
Abstract
Wearing protective helmets decreases the risk of incurring traumatic brain injury (TBI) in bicycle accidents. In 2007, the German Neurosurgical Society advocated compulsory use of bicycle helmets. Although neurosurgeons are the specialists who primarily treat patients with TBI in Europe, the distribution of helmet users among neurosurgeons (NS), as well as factors that influence the decision to wear helmets and whether professional knowledge or experience in TBI influences the use or attitude concerning bicycle helmets, remains unclear. A total of 55 neurosurgical departments in Germany, Austria, and Switzerland were contacted and asked to answer anonymous questionnaires concerning helmet use and TBI experience. To compare the neurosurgical attitude with that of a “non-neurosurgical, non-TBI-educated” control group, people of the general public (PUB) were interviewed. A total of 465 NS and 546 PUB returned questionnaires, with 49.7% of the NS and 44.5% of PUB indicated that they wear helmets while bicycling. Trauma experience did effect the personal decision of whether to wear bicycle helmets. Support of compulsory use was influenced by TBI experience. Furthermore, the incidence of helmet use in children was correlated to actual helmet use and disposition of their parents to make helmet use compulsory. NS and PUB behaved in similar ways. Only half wear protective helmets, while the others show cognitive dissonant behavior. With respect to compulsory helmet use, NS are also split in half. Experience with TBI and trauma education has effects. However, education alone does not suffice in promoting the use of bicycle helmets.
Introduction
W
Although the use of helmets is reported to lead to a significant decrease in the risk of TBI after bicycle accidents (Abu-Zidan et al., 2007; Attewell et al., 2001; Rickels et al., 2006), only about 5% (2 million) people were reported to wear protective helmets while bicycling in 2006. In this context, the German Neurosurgical Society (DGNC), during their annual meeting in 2007, demanded the introduction of compulsory helmet use for all bicyclists in Germany. Over the past two years, no major legislative changes concerning bicycle-helmet use took place in Germany or in any other European country. On the contrary, politicians and sports associations suggested improving education and increasing public awareness to convince the general public that wearing helmets is in everybody's interest.
Considering the 2007 demand of the German Neurosurgical Society, neurosurgeons seem to be particularly suited to evaluate whether neurotraumatological knowledge and experience, and therefore education, has influenced personal attitude and opinion over the past few years, leading to an increase in the use of helmets while bicycling. As the distribution of helmet users among neurosurgeons (NS), as well as their opinion and attitude in general, is not known, a survey was performed addressing major neurosurgical departments in Germany, Austria, and Switzerland. To get a further idea if there are major differences in attitude compared to the general public (PUB), a representative cohort of persons of the non-TBI-educated general population (PUB) were also interviewed.
Methods
Interviewees
From January to April 2009, 55 major neurosurgical departments (NS) in Germany, Austria, and Switzerland were contacted. Twenty anonymous questionnaires were mailed for voluntary completion to each of the 35 German University Centers, 11 Austrian University Clinics, and 9 Swiss University and Canton Hospitals. To act as a comparison, a “non-neurotrauma-educated” general population control group (PUB) was also interviewed. People visiting sports-equipment stores in Germany were asked to voluntarily complete the anonymous questionnaire. Only questionnaires answered by people aged 18 years or older were included.
Questionnaire
Participation in the survey was anonymous and voluntary. Thirteen closed questions were asked. Answers were predefined, mainly in ordinal categories. Neurosurgeons (NS) were asked about their experience in treating patients with brain injury after bicycle accidents, whereas the general population (PUB) was asked if they knew of people who had suffered from head injury while riding a bike. Everybody was asked whether they would favor compulsory use of helmets for bicyclists. In addition, topics such as age, gender, sports skills, duration of helmet possession, personal wearing habits, and, if applicable, the habits of their children were covered.
Statistical analysis
Data are presented as either percentage of persons or as median and range. Statistical analysis of the data was performed using SPSS 11.5 for Windows statistical software (SPSS, Inc., Chicago, IL). In comparisons, Pearson's chi-square test was used. Statistical significance was defined as p < 0.05.
Results
Of the 55 neurosurgical centers that were contacted, 46 centers (27 in Germany, 10 in Austria, and nine in Switzerland) answered, and 465 questionnaires (NS) were returned. In the general population group (PUB), 546 questionnaires were filled out.
The NS and PUB groups did not differ significantly concerning gender, age, and sports skills; 77.6% of the interviewed NS and 63.7% in the PUB group were male. In both groups, the majority of questioned people were aged 45 years or younger. A total of 94% of the NS group and 87% in the PUB group cycled. Both groups mainly rode their bikes in road traffic (60.3% NS and 54.8% PUB), while 7.5% (NS) and 15.9% (PUB) only did mountain biking. Approximately one third of NS (32.2%) and PUB (29.3%) used bikes for both transportation and mountain biking. Furthermore, more than 80% of each group were convinced that they retained control over their bicycles all the time.
A total of 48.1% of the neurosurgical population and 60.5% of the interviewed general population had children, of which more than 80% rode bikes.
Experience with traumatic brain injury
A total of 89.4% of all NS had treated patients with TBI after bicycle accidents. However, neurosurgeons from Germany and Switzerland were more experienced in treating patients with TBI after bicycle accidents than their colleagues from Austria (p = 0.01): the majority of German and Swiss neurosurgeons had treated more than five patients with TBI after bicycle accidents during the last year, whereas Austrian neurosurgeons typically claimed to have treated between one and five patients (p = 0.01). As expected, neurosurgeons had significantly more experience with TBI after bicycle accidents, and knew more cases of brain and head injury than the general population (p < 0.001). In comparison to the NS group, only 23.2% of the PUB group knew of somebody who had suffered from head trauma while bicycling.
Attitude to wearing helmets
Neurosurgeons did not differ significantly in their behavior and attitude to wearing and owning protective bicycle helmets from the general population: 49.7% of NS and 44.5% of PUB always wore their helmets while bicycling. One third of all bicyclists bought their helmet more than 5 years ago (32.4% NS; 34.2% PUB). Less than 4% bought a new helmet this season (3.8% NS; 0.6% PUB; p > 0.05). A total of 14.6% of NS and 10.1% of PUB plan to buy and use a helmet, while about 20% do not want to buy or wear a helmet in the future (18.8% NS; 20.9% PUB).
However, the fraction of bicyclists who refused to wear a bicycle helmet is significantly greater in the TBI-uneducated PUB group than among neurosurgeons (37.1% of NS vs. 45.8% of PUB; p = 0.036).
Furthermore, the use of bicycle helmets depended on the bicyclists' skills: mountain bikers started to use helmets earlier and for a longer time period (1–5 years) than those who used their bike mainly as a means of transportation in road traffic (p < 0.001; Fig. 1).

The percentage of neurosurgeons (NS) and of the general population (PUB) who always or never wear a helmet while bicycling in street traffic (street) or while mountain biking (mountain).*p < 0.001.
In the NS group, the use of helmets was neither correlated with the experience with TBI nor the number of patients treated after bicycle accidents. Independent of whether NS had formerly treated patients after bike accidents and had TBI experience, 37.1% of NS refused to wear a helmet, indicating, at least in a subgroup of NS, cognitive dissonance on protective helmet use. Furthermore, no country-dependent differences could be detected. However, in the PUB group, persons who had knowledge of people with injuries after bicycle accidents in their acquaintance used helmets more often than those who did not know anybody with TBI (p = 0.02). Furthermore, comparing “TBI-knowledge after bicycle accidents” with “TBI-missing-knowledge,” despite the NS or PUB group, revealed that those who had experience with TBI after bicycle trauma used helmets significantly more often (p < 0.001), while those who were inexperienced refused to wear a helmet in the future (p < 0.005; Fig. 2).
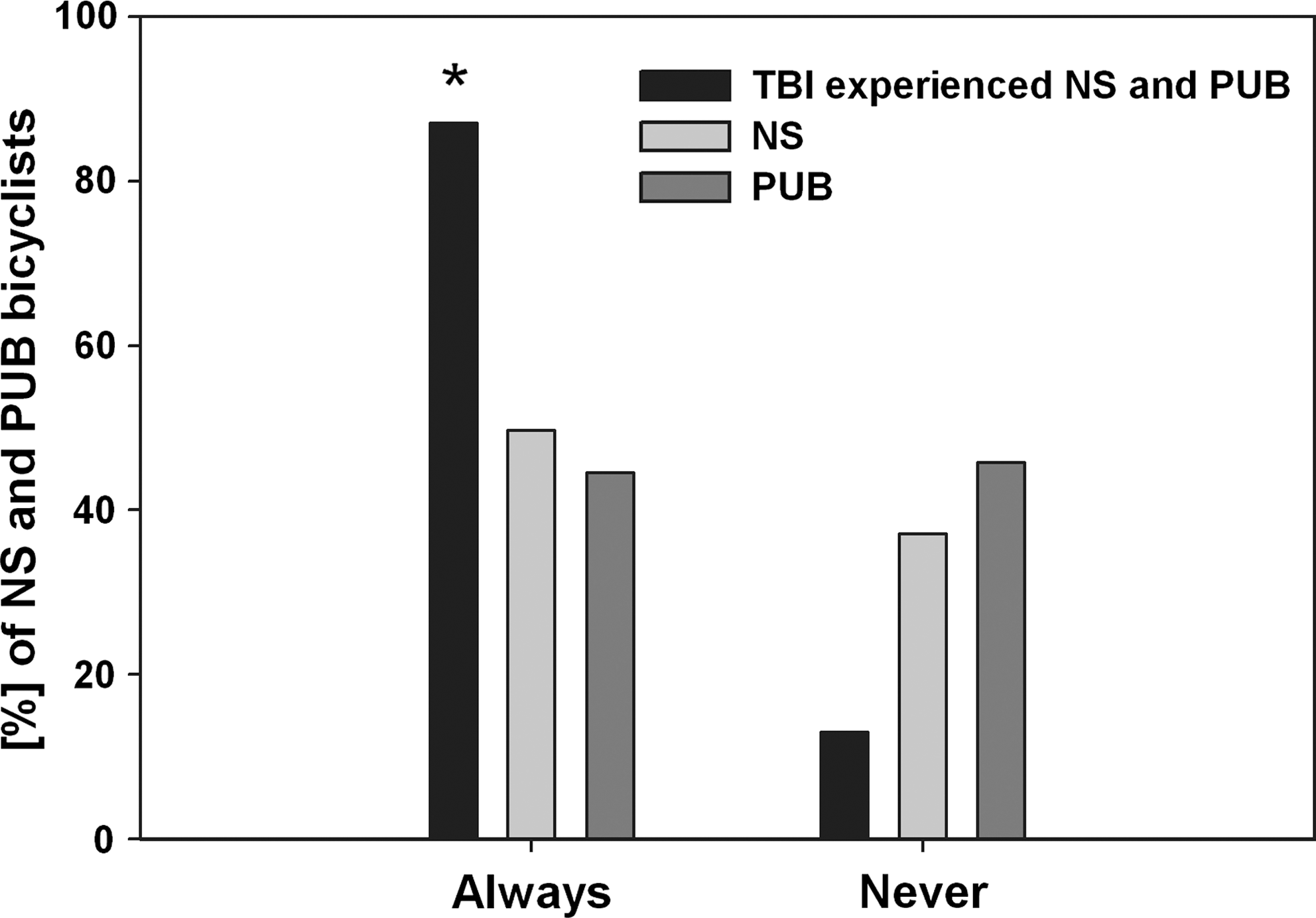
The percentage of neurosurgeons (NS) and of the general population (PUB) who always or never wear a helmet while bicycling compared to the attitude of all NS and PUB who have TBI education and experience. All those who are TBI educated wear helmets significantly (*) more often. *p < 0.005.
Children of the NS group wore helmets in 88% of cases while riding a bicycle, whereas PUB children used helmets in 60.9% (p < 0.001). The use of helmets by children of both groups was dependent on the attitude of their parents with respect to their own use of helmets, and was further correlated to their opinion on compulsory helmet use (p < 0.001). Therefore, most of the children who did not wear a helmet while bicycling had parents who did not wear helmets themselves.
Compulsory helmet use
Independent of their country of origin (Germany, Austria, or Switzerland) or the different use of bicycles (mountain biking vs. traffic), 63.8% of all NS and 50% of PUB favored compulsory use of helmets for bicycling. A total of 27.2% of NS and 35% of PUB rejected this option. The remaining interviewees of the NS and PUB group either did not respond to this question or had no opinion on this subject.
NS and PUB followed the same pattern: those who already used a helmet were more likely to vote for compulsory use than those who did not (p < 0.001). The opinion of whether the use of helmets should be made compulsory for bicyclists was influenced by TBI experience (p = 0.003). Furthermore, sports skills influenced the decision for compulsory helmet use in NS and PUB: those who practiced mountain biking favored compulsory use, while the majority of those who used their bicycles mainly as means of transportation in general traffic stood against compulsory helmet use (p = 0.001).
Discussion
Traumatic brain injury (TBI) is considered the primary cause of fatal injuries after bicycle accidents (Rickels et al., 2006; Rosenkranz and Sheridan, 2003; Silverberg et al., 1992; Sosin et al., 1996; Tsai et al., 2004). Therefore, accident prevention and protective measures are very important. Protective helmet use is reported to reduce the risk of brain injury after bicycle accidents by a factor of five (Attewell et al., 2001; Barkow, 1991; D.C. Thompson et al., 1996; R.S. Thompson et al., 1989). This is the reason why emergency response personnel and medical organizations, including the German Neurosurgical Society (DGNC), have advocated protective helmet use for bicyclists during recent years.
Neurosurgeons educated in brain-trauma treatment and with greater proven experience in TBI than the general population were scarcely affected by their TBI experience in their own decision to wear protective helmets: only one half of the neurosurgeons wore helmets while bicycling. In this, they did not differ from the general public. More than one third (37.1%) of NS show cognitive dissonant behavior by not wearing protective helmets while bicycling. A recent survey on ski patrollers showed similar signs of cognitive dissonance in their attitude with respect to the use of helmets. Even though they knew that helmets reduce serious injuries, most did not wear their helmets regularly (Evans et al., 2009). However, knowledge and information do influence helmet acceptance: comparing “TBI-knowledge after bicycle accidents” with “TBI-missing-knowledge,” irrespective of the NS or PUB group, revealed that those who had experience with TBI after bicycle trauma used helmets significantly more often, while those who were inexperienced refused to wear a helmet in the future. Furthermore, significantly fewer NS, who are more highly TBI-educated than PUB, refused momentarily to wear a helmet. This correlates well with other results. Children of NS used helmets significantly more than children of PUB. However, those PUB who did know persons in their acquaintance who had suffered from TBI did use protective helmets significantly more often or planned to wear one in the future than those who did not.
However, considering the cognitive dissonant behavior of one third of NS, education alone, when it is based solely on the appeal to reason, might not lead to complete acceptance and use of helmets. Consequently, education on TBI, as favored by some groups, seems to be of significant value in increasing the acceptance of helmets, but it might need to be complemented with other factors such as, for example, emotional elements.
Overestimation of one's ability and a deceptive sense of security are other factors preventing full helmet acceptance while bicycling. In our survey, both NS and PUB tended to overestimate their own capabilities while bicycling. When asked if they believed they have permanent control over their bikes—a question that can truly only be answered with “NO”—more than 80% of the bicycling NS and PUB answered “YES.” Especially surprising was the fact that this was also true for those who favored mountain biking, because this subgroup seemed to be more risk aware, favored compulsory helmet use, and wore helmets earlier and for a longer time period than those who used their bikes mainly as a means of transportation in road traffic.
Some members of both groups commented on their refusal to wear a helmet when they returned the questionnaire. The most frequent comments corresponded to those reported by Finnoff et al. (2001): “uncomfortable,” “annoying,” “it's hot,” “don't need it,” and “don't own one.” Arguments in favor of wearing helmets were: “increased safety,” as well as “our children have worn helmets for years because we enforced it—now we also wear a helmet as a role model.” The first three arguments show that there is further need for technical improvement of helmets.
Parents of both the NS and PUB groups reported that their children wore protective helmets significantly more often (80–90%) than they did themselves. However, parental perceptions about the use of helmets by their children may not accurately reflect the truth. Ehrlich et al. (2001) found out that parents, influenced by their expectations of the use of bicycle helmets by their children, tend to overestimate compliance. In our study, the incidence of helmet use in children correlated with two factors: (a) the actual helmet use of their parents and (b) the disposition of the parents to make helmet use compulsory. The first factor shows the effectiveness of role models for increasing the use of protective equipment, which is based on emotion and a well-known and important fact (Bolen et al., 1998; Dannenberg et al., 1993). Therefore, role models employed in campaigns might help to improve helmet use with carefully chosen personalities. The second factor relates more to parental authority than to their influence as role models, and is therefore connected to the problem of compulsory use.
The German Neurosurgical Society demanded compulsory use of protective helmets for bicyclists, which has to be controlled and enforced with legal measures. If not accepted by a great majority of the population, this will be difficult, personnel-intensive, and therefore costly. Furthermore, legislation will hardly act if the majority of their voters oppose such a move. Therefore, prior to the decision to make helmet use compulsory, one should evaluate the acceptance of compulsory helmet use, and the implementation has to be accompanied by campaigns using all available means to increase acceptance. A Cochrane meta-analysis on bicycle-helmet legislation effectiveness showed that making helmet use compulsory effectively increased the incidence of helmet use and decreased head-injury rates in the populations where it was implemented. However, none of the included studies measured actual bicycle use, so it was not possible to evaluate the claim that fewer individuals were cycling because of the implementation of the helmet laws (Macpherson and Spinks, 2008).
Our survey shows that compulsory helmet use was favored by those who themselves wore helmets. TBI experience increased the support, which is surprising, since no such influence could be found on their own helmet use. It seems that those who are experienced with TBI but do not use protective helmets are to some extend aware of their cognitive dissonant behavior and feel that some outside pressure is needed to change it. A higher percentage of mountain bikers wear helmets and are in favor of compulsory use than bicycling participants of general road traffic. A look on German roads shows that most bikers cycling for exercise and fun wear sports apparel with fashionable helmets similar to professional bikers. They may be more risk aware but clearly they want to be lookers. This is an important hint to how helmet wear could be promoted and the acceptance of compulsory use improved. But it will only be really successful if it is transferred from the sport bicyclers to those who use their bikes merely for transportation.
Conclusions
Neurosurgeons present a well-educated group in neurotraumatology. Half of them wear helmets, while one third shows cognitive dissonance between their knowledge of brain trauma and their attitude to wearing protective helmets. Despite some cognitive dissonant behavior, knowledge and education do play a significant role in the decision to wear bicycle helmets. However, rational education alone might not always be sufficient for future helmet promotion. It has to be complemented with more emotional approaches. Making helmet wear a matter of fashion and part of the apparel bikers like to wear, even while participating in general traffic, is another promising and important approach.
Compulsory use of bicycle helmets, as favored by the German Neurosurgical Society and supported by more than half of the questioned neurosurgeons and those of the general population group, has to be implemented, controlled, and enforced with legal measures. If it is not accepted by a great majority of the population, this will be difficult, personnel-intensive, and expensive. Our results show that neurosurgeons and the general public are split in half on this matter. Therefore, increasing the rate of bicycle-helmet users has to be accompanied by continuing campaigns using all available means to increase acceptance, which have to be based on approaches that have been outlined above.
Footnotes
Acknowledgment
We wish to thank the families of the first and second authors for their enthusiasm and help in distributing questionnaires. Furthermore, we would like to thank everybody who voluntarily took the time to fill out the questionnaire.
Author Disclosure Statement
No competing financial interests exist.