
Abstract
The QOLIBRI (Quality of Life after Brain Injury) is a novel health-related quality-of-life (HRQoL) instrument specifically developed for traumatic brain injury (TBI). It provides a profile of HRQoL in six domains together with an overall score. Scale validity and factors associated with HRQoL were investigated in a multi-center international study. A total of 795 adults with brain injury were studied from 3 months to 15 years post-injury. The majority of participants (58%) had severe injuries as assessed by 24-h worst Glasgow Coma Scale (GCS) score. Systematic relationships were observed between the QOLIBRI and the Glasgow Outcome Scale-Extended (GOSE), Hospital Anxiety and Depression Scale (HADS), and SF-36. Within each scale patients with disability reported having low HRQoL in two to three times as many areas as those who had made a good recovery. The main correlates of the total QOLIBRI score were emotional state (HADS depression and anxiety), functional status (amount of help needed and outcome on the GOSE), and comorbid health conditions. Together these five variables accounted for 58% of the variance in total QOLIBRI scores. The QOLIBRI is the first tool developed to assess disease-specific HRQoL in brain injury, and it contains novel information not given by other currently available assessments.
Introduction
Appreciation that patient-reported outcomes (PRO) are of key importance has led to an increased interest in quality of life after TBI (Bampoe et al., 2002; Fuhrer, 2000; Hawthorne et al., 2009; von Steinbüchel et al., 2005b). Recent work has shown that a wide variety of factors influence well-being, life satisfaction, and health-related quality of life (HRQoL) in persons after TBI, including loss of autonomy (Mailhan et al., 2005), emotional state (Corrigan et al., 2001; Koskinen, 1998), and level of participation (Pierce and Hanks, 2006). Measurement of subjective HRQoL is of importance in clinical trials, where PRO are increasingly seen as essential to providing a complete assessment of the effects of treatment (Chassany et al., 2002; Guyatt et al., 1989; Patrick et al., 2007). Patient reports have the advantages of yielding information about treatment effects known only to the individual, providing a unique perspective on subjective outcome, and avoiding the potential loss of information that can occur when patient responses are filtered through a clinician (FDA Ctr Drug Evaluation Res, 2006). A common interest among experts in TBI is to identify patient-relevant outcomes that are more fine-grained than well-established measures of functional recovery such as the Glasgow Outcome Scale (GOS; Maas, 2000).
Generic measures of subjective health status, such as the Short-Form Health Survey-36 (SF-36), contrast with disease-specific HRQoL, insofar as disease-specific instruments may capture specific aspects of life that the generic functional instruments do not. Therefore disease-specific instruments may be more relevant to the patients and more sensitive to the consequences of particular health conditions. A major shortcoming to date has been the absence of a disease-specific measure of HRQoL for TBI patients (Berger et al., 1999). The lack of such an instrument prompted the formation of an international group to develop an appropriate measure (Bullinger and The TBI Consensus Group, 2002; von Steinbüchel et al., 2005a). A multidimensional view of HRQOL was adopted, encompassing well-being and functioning in physical, psychological (cognitive and emotional), social, and daily life domains, with the person viewed as the best source of information on his or her subjective state (von Steinbüchel et al., 2005b). The resulting questionnaire for HRQoL after brain injury, the Quality of Life After Brain Injury (QOLIBRI) survey, encompasses six domains that are known to be affected by injury. The purpose of this article is to report findings concerning the validity of the QOLIBRI from a large-scale international study, to consider the clinical and research value of the new instrument, and to examine correlates of HRQoL after TBI. A separate article describes the steps in the development of the QOLIBRI, the psychometric properties of the individual items and scales, and contains further information concerning methods (von Steinbüchel and the QOLIBRI Task Force, 2010).
Methods
Participants
Centers using six language versions of the QOLIBRI (Dutch, English, Finnish, French, German, and Italian), recruited a total of 921 participants with TBI who were living in the community or in a rehabilitation center. Inclusion criteria for the study were: ICD-10 diagnosis of traumatic brain injury, 3 months to 15 years post-injury, aged 15 years or more at injury, outpatient status, aged 17–68 years at interview, and able to give informed consent. Exclusion criteria were: Glasgow Outcome Score-Extended (GOSE) score <3; spinal cord injury; significant current or pre-injury psychiatric history; ongoing severe addiction; inability to understand, cooperate and answer; and having a terminal illness. In order to ensure a well-characterized sample the current analysis is confined to 795 participants for whom both an initial GCS score and a follow-up GOSE score were available.
Measures
The 24-h worst GCS score (Teasdale and Jennett, 1974) score was obtained from medical records. Brain injury severity was classified into mild (GCS 13–15), moderate (GCS 9–12), and severe (GCS 3–8).
The QOLIBRI consists of 37 items in six scales and is summarized in Table 1. Four scales contain ‘ “satisfaction” items, and two scales have “bothered” items; responses are made on a 5-point scale from “not at all” to “very.” The QOLIBRI gives a profile of quality of life in six domains relevant for TBI, together with a total quality-of-life score.
QOLIBRI, Quality of Life after Brain Injury.
The GOSE was used as an assessment of functional status (Wilson et al., 1998). Classification on the GOS was obtained by collapsing the extended categories: Severe Disability (GOSE 3–4), Moderate Disability (GOSE 5–6), and Good Recovery (GOSE 7–8). Depression and anxiety were assessed using the Hospital Anxiety and Depression Scale (HADS; Zigmond and Snaith, 1983); scores of 8–10 represented mild cases, 11–15 moderate cases, and 16 or above severe cases (Snaith and Zigmond, 1994). The SF-36 (Ware and Sherbourne, 1992) was used as a patient-reported generic health outcome measure. We defined a low SF-36 score as lying one standard deviation below the mean of the normative sample, and a very low score as two standard deviations below the norm.
Patients also provided social and demographic information, including age, gender, relationship status, educational background, occupation, level of independence, number of social contacts, participation in leisure activities, and use of alcohol and recreational drugs. In addition, a health questionnaire covering 28 comorbid health conditions and problems adapted from Power and associates (2005) by von Steinbüchel and colleagues (2006) was used, as was a questionnaire on help needed in five specific areas (personal needs, mobility, activities of daily living, transportation, and organization, and management), including five items in 5-point Likert scale format. Interviewers completed a checklist that covered information concerning clinical background, including post-traumatic amnesia and current medication, and a rating of disorders in 10 areas (epilepsy, hemiparesis, visual and auditory deficits, extra-cerebral injuries, communication problems, attention dysfunction, memory dysfunction, executive dysfunction, and affective and behavioral disorders).
Data collection
The procedure was as follows: Initial contact was made to obtain consent and to arrange for the questionnaires to be completed. Centers were instructed that if participants were able to fill in the questionnaires without help, then they should be self-completed, and the questionnaires could be mailed to them if this was more convenient. If the person needed help, then assistance should be arranged (usually face-to-face contact). In the case of face-to-face contact, the GOSE and interviewer checklist were completed at the same time. If postal administration was used for the questionnaires, then the GOSE and clinician checklist were completed using a telephone interview.
Data analysis
Data analysis was carried out using SPSS 16.0 (SPSS Inc., Chicago, IL). Item scores on the QOLIBRI “bothered” scales were reversed to match the “satisfaction” questions. Means were calculated for each QOLIBRI scale, prorated if no more than one-third of items were missing, and expressed as a score from 0 (lowest possible HRQoL measured by the questionnaire), to 100 (best possible HRQoL). A total QOLIBRI score was also calculated as the mean of all individual items, using prorating if necessary.
Validity was assessed by examining the relationship between the QOLIBRI scales and three sets of variables: (1) demographic and clinical characteristics, (2) disability and emotional state, and (3) generic health outcomes. Construct validity was examined by calculating correlations between QOLIBRI scales and variables in sets (1), (2), and (3). We analyzed relationships with both Spearman and Pearson correlations to help to establish whether parametric approaches could appropriately be applied to the data. Many of the variables significantly deviated from a normal distribution (i.e., were skewed). We therefore used ranked data in the regression and partial correlation analyses (Conover and Iman, 1981). The SPSS 16 “rank variables” routine was used to create rank variables, assigning lowest ranks to lowest expressions of the original continuous variables. We compared generic subjective health outcome as assessed by the SF-36 and the QOLIBRI as a HRQoL measure for TBI. Partial correlations of scale scores were used to compare the strength of the relationships of the QOLIBRI and the SF-36 with the disability-specific outcome measure, the GOSE.
Furthermore, proportions are reported to help make HRQoL data more meaningful in clinical contexts (King and Fayers, 2008). We also collated the responses in the lowest two categories (“not at all” or “slightly” satisfied, and “quite” or “very” bothered). Proportions of low responses were calculated for each of the scales by dividing the total number of such responses by the number of items in the scale. This gives a measure of the proportion of items on which the person indicates poor HRQoL. The total proportion of low responses was calculated in a similar manner using all QOLIBRI items.
Finally, the scale scores of variables in groups (1) and (2) were converted to ranks, and their contribution as independent predictors of HRQoL was examined using step-wise linear regression analysis. For this analysis, missing values of variables were replaced by the mean. The criterion for inclusion in the final model was that the variable should independently explain 1% or more of the variance (increase in R2 > 1%).
Results
The mean age of the 795 cases (573 male) was 39 years (SD = 13.3 years), and the mean period of follow-up was 5 years (SD = 3.9). The majority of patients (58%) were severely injured, 10% had moderate injuries, and 32% had mild injuries. Brain injury rehabilitation centers were a major source of recruitment to the study: 255 participants (33%) were currently in rehabilitation, and 397 (51%) had been in rehabilitation. The highest education levels were: primary school (5.7%), secondary school (25.0%), trade/technical certificate (29.5%), college diploma/degree (23.4%), and university degree (11.9%). Further information about the sample is given in Table 2, and is contained in von Steinbüchel and the QOLIBRI Task Force (2010). Comparison of Spearman and Pearson correlations (Table 3) shows that no difference exceeds 0.06, and this helps to justify parametric approaches to data analysis.
GOSE, Glasgow Outcome Scale-Extended; HADS, Hospital Anxiety and Depression Scale; SF-36, Short-Form Health Survey-36; MCS, Mental Component Score; PCS, Physical Component Score.
???; **???; ***???.
QOLIBRI, Quality of Life After Brain Injury; GOSE, Glasgow Outcome Scale-Extended; HADS, Hospital Anxiety and Depression Scale; SF-36, Short-Form Health Survey-36; MCS, Mental Component Score; PCS, Physical Component Score.
The questionnaires were completed by self-report in a face-to-face situation (n = 240), by face-to-face interview (n = 215), by mail (n = 325), and by telephone interview (n = 13). The main centers using postal contact were in Finland and Germany, and the return rates were 60% in both cases. A one-way analysis of variance (ANOVA) comparing QOLIBRI total scores for the three main administration modes (self report, interview, and mail) was not significant [F(2,778) = 2.77; p > 0.05]. The internal consistency of the QOLIBRI total score was high for the three administration modes (0.94–0.96), and test-retest reliabilities ranged from 0.87–0.91. Further information concerning the reliability of the QOLIBRI is given in von Steinbüchel and the QOLIBRI Task Force (2010).
Influence of demographic factors and clinical background
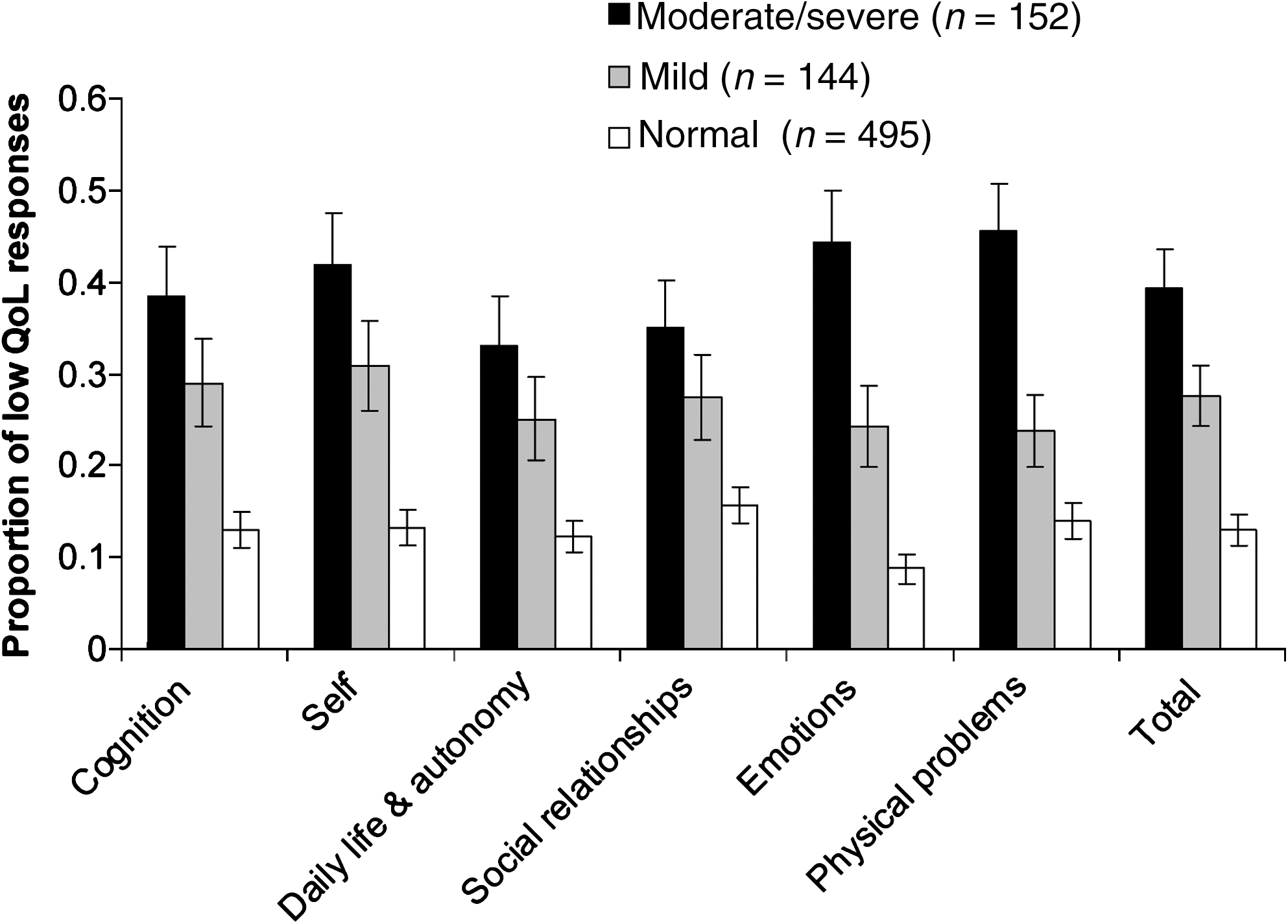
Relationships between the QOLIBRI scales and demographic and clinical characteristics are summarized in Table 3. In general, effects of age, education, time since injury, and severity of injury (GCS) were very weak (all r = .11 or less; see Table 3 and Fig. 1). On the other hand, current comorbid health conditions showed a significant relationship with all QOLIBRI scales, and had a particularly strong correlation (r = .56) with the Physical Problems scale (Table 3).

QOLIBRI and GCS severity category: mean proportions (and 95% CIs) of responses indicating low quality of life (low QoL; QOLIBRI, Quality of Life After Brain Injury; GCS, Glasgow Coma Scale; CI, confidence interval).
Relationships with disability and emotional state
There were significant relationships between the need for help in daily life (clinical list) and the QOLIBRI, and particularly the “Daily Life & Autonomy” and “Physical Problems” scales (r = −.52 and −.41, respectively). There are significant relationships between the GOSE and all QOLIBRI scales (Table 3 and Fig. 2); the strongest relationship was with the “Daily Life & Autonomy” Scale (r = .42), and the weakest was with the “Emotions” scale (r = .19). From Figure 2 it is apparent that participants with severe disability (143, 18% of the sample) reported many more areas of poor HRQoL than those who had good recovery, on average two or three times as many on most of the QOLIBRI scales. The figure also shows that the moderately disabled group (433, 54%) had poorer HRQoL than those with good recovery (219, 28%).

QOLIBRI and outcome category on the GOSE: mean proportions (and 95% CIs) of responses indicating low quality of life (low QoL; QOLIBRI, Quality of Life After Brain Injury; GOSE, Glasgow Outcome Scale-Extended; CI, confidence interval).
There were systematic relationships between the QOLIBRI and emotional state (Table 3 and Figs. 3 and 4). Using conventional cut-off points for the HADS, 132 (17%) participants were classified as having moderate or severe depression, and 152 (19%) were classified as having moderate or severe anxiety. Another 120 (15%) had mild depression, and 144 (18%) mild anxiety. Relationships with the HADS were observed with all QOLIBRI scales, suggesting a general impact of emotional state on all aspects of HRQoL. Effects of the HADS anxiety scale and depression scale (both categorized in three levels: no, mild, and moderate/severe) were significant for all scales in all individual language versions. Effect sizes for the QOLIBRI total score and Anxiety Scale and Depression Scale were >.10 for all language versions. The strongest relationships with specific QOLIBRI scales were between the HADS depression scale and the self scale (r = –.62), and the HADS anxiety scale and the emotions scale (r = –.62; Table 3).

QOLIBRI and the HADS Depression Scale: mean proportions (and 95% CIs) of responses indicating low quality of life (low QoL; QOLIBRI, Quality of Life After Brain Injury; HADS, Hospital Anxiety and Depression Scale; CI, confidence interval).
QOLIBRI and the HADS anxiety scale: mean proportions (and 95% CIs) of responses indicating low quality of life (low QoL; QOLIBRI, Quality of Life After Brain Injury; HADS, Hospital Anxiety and Depression Scale; CI, confidence interval).
QOLIBRI and SF-36
Around one-third of participants had low mental well-being as indicated by SF-36 MCS one SD or more below norms, and a quarter had low physical well-being as indicated by low PCS. The proportions of patients with very poor mental and physical well-being were 14% and 7%, respectively. Relationships between the QOLIBRI scales and the SF-36 MCS and PCS are summarized in Table 3, and illustrated in Figures 5 and 6. The PCS was most strongly related to the Physical Problems scale (r = .63), while the MCS was most strongly associated with the Emotions scale (r = .61; Table 3). The relationships observed with the total QOLIBRI score suggest that the QOLIBRI has more in common with the MCS than the PCS of the SF-36. For the six language versions, the correlation with the total QOLIBRI score was r = .48 or more for the MCS, and r = .39 or more for the PCS.
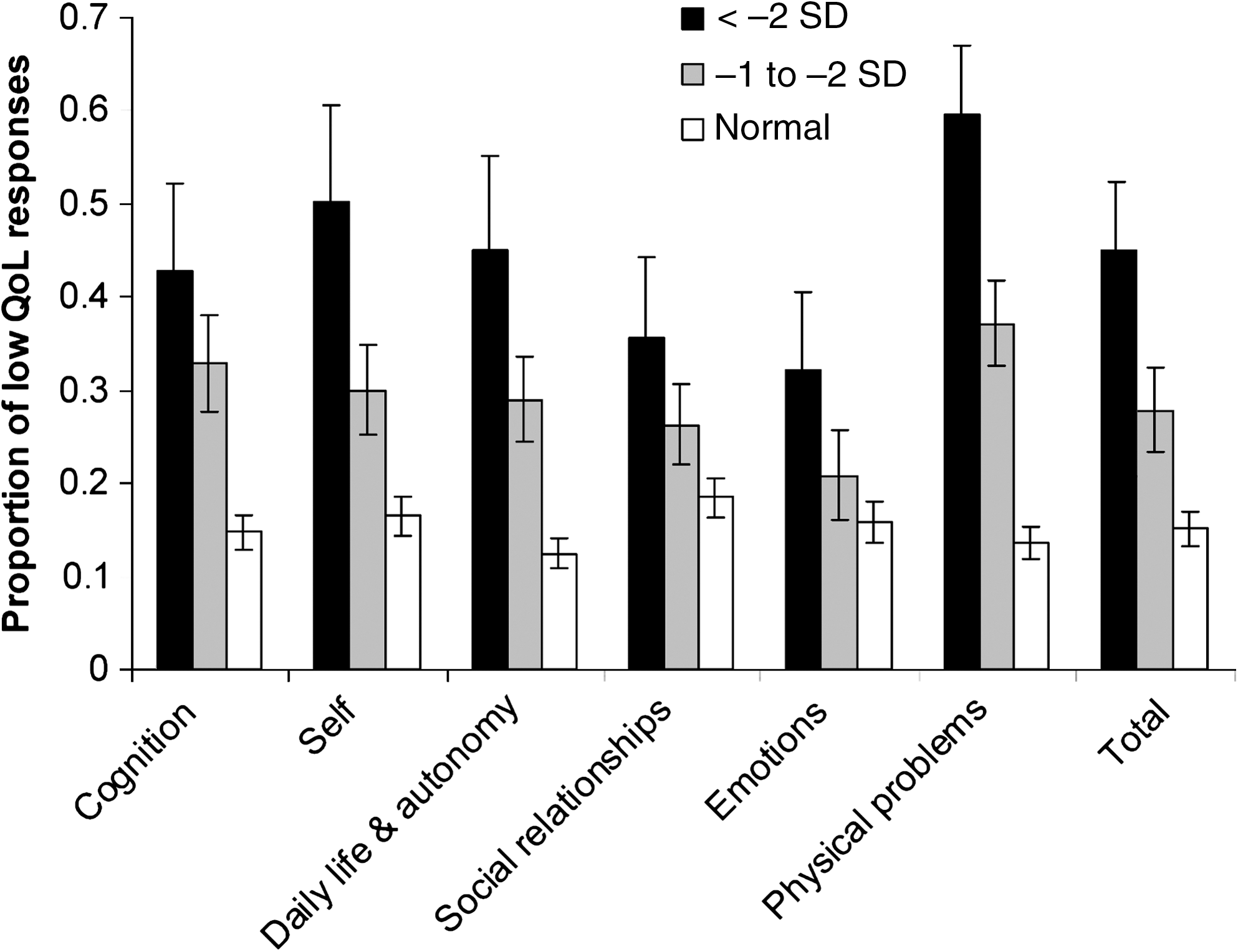
QOLIBRI and SF-36 Physical Component Score: mean proportions (and 95% CIs) of responses indicating low quality of life (low QoL; QOLIBRI, Quality of Life After Brain Injury; SF-36, Short-Form Health Survey; CI, confidence interval).

QOLIBRI and SF-36 Mental Component Score: mean proportions (and 95% CIs) of responses indicating low quality of life(low QoL; QOLIBRI, Quality of Life After Brain Injury; SF-36, Short-Form Health Survey; CI, confidence interval).
The question of whether the QOLIBRI performs as well as the SF-36 as a HRQoL measure for TBI was studied by investigating relationships with the GOSE, a TBI-specific functional outcome measure. The correlation between the GOSE and QOLIBRI total was r = .39. This was significantly larger than the correlation between the GOSE and the MCS, r = .20 (z for the difference = 6.52; p < 0.001), and similar to the correlation between the GOSE and the PCS, r = .34 (z for the difference = 1.61; p = 0.054). The partial correlation between the GOSE and QOLIBRI total scores was still highly significant when controlling for MCS (r = 0.36; p < 0.001), whereas the correlation between the GOSE and MCS disappeared when controlling for QOLIBRI (r = −0.05; p = 0.22). This analysis indicates that outcome-related information captured by the SF-36 mental health component score is also captured by the QOLIBRI, but there is additional information available from QOLIBRI scores that is lost when only the MCS is considered.
Predictors of quality of life
Stepwise linear regression was carried out, using the QOLIBRI total score as the dependent variable. The analysis identified five predictors, each of which independently explained at least 1% of the variance in the QOLIBRI total (Table 4). These were (in descending order of importance) HADS depression (rank-transformed raw scores ranging from 0–20), the degree of help needed (rank-transformed sum of the five 5-point items, range 0–25), comorbid health conditions (rank-transformed sum of 28 yes/no items, ranging from 0–28), HADS anxiety (rank-transformed raw scores ranging from 0–20), and rank-transformed GOSE score (3–8). Together the five correlates explained 58% of the variance in the QOLIBRI total (Table 4). A number of other variables were considered, including age, education, GCS score, years since injury, administration mode, and language version, but these were excluded from the final model, either because they were only weakly associated with the QOLIBRI (explained less than 1% of the variance), or their contributions were mediated by one or more of the five main predictors.
Variables were excluded if they explained less than 1% of the variance.
QOLIBRI, Quality of Life After Brain Injury; GOSE, Glasgow Outcome Scale-Extended; HADS, Hospital Anxiety and Depression Scale.
Discussion
The QOLIBRI captures multiple aspects of health-related quality of life, encompassing the physical, psychological (emotional and cognitive), social, and functional domains (von Steinbüchel et al., 2005a). The domains assessed are specifically important in TBI, reflecting changes that are identified as common in this group: cognitive consequences (Dikmen et al., 2003), changes in the sense of self (Prigatano, 1992), alterations in social relationships (Mazaux et al., 1997), limitations to activity and participation (Ponsford et al., 1995), emotional problems (Hoofien et al., 2001), and physical problems caused by injury. HRQoL in some of these areas is not well assessed or not assessed at all by other measures, and the tool is thus unique in covering areas that are typically affected by brain injuries.
The results show the expected pattern of relationships with other scales, thus confirming the validity of the QOLIBRI. Particular patterns of relationships in the findings (Table 3) are consistent with expectations: The SF-36 PCS has its highest correlation with the QOLIBRI Physical Problems scale (.63), and a similar pattern is seen for Comorbid health conditions (.60). The HADS anxiety scale correlates most strongly with the QOLIBRI Emotions scale (−.64), and HADS depression with the Self scale (−.62). The SF-36 MCS correlates most highly with the Emotions (.62), and Self (.56) scales. Help needed with activities correlates most highly with the Daily Life (−.53) and Physical Problems (−.47) scales. As would be expected, the strongest correlations with the GOSE are with Daily Life (.43) and Physical Problems (.40).
The new scale provides additional information not provided by the GOSE, HADS, or SF-36. In the current study the overall relationship between the GOSE and the QOLIBRI was only moderate, indicating that people could have poor outcome on the GOSE and have good HRQoL and vice versa. The results thus imply that some people adjust well to the consequences of disability, while others do not. Understanding successful adjustment, and the factors that can promote it, is a major challenge for future research.
Regression analysis showed that the strongest predictors of QOLIBRI scores are aspects of current status, and specifically emotional state, comorbid health conditions, and functional outcome, while demographic and clinical background factors have little if any influence. It is perhaps not surprising, given the average length of time since injury, that GCS played little if any role, and the current finding is in accordance with the work of others (Dikmen et al., 2003). It is known that most psychosocial and cognitive changes happen during the first 3–4 years after TBI (Truelle et al., in prep.); however, most of the patients in the present study were assessed about 5 years after TBI. Since awareness of deficits improves over time (Hart et al., 2009), the low correlation between time since injury and QOLIBRI seems to argue against a significant influence of impaired self-awareness in our data. This argument is also supported by the high Mini Mental State Examination scores (MMSE; Folstein et al., 1975) of most participants (see von Steinbüchel and the QOLIBRI Task Force, 2010). The results of regression analysis are consistent with previous reports of an association between quality of life and emotional state (Corrigan et al., 2001; Koskinen, 1998; Underhill et al., 2003), and loss of independence (Mailhan et al., 2005). The association of depression and HRQoL is an ubiquitous finding in other diseases, but it is acknowledged that HRQoL goes beyond simply assessment of the emotional state (Gladis et al., 1999; Höfer et al., 2005). It is noteworthy that some of the dominant factors that influence HRQoL appear to be potentially modifiable.
A notable finding is the extent to which low HRQoL is reported by participants. The results of the comparison with the GOSE show that in each domain of the QOLIBRI, disabled TBI participants indicate low HRQoL in two or three times as many areas as those who had good recovery. It is particularly noteworthy that patients with moderate disability reported significantly lower HRQoL than those with good recovery. The findings argue against the common assumption that someone with moderate disability has a “good” outcome, and potentially point to the need for interventions to help this group. In this context it should be emphasized that moderate disability was not only the most common outcome of TBI in the current group, but it is more generally a frequent outcome in people hospitalized with brain injuries of all severities, even those with apparently mild injuries (Thornhill et al., 2000).
The HADS indicated that 17% met criteria for moderate or severe depression. The latter indicates a level of emotional distress that could benefit from intervention, and the figure here contrasts with an expectation that 4% would meet this criterion in a non-clinical sample (Crawford et al., 2001). Similarly, on the SF-36, the proportion of cases with very poor mental (14%) and physical (7%) well-being is higher than the 2.3% expected for a normally distributed T-score. The results from the HADS and SF-36 thus indicate that a subgroup had significant problems in mental and/or physical well-being, and the findings on the QOLIBRI suggest that this may be only the tip of the iceberg. One could argue that the relatively high incidence of depression in the present sample might be due to the convenience sampling employed by many of the participating centers, possibly leading to over-representation of the more distressed people. However, the incidence of 17% clinical depression found here fits well in the typical range reported in the TBI literature (e.g., Jorge et al., 2004), and a comparison of HADS depression scores between the centers employing consecutive/random sampling (Germany and Australia; n = 235), and those employing convenience sampling (Belgium, Finland, France, Italy, Netherlands, the U.K., and the U.S.A.; n = 560) did not reveal significant differences.
The GOS/GOSE is currently the most popular outcome measure in acute brain injury trials; however, it is widely acknowledged that this assessment has limitations. It does not address some important domains, including cognition (Berger et al., 1999; Dijkers, 2004). As an assessment of functional outcome it does not capture the subjective evaluation of the individual. In brain injury the interest in HRQoL has been fueled in part by the failure of clinical trials in the acute stage to demonstrate clinical benefit using functional outcomes as a primary end-point (Narayan et al., 2002). The development of a disease-specific HRQoL measure for TBI opens the possibility of constructing a composite outcome assessment that covers both functional outcomes and HRQoL. Such a composite assessment would avoid some of the obvious limitations of the GOS, would help to complete the picture of outcome after brain injury, and potentially give a more sensitive assessment for clinical trials.
Outcome measures assessing TBI-specific HRQoL may contribute to quality control in short- and long-term care, medical decision-making, and rehabilitation planning. In clinical use in the rehabilitation setting, it can help to identify and set appropriate goals for therapy. A challenge here is to include an element of individualization in an assessment that has simplicity and broad applicability (Dijkers, 2003). In clinical practice it can be useful to supplement the QOLIBRI with questions about whether the person is bothered by specific problems, such as for example seizures, legal issues, ability to drive, stigmata, and sleep problems.
The current study has some important limitations. The study was intended to validate the QOLIBRI, and it was therefore desirable to collect data from a large sample of brain injuries with a wide variety of clinical characteristics. The majority of TBI participants were recruited as convenience samples. Collection of control data from representative healthy individuals in different centers was beyond the scope of the present study. The resulting study sample is a large and heterogeneous TBI group that is good for validation purposes, but in which there are significant clinical and demographic differences in the cohorts recruited in the different centers and over different time intervals since injury. Country-to-country differences in clinical and demographic characteristics are not atypical of international TBI databases (Murray et al., 1999), and partly reflect differences in management of brain injuries in different clinical settings. The current study was not designed to allow comparison of HRQoL of patients with TBI in different countries, although this would undoubtedly be interesting to investigate. Similarly, although participants were followed-up over a wide range of intervals after injury, the cross-sectional design here does not allow a straightforward analysis of recovery over time. An issue that therefore remains unresolved is the responsiveness of the QOLIBRI to change. The results show that the QOLIBRI is sensitive to differences in outcome on the GOS and other functional indicators. However, a longitudinal study is needed to investigate the responsiveness of the QOLIBRI-TBI to change over time. Finally, it was beyond the scope of the study to investigate impairment of self-awareness in the whole sample, and we cannot rule out the possibility that a minority of participants had poor insight (Bivona et al., 2008). We were able to establish for the total sample that level of cognitive function did not affect the reliability of reports (von Steinbüchel and the QOLIBRI Task Force, 2010). However, the specific issue of the influence of deficits of self-awareness on reported HRQoL is an important topic for further research (Malec et al., 2007).
In conclusion, the QOLIBRI provides a profile of health-related quality of life in domains that are relevant for TBI, as well as a summary score of overall HRQoL. Systematic relationships were observed between the QOLIBRI and the GOS, HADS, and SF-36, confirming the validity of the new instrument. It is suggested that the QOLIBRI is a useful tool for assessing disease-specific HRQoL in TBI, that contains information not yielded by other currently available assessments.
Footnotes
Acknowledgments
The QOLIBRI Task Force consists of collaborating investigators in the following countries (*Steering Committee, †Methodological Group): Argentina (Armando Basso), Australia (Graeme Hawthorne†), Austria (Stefan Höfer†), Belgium (Christine Croisaux, Andrew Maas*), Brazil (Lucia Braga), China (Wai Poon, Zhang Tong), Denmark (Anne-Lise Christensen), Finland (Jaana Sarajuuri, Sanna Koskinen), France (Philippe Azouvi, Michelle Montreuil, Pierre North, Jean-Luc Truelle*), Germany (Monika Bullinger,*† Henning Gibbons,† Edmund Neugebauer,* Tanja Lischetzke,† Nadine Sasse, Silke Schmidt,† Nicole von Steinbüchel,*† Klaus von Wild,* Wolfgang Woerner†), Greece (Eva Tazopoulou), E. Wahjoepramono (Indonesia), Italy (Rita Formisano), Japan (Yoichi Katayama), the Netherlands (Wilbert Bakx, Peter Vos), Poland (Maria Pachalska), Portugal (Sandra Guerreiro), Russia (Boleslav Lichterman), Taiwan (Wen-Ta Chiu), United Kingdom (Richard Greenwood, Jane Powell,* Lindsay Wilson†), United States of America (John DaVanzo, George Zitnay*).
Author Disclosure Statement
No competing financial interests exist.