
Abstract
Adult outcome from childhood brain injury is largely unknown, and health professionals have minimal evidence available to inform families about their child's long-term prognosis. This study aimed to investigate long-term outcomes in this group, focusing on quality of life (QOL) and the injury, developmental, and environmental factors that influence this domain, using a retrospective and cross-sectional design. The sample was ascertained via medical record audit at the Royal Children's Hospital, Melbourne, Australia, and included 130 adult survivors of child traumatic brain injury (TBI) (84 men). Participants were 18–42 years at evaluation (mean = 23.2, SD = 3.3) and completed questionnaires regarding QOL and educational, employment, and psychological status. Analysis of variance, chi-square, and regression were employed to assess group differences and predictors of outcome. While most adult survivors of childhood TBI rated their QOL as intact, 17% of the sample reported poor QOL. Poor QOL was more likely with low levels of perceived independence, severe TBI, younger age at injury, failure to complete high school, and psychological problems. In conclusion, QOL in adult survivors of childhood TBI is better than expected and closely associated with both injury and noninjury factors, most consistently with the individual's perception of their level of independence.
Introduction
T
It is likely that, when such injuries occur during childhood, normal developmental processes will be disrupted, exacerbating the primary consequences of insult. If this is the case, then adult survivors of childhood TBI will suffer problems across a wide range of domains, including cognitive, academic, vocational, social, and emotional, potentially leading to poor QOL and family and community burden. Only a handful of studies have followed child survivors into adulthood. These show somewhat conflicting results, possibly due to inherent methodological problems of longitudinal research, including sample attrition and bias and changes in diagnostic and treatment approaches over time. Klonoff and colleagues (1993) conducted telephone interviews with survivors (n = 159) 21 years post-injury and identified psychological and family problems as well as poor educational and vocational attainment, with an association between injury severity and presence of difficulties. Using similar methods (n = 20), Cattelani and associates (1998) reported that physical and cognitive problems declined as children reached adulthood, while social maladjustment and poor QOL remained. In contrast, positive outcomes have been reported by others (Hessen et al., 2007; McKinlay et al., 2002; Vignolo, 1980), although these studies focused on mild TBI or failed to consider injury severity.
Attempts to better explain physical and cognitive outcomes following TBI have identified several injury-based and demographic factors: injury severity, injury age, premorbid characteristics of the child, socioeconomic status (SES), and family function (Anderson et al., 2005; Rivara et al., 1993; Yeates et al., 2004). It is likely that these factors will also influence psychosocial outcomes, although the relative weightings may be different (Hoofien et al., 2002; Kieslich et al., 2001; Nybo and Koskiniemi, 1999). In support of this assumption, Muscara and colleagues (2008) compared survivors of mild and moderate-severe TBI sustained in childhood at 10 years post-injury and found poorer adaptive and social skills associated with more severe injury. Koskiniemi and co-workers (1995) examined young adults with TBI prior to age 7 and found strong associations between employment status and both brain pathology and medical disability. Younger age at injury, emotional instability, and personality disturbance were also implicated. Donders and Warschausky (2007) compared young people injured in childhood and adolescence and demonstrated poorer psychosocial outcome for earlier injuries even after 10 years. Exploring demographic influences on long-term outcome, Catroppa and associates (2008) identified pre-injury child function as critical for outcome at 5 years post-TBI, while social disadvantage has also been linked to poorer function after child TBI (Anderson et al., 2006; Taylor et al., 2002).
In summary, there is a growing body of literature describing long-term outcomes following childhood TBI, suggesting that adult survivors have elevated risk of physical, cognitive, and psychosocial impairments that are likely to impact negatively on day-to-day function and, as a result, on QOL. While several studies have examined cognitive and functional domains, few have considered QOL and none have explored the factors contributing to good or poor QOL. The aim of the present study was to recruit a large, representative group of survivors of childhood TBI and survey their current QOL. Using these data, we derived three groups (poor, borderline, and intact QOL) and then examined the characteristics of these QOL groups with respect to injury and demographic variables, academic and vocational outcomes, and psychological status. Based on previous literature, we predicted that poorer QOL would be associated with more severe TBI, lower educational and vocational status, and elevated risk of psychosocial problems. Further, we expected that age at injury, SES, educational achievement, and current functional levels would play a significant role in predicting QOL.
Materials and Method
Participants
Recruitment was conducted via medical record review, with eligibility defined as admission to the neurosurgical ward at the Royal Children's Hospital, Melbourne, Australia, with a diagnosis of TBI. Inclusion criteria were (i) aged 0–16 years at the time of TBI; (ii) diagnosis of TBI; (iii) medical records sufficient to determine injury severity; (iv) older than 18 years at the time of assessment; (v) no pre-injury history of neurological, developmental, or psychiatric disorder; (vi) accidental injury; and (vii) English speaking.
Medical record audit identified 300 cases meeting inclusion criteria. Fifty-three (17.7%) individuals could not be located via mail, electoral roles, or medical databases. Two potential participants had died since their injuries, 52 (26.7%) did not respond and 35 (11.7%) declined to participate due to work commitments, distance, or lack of interest. Comparing participants and nonparticipants, no differences were found for SES, sex, accident type, neurosurgical interventions, or days of hospital admission.
The resultant sample for the study comprised 130 (53% of located cases) adolescents and young adults (84 men). Table 1 provides a summary of the demographic characteristics of the resultant sample. Participants were aged between 18 and 42 years (mean = 23.2, SD = 3.3) at time of recruitment, had sustained a TBI within the age range of 0–16 years (mean = 10.0, SD = 2.8). Assessment was conducted on average 12.3 years post-injury (SD = 5.2, range 3–41). Individuals who had sustained mild, moderate, and severe TBI were included, and concussive injuries were excluded.
QOL, quality of life; MVA, motor vehicle accident; ns, not significant.
Severity of TBI was determined from medical records, using the Glasgow Coma Score (GCS; Teasdale and Jennett, 1974): lowest in 24 hours post-TBI, length of post-traumatic amnesia (PTA), length of coma, radiological results (computed tomography [CT], magnetic resonance imaging [MRI], X-ray), presence of neurological signs: (i) mild TBI = GCS: 13–15, period of altered consciousness/coma <1 hour, normal CT/MRI, no neurological signs; (ii) moderate TBI = GCS: 9–12, period of altered consciousness/coma 1–24 hours and/or abnormalities on CT/MRI scan, and/or presence of neurological signs; (iii) severe TBI = GCS < 9, loss of consciousness >24 hours, abnormalities on CT/MRI, and/or presence of neurological signs. Using these definitions, 63 (48.5%) participants had mild TBI, 29 (22.3%) moderate TBI, and 38 (29.2%) severe TBI. Interrater reliability was examined for these groupings, using 10% of eligible cases, and found to be high (0.95).
Measures
Predictors/risk factors
Injury severity: categorized as mild, moderate, or severe TBI as described in the previous section.
Age at injury: recorded from medical records.
Psychosocial factors: SES at time of assessment was coded according to Daniel (1983) based on current highest occupational prestige of the participant's parents, as an index of SES level since TBI. This measure provides a 7-point rating with higher scores reflecting lower SES. These ratings were then categorized into high (<4) or low (≥4) SES.
Pre-injury function: assessed via a 12-item questionnaire completed by the parent. Questionnaire items included presence of diagnosed medical, developmental, or psychiatric problems pre-injury and at the time of assessment, involvement in rehabilitation since injury, and current level of independence.
Outcome
Functional outcome: Participants and their parents completed a 30-item questionnaire which tapped into functional skills post-TBI including educational level, employment status, psychological function, and current relationships. Involvement in rehabilitation and other interventions were also assessed.
Quality of life: Participants completed the Sydney Psychosocial Reintegration Scale: Form P (SPRS; Tate et al., 1999), adapted for childhood TBI, which incorporates three scales: work and leisure, relationships, and living skills. Each scale includes four items that require the respondent to provide subjective ratings of their level of satisfaction with respect to particular skills and abilities (e.g., work and study, independence, social skills) post-injury and how they compare with normal development. Responses were recorded on a 0 (extremely affected) to 6 (not at all affected) scale, with a maximum score of 24 per scale and a maximum total score of 72. Total SPRS scores were employed to derive QOL classifications, as described by Tate and colleagues (1999): 1) 0–47 = poor QOL; 2) 48–64 = borderline; and 3) 65–72 = intact QOL. For each of the three subscales scores were similarly categorized: 1) 0–15 = poor QOL; 2) 16–21 = borderline QOL; and 3) 22–24 = intact QOL. The SPRS has high internal consistency (α = 0.90), high agreement between raters (0.95), and high stability over a 1-month period (0.90). Measures purported to assess QOL often lack established validity and have been argued to tap skills other than QOL (e.g., participation, integration). Of note, preliminary evidence has been documented for both convergent and discriminant construct validity, and studies have supported the SPRS as a measure of QOL rather than participation, reporting high correlations with the psychosocial scale of the Sickness Impact Profile but low association with Community Integration Scale (Hodgkinson et al., 1999).
Procedure
This study was approved by the Human Ethics Committee of the Royal Children's Hospital, Melbourne, Australia. Following medical record audit, all identified adolescents or young adults and their families were contacted by letter and invited to participate in the study. Participants were given the option of returning an “opt out” response within 2 weeks or awaiting a phone call from a member of the research team. When negative responses were returned, no further contact was made. When no response was received, researchers contacted potential participants by telephone to provide further study details and seek their consent for inclusion in the study. For potential participants not located via this method, admission information was used to locate current addresses via the electoral role. For those individuals that could not be located, injury and psychosocial data were recorded for analysis in order to address possible sample bias. Once consent was obtained, participants and their parents or guardians were sent a package of questionnaires for completion and return to the research team. When questionnaires were not returned within 2 months a member of the research team then followed up with all consenting participants and parents with a telephone call to remind them of the study and to offer further assistance for completion of questionnaires.
Data analysis
Data analyses were conducted using SPSS 17.0. for Windows. A small amount of questionnaire data was missing for a small number of participants. In these instances missing data were not included in analyses. Precise sample sizes for each measure are given in relevant tables.
To explore QOL group differences with respect to injury and demographic characteristics and functional outcomes either ANOVA or chi-square analyses were conducted. To explore the impact of injury severity on long-term quality of life, ANOVA was employed using mean SPRS scores, and then followed-up with chi-square analyses across severity groups and QOL categories. Potential predictors (severity group, age at injury, SES, employment, psychological and educational status, independence level) were further explored with regression analyses.
Results
Demographic, injury, and functional characteristics
As illustrated in Table 1, there were no differences across QOL groups for sex, age at injury, SES, or frequency of pre-injury educational or psychological problems. For age at assessment, the poor QOL group was significantly older than the other two groups. Injury data for the group are also presented in Table 1, with expected group differences detected for injury measures including days in hospital, multiple trauma, and access to rehabilitation or intervention post-injury. Motor vehicle accidents were commonly related to poorer QOL, while sports injuries and falls/blows were more frequent in borderline and intact QOL groups.
Functional status questionnaire (participants and parents)
Table 2 provides data on interventions and functional outcomes, based on parent responses. Parent ratings were chosen here based on analysis of missing data and feedback from participants that indicated generally poor recall of such information, much of which fell many years prior to study. Overall, 53 parents (40.8%) reported that their child received intervention or rehabilitation post-injury, with access to rehabilitation significantly related to poorer QOL. Further, 33 (25.4%) of the young adults continued to access rehabilitation services in the 5 years prior to the study, with highest representation in the poor (42.1%) and borderline (39.3%) QOL categories. Significant group differences were detected with regard to need for additional educational support post-TBI, level of education obtained, and current occupational level. In all instances, poorer QOL was related to more difficulties.
QOL, quality of life;
While pre-injury psychological problems were rarely documented, post-TBI rates of psychiatric problems and associated interventions were elevated in the poor and borderline QOL groups compared to those with intact QOL. Less severe “adjustment problems,” were also more commonly linked with poor QOL, based on both participant and parent ratings. Of note, parents were much more likely to report that the young person experienced these problems (33%) than were participants (3%).
Predictors of adult QOL
ANOVA was conducted across severity groups for the subscale scores from the modified SPRS: work and leisure, relationships, and living skills (Table 3). A significant injury effect was identified for total SPRS score (F 2,129 = 9.73, p < 0.001), and for all subscales (work and leisure: F 2,129 = 14.69, p < 0.001; relationships: F 2,129 = 3.72, p = 0.03; and living skills: F 2,129 = 5.55, p = 0.005). Post hoc pairwise comparisons indicated that the severe TBI group recorded lower QOL scores than the mild TBI group, and in all but the relationships subscale they also had lower QOL than those with moderate TBI. Frequencies of participants falling into each of the three QOL categories for each severity level are illustrated in Figure 1, with significant differences identified in distributions across all four measures [work and leisure: χ2 (6, N = 130) = 26.29, p < 0.001; relationships: χ2 (6, N = 130) = 11.68, p = 0.04; living skills: χ2 (6, N = 130) = 17.71, p = 0.004; and total: χ2 (6, N = 130) = 17.74, p = 0.001], and with more severe injury and poorer QOL consistently linked.
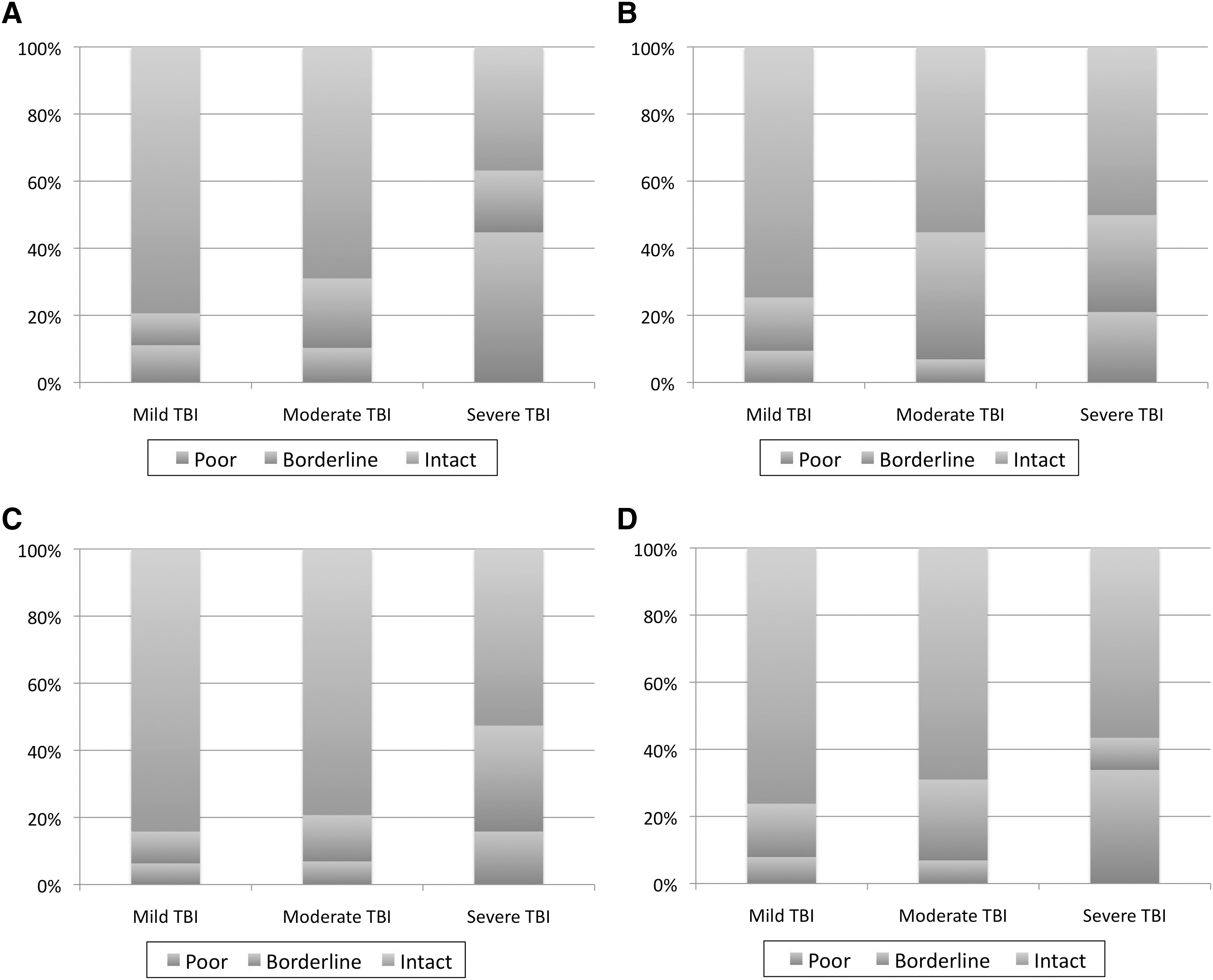
Proportion of young survivors of TBI with intact, poor, and borderline quality of life (QOL). (
p < 0.05; **p < 0.01; ***p < 0.001.
SPRS, Sydney Psychosocial Reintegration Scale; TBI, traumatic brain injury.
Regression analyses identified several additional factors which contributed to current QOL. Findings are detailed in Table 4. Overall, participants' perceived independence was the best predictor of QOL, contributing significantly to all SPRS measures. Educational level achieved was also important for all domains but living skills, while age at injury predicted relationships and living skills. Injury severity and current psychological status were less influential, only contributing to the work and leisure domain, while SES level and employment status were not linked to any QOL variables. The proportion of variance explained by regression models was just above 50% for work and leisure and total scores, and around 40% for relationships and living skills.
ns, not significant.
Discussion
The aim of this study was to investigate QOL in adult survivors of childhood TBI and to explore factors contributing to long-term QOL in this group. Previous research attempting to determine the consequences of early TBI that persist into adulthood has been plagued by methodological weaknesses (sample attrition and bias, evolving injury descriptors), and we attempted to reduce these, while acknowledging that some methodological problems are unavoidable when conducting such long-term investigations. Our sample was representative of the hospital's admissions for TBI during the period of recruitment, in terms of key injury and noninjury factors (length of hospital stay, accident type, sex, SES). We hypothesized that, as well as the established influence of injury-related parameters (severity, injury age), noninjury indices, such as SES, academic success, employment status, and psychological factors would play a significant role in determining long-term QOL, as has been documented by others at earlier stages post-injury (Anderson et al., 2005; Yeates et al., 1997). Our findings provided partial support for these predictions, with group differences for QOL identified for injury severity factors, as well as educational attainment, and employment and psychological status. When considering relative contributions to QOL, levels of both educational attainment and independence were consistently important, with injury severity, age at injury, and psychological status relevant for individual QOL domains. Lastly, SES and employment status were unrelated to any areas of QOL.
Descriptive data provided by participants and their parents demonstrated that approximately three quarters of survivors had accessed no additional educational support during their school years, with a similar proportion completing high school, and two fifths continuing on to higher education. One third of the sample was unemployed at the time of the study, and approximately one half had either skilled or professional employment. Not surprisingly, those with lower educational and vocational attainment were more highly represented in the poor and borderline QOL categories. Psychological problems and post-injury intervention rates were low and around the level suggested by population statistics (Australian Bureau of Statistics, 2006), although once again, more problems were noted in individuals with poor or borderline QOL. Access to rehabilitation was also related to QOL, with individuals with poor QOL more likely to have been involved in some form of treatment post-injury. This association most likely reflects the more significant residual problems for this group of survivors, rather than suggesting that intervention leads to poorer QOL.
One particularly interesting finding was observed for psychological adjustment, measured via the functional outcomes questionnaire, for which both participant and parent ratings were available. On this measure, parent ratings identified problems (28.5%) 10 times more commonly than participants (2.4%). Further, parent ratings were not associated with QOL scores. Of note, none of the study participants were involved in ongoing litigation associated with their injuries, which might impact parent ratings. These results are consistent with research describing limited insight post-TBI (Draper et al., 2007), which might lead to an interpretation that young adult survivors are largely unaware of their functional deficiencies. However, while this argument might explain the discrepancies between ratings for participants with severe TBI, who are likely to have sustained serious brain damage commonly associated with poor insight, it fails to account for elevated rates associated with moderate and more specifically mild TBI where brain damage is, by definition, less serious. An alternative argument is that parents have developed a particular perception of the level of function of these young people, which has been influenced by early injury and possibly acute and subacute functional problems, or by their own psychological adjustment post-injury. Further research is required to explore these possibilities more fully.
Examination of the scores for the total group under study demonstrated that almost two thirds of adult survivors did not report any problems with their QOL, and only 15% rated themselves as having poor QOL. As illustrated in Figure 1, using total SPRS results, individuals with a history of severe TBI were roughly five times as likely to rate themselves as having poor QOL than those with mild and moderate TBI. While poor and borderline QOL was present within all severity levels and across all QOL domains, rates were consistently higher for the severe TBI group, with mild and moderate TBI associated with similar outcomes. Poorest results were found for work and leisure (ability, participation, organization), with almost half of those in the severe TBI group reporting poor outcomes, compared to 20% for relationships and 15% for living skills. Satisfaction with work and leisure was also marginally lower than for other domains for mild and moderate TBI groups. Living skills (e.g., hygiene, dressing, transport, living context) appeared less vulnerable to early TBI, with relatively few young adults with TBI noting difficulties in this domain, even following severe TBI. These findings suggest that work and leisure activities are particularly impacted in the long term post-TBI, and this interpretation is supported by findings of reduced educational attainment and employment status in the current sample, as well as by previous literature (Anderson et al., 2008; Kinsella et al., 1995). In contrast, routine living skills appear relatively robust, with few participants noting significant residual problems with these activities, suggesting that survivors have few difficulties coping independently with basic personal daily activities.
The second prediction of the study was that both injury and noninjury factors would contribute to long-term QOL. This prediction was only partially supported, with different factors contributing to specific QOL domains. First, and as noted previously, injury severity was a key predictor of satisfaction with work and leisure, with more severe injury related to poorer scores. In addition, lower perceived level of independence, lower educational level achieved, and psychological problems all contributed significantly. For relationships, once again, perceived level of independence and educational level were influential, with younger age at insult associated with poorer outcome in this domain. Living skills were predicted by age at injury and perceived level of independence, with younger age and less independence linked to less satisfaction. The major influences on overall QOL scores were educational level and independence level. Interestingly, and contrary to predictions, SES was not significant in any of the regression models and neither was employment status. This pattern of findings is in keeping with results from studies looking at outcomes closer to time of injury, which suggest that injury severity is specifically related to “cognitive” outcomes, which are likely to be best captured by the work and leisure domain of the SPRS, while psychosocial outcomes are more closely linked to environment (Anderson et al., 2005, 2006,). Further, while age at injury was not a consistent predictor, it was linked to both living skills and relationships, supporting a link between developmental level at time of injury and social and psychological function (Donders and Warschausky, 2007).
A number of study limitations need to be taken into consideration when interpreting these findings. First, participation rates (56%), while higher than reported in previous studies, were less than optimal, raising concerns about sample bias. It may be argued that the sample is biased with a likelihood of greater participation by higher functioning families; however, this was not our subjective impression, at least for those families with whom we had contact. The availability of injury data and demographic information for all potential participants and the subsequent finding that participating and nonparticipating groups did nor differ on these variables, which included SES at time of injury, provide some reassurance on this issue. Second, many of the individuals under study suffered their injuries well before the introduction of standardized injury indices such as GCS and PTA measures. While we believe that we were able to reliably classify participants into injury groups, as evidenced by high interrater reliability, such an approach is not optimal, and may introduce unreliability into severity ratings. Third, the QOL measure employed was designed as a TBI-specific measure. The generalizability of findings must be considered in the light of this limitation. Finally, much of the data collected were based on self-ratings. Given concerns about lack of insight associated with serious injury, it may be that this impacted our results. The differences between parent and participant ratings for presence of adjustment problems would support this possibility, with parents more than five times as likely to identify adjustment problems than the young adult survivors. Of note, however, in the domain of QOL, it could be argued that, regardless of insight, it is the survivors' perceptions of personal satisfaction that are of most relevance.
In conclusion, while reduced QOL was found to persist into adulthood following child TBI for some individuals, in general survivors reported intact QOL or only mild dissatisfaction with life skills and style, suggesting better outcomes than might be predicted from studies assessing early functional recovery. However, specific problems were identified in subgroups of TBI survivors and in the presence of particular risk and resilience factors, providing some guidance for clinicians with respect to resource allocation after childhood TBI. Firstly, most problems were identified in the areas of work and leisure activities (20% of sample), in which injury severity was a strong predictor of outcome, with educational performance and early psychological adjustment also influential. Relationships were also identified as an area of concern in around 10% of participants, with younger injury age and poorer educational attainment important for this domain. These results indicate that both educational and psychological interventions should be considered in the post-injury period, especially for children with more severe insults occurring in early childhood. Living skills were surprisingly robust across the sample, with few participants indicating significant problems with routine personal daily living skills. Where identified, problems in this domain were linked to younger age at injury. However, by far the most important predictor of QOL, across all domains was the survivors' perception of their own level of independence. This finding suggests that, once acute rehabilitation is complete, health professionals and families need to focus their care and treatment on maximizing the child's independence and encourage the young person's adjustment to their new status, participation in developmentally appropriate activities, and personal responsibility.
Footnotes
Acknowledgments
The authors acknowledge the survivors and their families who contributed their time to this study and Katherine Lee for her assistance with statistical analyses.
Author Disclosure Statement
No competing financial interests exist.