding may mean that more severe focal injury is associated with a more severe level of ICP, or that the higher tier of ICP-reduction therapy compromises frontal perfusion. Alternatively, variation in the vascular anatomy of the frontal lobes (Brust and Chamorro, 2004) may make this tissue particularly vulnerable to diffuse swelling with alteration in end-arterial vascular dynamics within the anterior cranial compartment. These hypotheses warrant further evaluation and, in part, they support the renewed interest in the vulnerability of the frontal lobes in severe TBI (Marcoux et al., 2008) and the use of early decompressive craniectomy (Jagannathan et al., 2007; Schirmer et al., 2008; Timofeev et al., 2008). The findings in this report also inform the ongoing debate about the significance and treatment of raised ICP complicating TBI (Morris et al., 2006; Cremer, 2008; Saatman et al., 2008). Last, the imaging and neuropsychology tools we have used in a group who would be classed as achieving “favorable” outcome show that these measures are sensitive to the ictal physiology (and its later outcome), which is the target of therapy. Such measures also warrant further consideration and inclusion in randomized controlled trials of therapy.
Footnotes
Acknowledgments
We wish to thank the patients and families who participated in this study, and the staff in the Department of Paediatrics and Radiographers at the Wolfson Brain Imaging Centre. The Medical Research Council (G9439390), the Addenbrooke's Charitable Trust, and the Evelyn Trust supported this work.
Author Disclosure Statement
No competing financial interests exist for the following authors: Helen Slawik, Claire Salmond, Joana Taylor-Tavares, Guy Williams and Robert Tasker. Professor Barbara Sahakian is a scientific consultant for Cambridge Cognition Ltd. (Cambridge, MA), the developer and marketing company for the CANTAB neuropsychology testing.