
Abstract
This study was designed to evaluate the potential benefits of hyperbaric oxygen (HBO) in the treatment of traumatic brain injury (TBI). The right cerebral cortex of rats was injured by the impact of a 20-g object dropped from a predetermined height. The rats received HBO treatment at 3 ATA for 60 min after TBI. Neurological behavior score, brain water content, neuronal loss in the hippocampus, and cell apoptosis in brain tissue surrounding the primary injury site were examined to determine brain damage severity. Three and six hours after TBI, HBO-treated rats displayed a significant reduction in brain damage. However, by 12 h after TBI, the efficacy of HBO treatment was considerably attenuated. Furthermore, at 24, 48, and 72 h after TBI, the HBO treatment did not show any notable effects. In contrast, multiple HBO treatments (three or five times in all), even when started 48 h after TBI, remarkably reduced neurology deficit scores and the loss of neuronal numbers in the hippocampus. Although multiple treatments started at 48 h significantly improved neurological behaviors and reduced brain injury, the overall beneficial effects were substantially weaker than those seen after a single treatment at 6 h. These results suggest that: (1) HBO treatment could alleviate brain damage after TBI; (2) a single treatment with HBO has a time limitation of 12 h post-TBI; and (3) multiple HBO treatments have the possibility to extend the post-TBI delivery time window. Therefore, our results clearly suggest the validity of HBO therapy for the treatment of TBI.
Introduction
T
Usually, hyperbaric oxygen (HBO) therapy is achieved by exposing a patient to barometric pressures higher than ambient pressure (1 atmosphere absolute [1 ATA]), while they breathe 100% oxygen. Exposure to HBO dramatically increases the oxygen content of the blood via physical dissolution of oxygen (Calvert et al., 2007; Daugherty et al., 2004; Nemoto and Betterman, 2007). In mammals, the increased blood oxygen levels seen during HBO treatment are released passively, and can penetrate into ischemic areas more deeply than under normobaric conditions (Calvert et al., 2007; Nemoto and Betterman, 2007). Therefore, HBO may be a very useful therapy for TBI patients. However, a recent literature review does not support the use of hyperbaric oxygen for TBI and stroke (Oppel, 2003), and the value of HBO treatment in TBI remains controversial (Rockswold et al., 2007). There remain many questions about the use of HBO therapy in TBI, such as the most effective therapeutic time window for the application of HBO, the optimal dosing regimen, guidelines that should be followed for repeated exposures, and the safety of re-exposure (Daugherty et al., 2004; Nemoto and Betterman, 2007). In the present study, we investigated the time window and the therapeutic effects of repeated HBO treatments for TBI. We also evaluated the value of systemic delivery of HBO treatment.
Pathologically, TBI shares several similarities with ischemic stroke. Both of them are characterized by central necrosis and a peri-lesional penumbra, where both excitotoxic and ischemic events eventually lead to delayed neuronal death (Leker and Shohami, 2002). In TBI, apoptosis commonly occurs in the peri-lesional area as a result of secondary brain insults (Chen et al., 2008; Conti et al., 1998). Several previous studies have demonstrated that HBO can prevent apoptotic death of neuronal cells in cerebral ischemic-anoxic and contusion insults (Calvert et al., 2003; Palzur et al., 2004). Nevertheless, the effects of HBO on neural apoptosis after TBI have not been fully elucidated. Therefore in this study we also examined apoptosis in brain tissue surrounding the primary injury site to explore the potential value of HBO in reducing secondary traumatic brain damage.
Methods
Animals
Male Sprague-Dawley rats (250–280 g body weight) were provided by the Experimental Animal Center of Nantong University, Nantong, China. The rats were housed in a temperature- and humidity-controlled animal facility with a 12-h light/dark cycle. All procedures used in this study were in accordance with our institutional guidelines, which comply with internationally accepted humane standards. The animal study groups are shown in Table 1.
HBO, hyperbaric oxygen; RT-PCR, reverse-transcriptase polymerase chain reaction; TUNEL, terminal deoxynucleotidyl transferase-mediated dUTP nick end labeling; TBI, traumatic brain injury; ATA, absolute atmosphere.
Traumatic brain injury
The rats were anesthetized using 2 mL enflurane in an ether jar, and maintained with 10% chloral hydrate (400 mg kg–1 IP). The head of the animal was fixed in a stereotactic frame. A right parietal craniotomy (3.5 mm posterior and 2.5 mm lateral to the bregma, diameter 5 mm) was performed with a drill under aseptic conditions. Following Feeney's weight-drop model (Feeney et al., 1981), a standardized parietal contusion was produced by letting a steel rod weighing 20 g with a flat end and diameter of 4.5 mm drop onto a piston resting on the dura from a height of 30 cm. The piston was allowed to compress the brain tissue to a depth of 2.5 mm. Heart rate, arterial blood pressure, and rectal temperature were monitored. The animal's temperature was maintained at 37 ± 0.5°C throughout the experiment. Sham-operated rats were anesthetized and only the right parietal craniotomy was carried out. All animals were randomly distributed in the study groups.
Hyperbaric oxygen treatment
All treatments were begun at 9:00
Neurological evaluation
All neurological evaluations were carried out by a researcher blinded to study group. The beam-balancing test and prehensile traction test were used for neurological scoring as proposed by Dixon and colleagues (1987) and Hall and associates (1988). Both tests were scored according to several grades. A higher score represents more severe neurological deficit, ranging from a minimum score of 0 for near-normal rats, to a maximum score of 14, indicating severe impairment. Prior to TBI, all of the animals were trained, and rats with abnormal neurological function were eliminated.
The beam-balancing test consisted of placing the rat on a narrow wooden beam (1.5 cm wide), and noting how long (up to 60 sec) the animal was able to maintain its balance: 0 = the rat walks easily and turns around freely; 1 = the rat maintains a stable posture for 60 sec; 2 = the rat hugs the beam or hooks it with its limb before 60 sec elapsed; and 3 = the rat falls off of the beam.
The prehensile traction test was conducted by placing the rat on a 120-cm-long taut string that was suspended between two upright metal bars 80 cm above a padded table, and noting how long (up to 60 sec) the animal could remain on the string: 0 = the rat grasps the string tightly and climbs up quickly; 1 = the rat can hold onto the string with its rear limbs and try to climb; 2 = the rat can remain on the string but without using its rear limbs; and 3 = the rat falls off of the string.
Gravimetric analysis of brain water content
The rats were anesthetized with 10% chloral hydrate (400 mg/kg IP) and killed by decapitation. The brains were immediately removed and separated into the left and right hemispheres. After the determination of the wet weight of each hemisphere, the tissue was dried for 72 h at 100°C, followed by measurement of the dry weight. The percentage brain water content was calculated as 100 × (wet weight – dry weight)/wet weight.
Reverse-transcriptase polymerase chain reaction amplification of mRNA
The rats were sacrificed 24 h after TBI, and the brains were immediately removed. The brain tissue surrounding the cortical contusion site was dissected (see Fig. 1A). The samples were frozen and stored at −80°C (Heto Ultra Freeze; Thermo Scientific, Milford, MA). Total RNA was extracted from brain tissue using Trizol reagent (Invitrogen, Carlsbad, CA), and quantified by optical density readings (GeneQuant; Amersham Biosciences, Buckinghamshire, U.K.). For RT-PCR, 2 μg of total RNA was reverse transcribed by using RevertAid™ First Strand cDNA Synthesis Kits (MBI Fermentas, Burlington, Ontario, Canada).
Comparison of the effects of three kinds of therapy. (
The sense and antisense primers used in this study are shown in Table 2 (the primers were purchased from Shengong Inc., Shanghai, China). The number of PCR cycles for each set of primers was optimized during the exponential phase of PCR by titration of visible product on GelStar-stained 1.5% agarose gels containing ethidium bromide. Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) and β-actin were used as controls. Quantification of amplified product was performed by gel densitometry. The band intensities were determined using a computer image analysis system (Quantity One; Bio-Rad Laboratories, Hercules, CA), and are expressed as the ratio to GAPDH or β-actin.
GAPDH, glyceraldehyde-3-phosphate dehydrogenase.
Nissl staining
The animals were killed with deep anesthesia by perfusion through the left ventricle with 200 mL of ice-cold phosphate-buffered saline (PBS; 0.1 mol/L), followed by 400 mL of 4% paraformaldehyde in 0.1 mol/L PBS (pH 7.4). The brains were then removed and post-fixed for 24 h in the same fixative. The post-fixed brains were protected in 30% sucrose in PBS. The brain tissue was coronally sectioned 20-μm thick with a cryostat (CM1900; Leica, Bensheim, Germany). Sections between 3 and 4.5 mm posterior to the bregma were selected. The free-floating sections were mounted onto slides and processed through different baths in the following order: chloroform, 30 min; acetone, 15 min; 100% ethyl alcohol (EtOH), 30 sec; 95% EtOH, 30 sec; 70% EtOH, 30 sec; distilled water, 30 sec, twice; cresyl violet, 20 min; distilled water, 30 sec, three times; 70% EtOH, 1 min; 95% EtOH, 1 min; 100% EtOH, 1 min; chloroform, 5 min; differentiator (95% EtOH with glacial acetic acid added until the pH was 4.1), 6 min; 95% EtOH, 2 min, 100% EtOH, 3 min, twice; xylene, 2 min; and xylene, 3 min, twice. After staining the sections were mounted with neutral balata and covered with a cover-slip.
The brain slices in each section were photographed (DM5000B; Leica). Normal neuronal profiles in the pyramidal cell layer of hippocampal area CA2 of the right side were counted. In each section the number of neuronal profiles, each identified as having a distinct nucleolus, were assessed in a 1-mm section of area CA2 at 200 × magnification. Hippocampal cell counts were taken from six sections per hemisphere, with two sections from each of three different coronal levels (3.1, 3.8, and 4.4 mm posterior to the bregma).
TUNEL assay
Apoptosis was measured with terminal deoxynucleotidyl transferase-mediated dUTP nick end labeling (TUNEL) staining of brain slices (sectioned at 4 μm thickness), using the TACS™ TdT Kit (Trevigen, Gaithersburg, MD). The positive cells in the brain tissue surrounding the cortical contusion area (see Fig. 1A) were identified and counted using a light microscope by an investigator blinded to study group. The extent of brain damage present was evaluated by the apoptotic index, which was the average number of TUNEL-positive cells in each section counted in 10 microscopic fields (at 200 × magnification).
Statistical analysis
All values are presented as mean ± standard deviation. Data from two groups were analyzed with the Student's t-test (non-directional), and data from repeated groups with one-way ANOVA and the Newman-Keuls test for post-hoc comparisons. Differences were considered statistically significant at a level of p < 0.05.
Results
Comparison of the effects of three different HBO treatment protocols
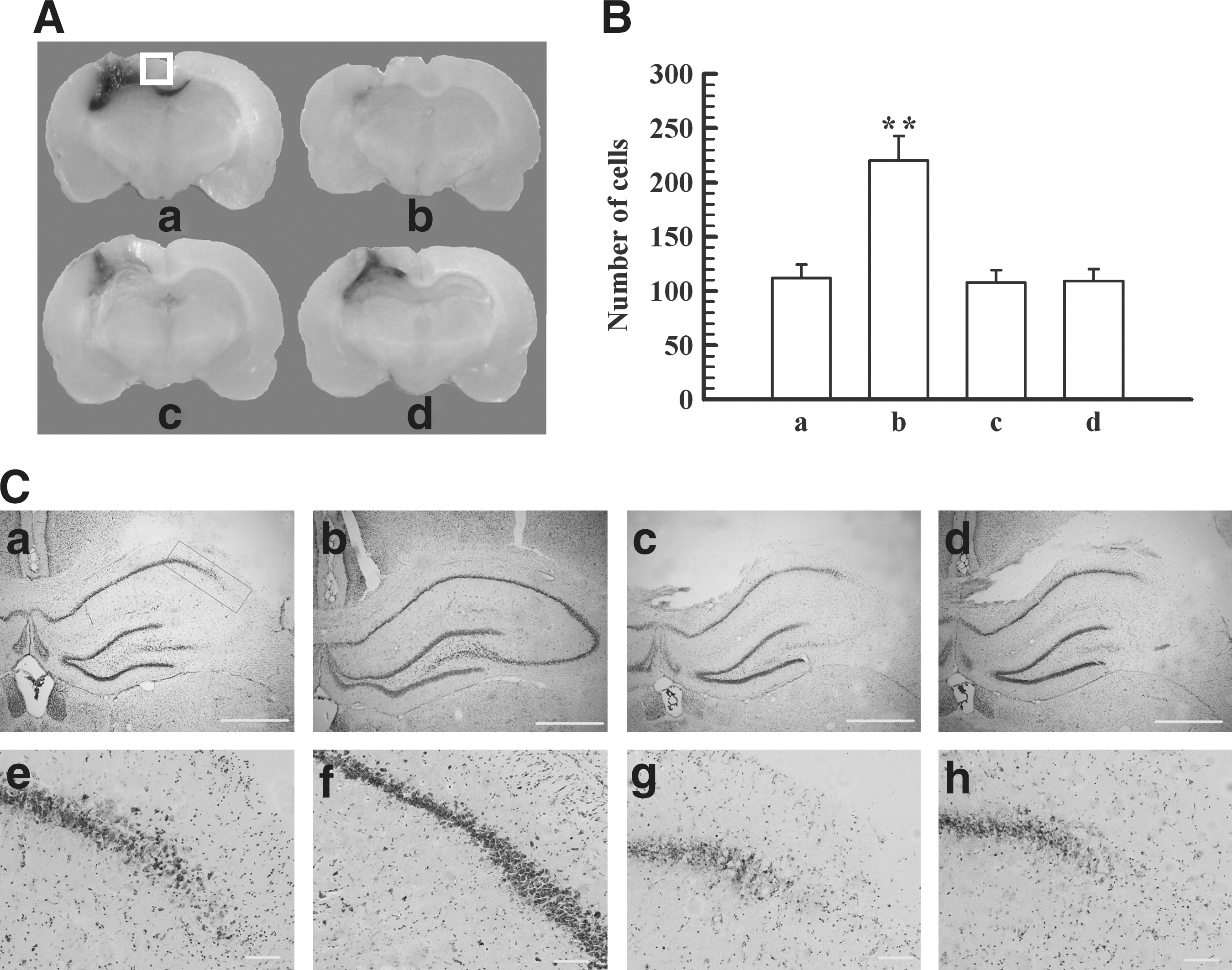
The rats were randomly divided into four groups: a control group, an HBO group, a normobaric hyperoxia group (100% O2, 1 ATA), and a hyperbaric normoxia group (3 ATA, partial pressure of O2 0.21 ATA). To observe structural changes, all animals were killed 48 h after TBI. The weight-drop trauma produced a wedge-shaped, highly reproducible lesion involving the parietal cortex and the subcortical white matter (Fig. 1A-a). Grossly, the lesion was characterized by a central cavity encompassed by a zone of hemorrhagic necrosis that was well delineated from the surrounding tissue. The lesions in the HBO group were less severe than those in the control group (Fig. 1A-b). However, with normobaric hyperoxia or hyperbaric normoxia, the lesions were similar to those seen in the control group (Fig. 1A-c and A-d). Microscopically, the outlines of the CA2 and CA3 areas in the hippocampus were damaged by TBI (Fig. 1C-a and C-e). The number of neuronal cells revealed by Nissl staining was greatly reduced after TBI (112.0 ± 12.45). However, when the rats were treated with HBO (3 ATA, 100% O2), at 6 h after TBI the number of neurons (220.0 ± 23.0) was significantly higher than without treatment (p < 0.01, Fig. 1B). Compared with the control group, the numbers of neurons in both the normobaric hyperoxia group and the hyperbaric normoxia group were not significantly different (p > 0.05, Fig. 1B).
Time window of HBO treatment
In order to observe the time window of the neuroprotective effect, HBO therapy was started at 3, 6, 12, 24, 48, and 72 h after TBI. The neurological evaluations, brain water content, and histopathological changes were analyzed 4 d post-TBI. We found that the onset of HBO treatment at 3, 6, or 12 h significantly reduced neurology deficit scores and brain water content (p < 0.01, Fig. 2A and B). However, no discernible effect was observed for these two variables when HBO treatment was started at 24, 48, or 72 h after TBI (Fig. 2A and B, p > 0.05). Compared with the sham-operated group, the number of neuronal cells revealed by Nissl staining was greatly reduced after TBI (p < 0.01), as shown in Figure 2C and D. When the rats were treated with HBO at 3, 6, or 12 h after TBI, the numbers of neurons were clearly increased (p < 0.01), but not in groups in which HBO treatment was started at 24, 48, or 72 h after TBI (Fig. 2C and D, p > 0.05).
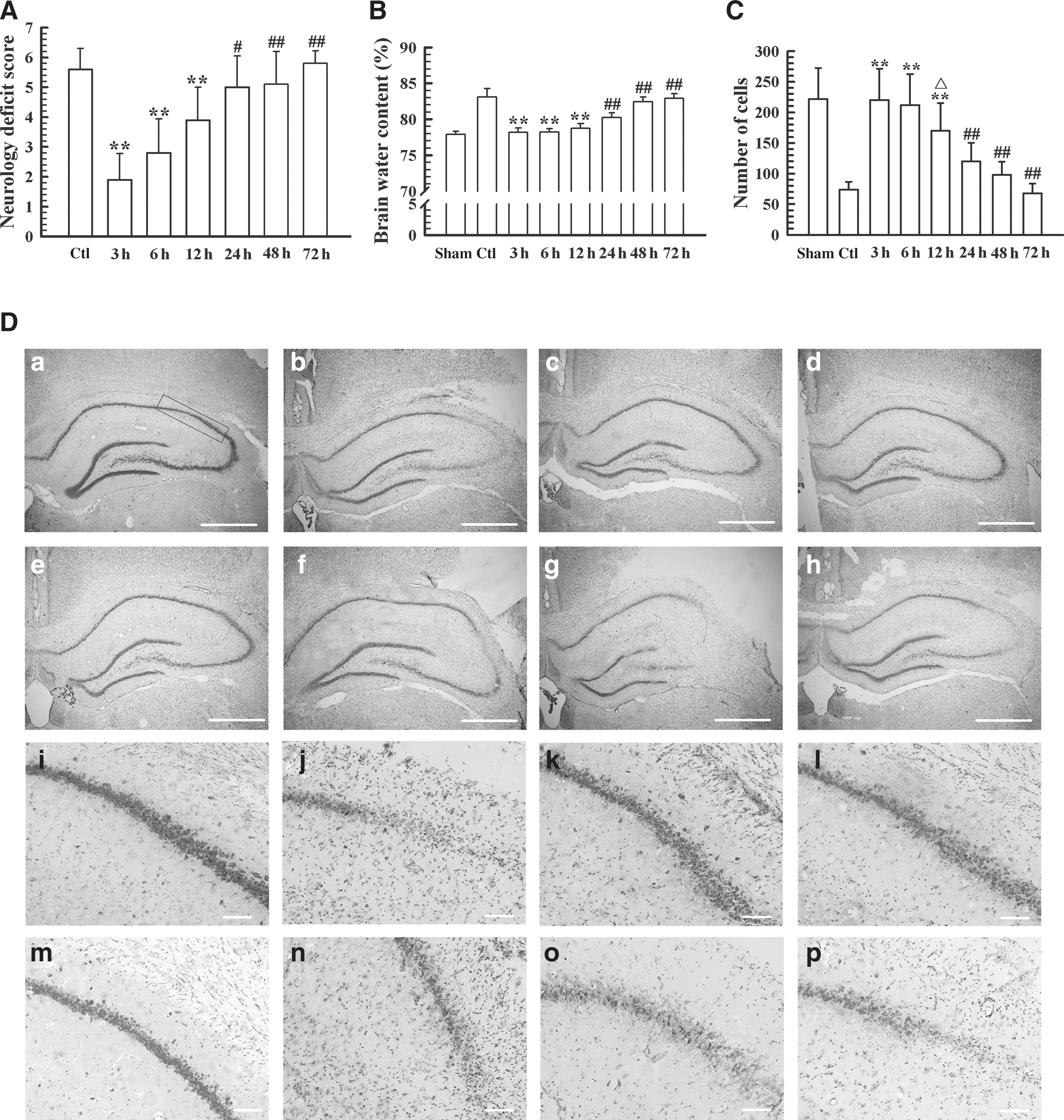
Time window of the onset of hyperbaric oxygen (HBO) treatment for rats with traumatic brain injury (TBI). (
Multiple HBO treatments expand the therapeutic window
In these studies, we found that HBO used at 3–12 h following TBI reduced brain water content, improved neurological outcome, and decreased neuronal loss. However, HBO treatment started at 24–72 h had a less neuroprotective effect. The greatest effects of HBO treatment were seen when it was given three or five times per day, especially for the delayed-treatment group. The neurology deficit scores of all rats were evaluated on the day before the final HBO treatment in the 72-h group. Then the animals were sacrificed for histological examination.
As shown in Figure 3F, for animals that received the first HBO treatment 6 h after TBI, multiple treatments appeared to further decrease the neurology deficit score and alleviate neuronal loss, but the values of these two parameters were not significantly different from animals receiving only one treatment (p > 0.05).
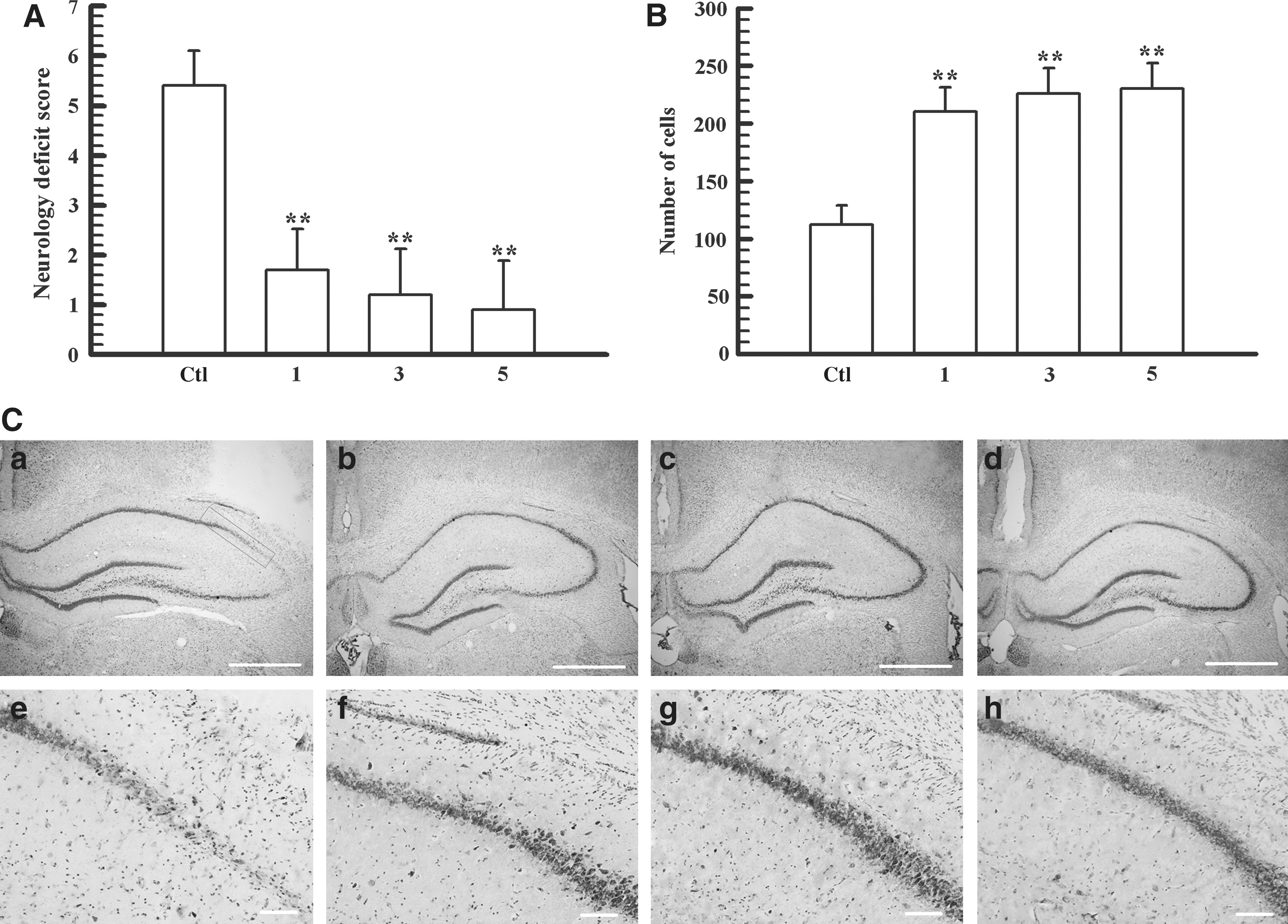
The effect of multiple hyperbaric oxygen (HBO) treatments, with the first treatment given at 6 h after traumatic brain injury (TBI). (
As shown in Figure 4, when the first HBO treatment was given 24 h after TBI, multiple HBO treatments decreased neurology deficit scores and increased neuronal loss significantly (p < 0.01). The effect of HBO was more marked with two treatments than with only one treatment (Fig. 4). However, no significant difference in the effects of HBO on these two parameters was observed between three and five treatments (p > 0.05, Fig. 4).
The effect of multiple hyperbaric oxygen (HBO) treatments, with the first treatment given 24 h after traumatic brain injury (TBI). (
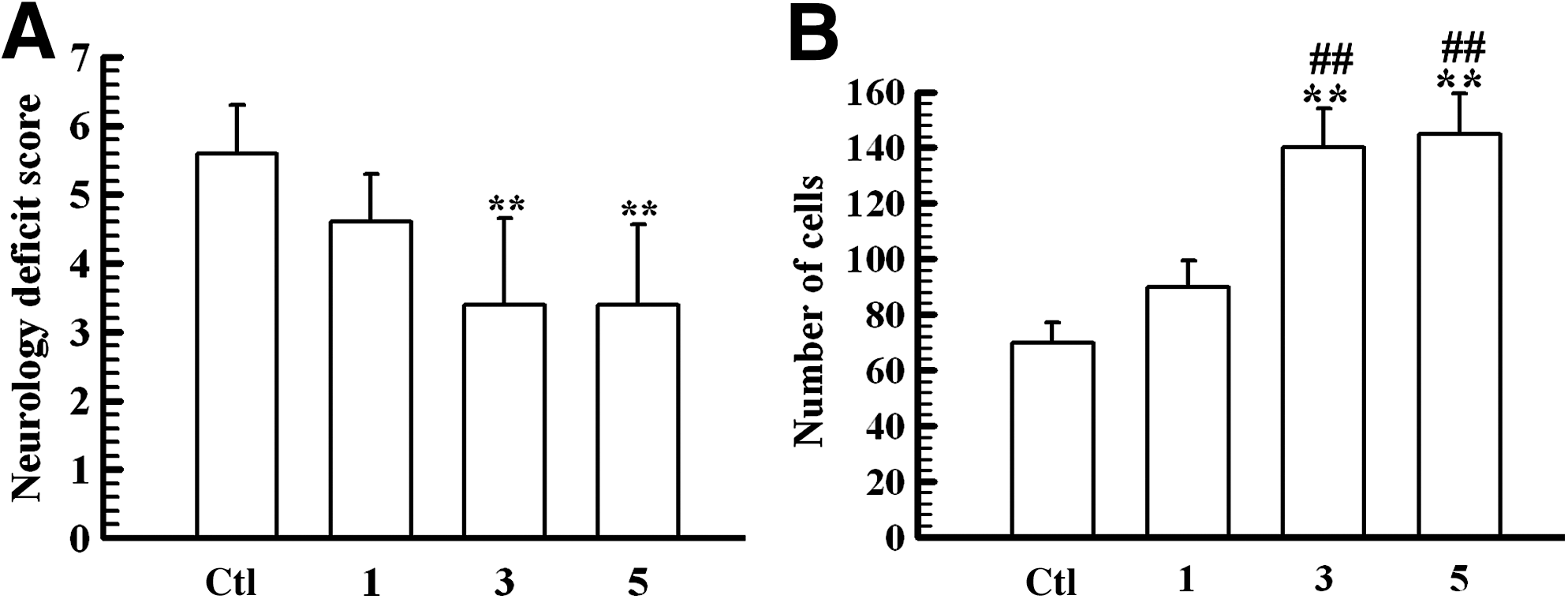
When the first HBO treatment was carried out 48 h after TBI, the results of three and five HBO treatments were similar to those seen when the first treatment was given 24 h after TBI (Figs. 4 and 5). Compared with the control group, three and five treatments reduced neurology deficit scores (p < 0.01, Fig. 5), and increased the number of neurons (p < 0.01, Fig. 5). However, the reduction in neurology deficit scores and elevation of neuron numbers were less than those of animals receiving one HBO treatment administered 3 or 6 h after TBI (p < 0.05 or 0.01, Figs. 2 and 5). In addition, five treatments did not show any improvement of efficacy for these two parameters compared with three treatments (p > 0.05, Fig. 5).

The effect of multiple hyperbaric oxygen (HBO) treatments, with the first treatment given 48 h after traumatic brain injury (TBI). (
When the first treatment was delayed until 72 h post-TBI, three or five HBO treatments did not improve neurological outcomes (p > 0.05), and only slightly elevated the numbers of neurons (p < 0.05, data not shown).
Effect of HBO treatment on neuronal apoptosis
Compared with sham-operated rats, the expression of bcl-2 mRNA in the cortex surrounding the contusion area was greatly reduced after TBI (p < 0.01, Fig. 6A and D). However, when the animals were treated once with HBO at 6 h after TBI, the expression of bcl-2 mRNA recovered partially (p < 0.05). The level of expression of bax mRNA in the control group tended to increase, but it was not significantly different from those of the other two groups (p > 0.05, Fig. 6B and D). Thus the changes in the relative ratio of bcl-2 to bax were almost identical to those of bcl-2 mRNA (Fig. 6D). Changes in the expression of caspase-3 mRNA were opposite to those of bcl-2 mRNA (i.e., caspase-3 mRNA expression was markedly increased after TBI [p < 0.01], but were significantly reduced by HBO treatment [p < 0.01, Fig. 6C and D]).
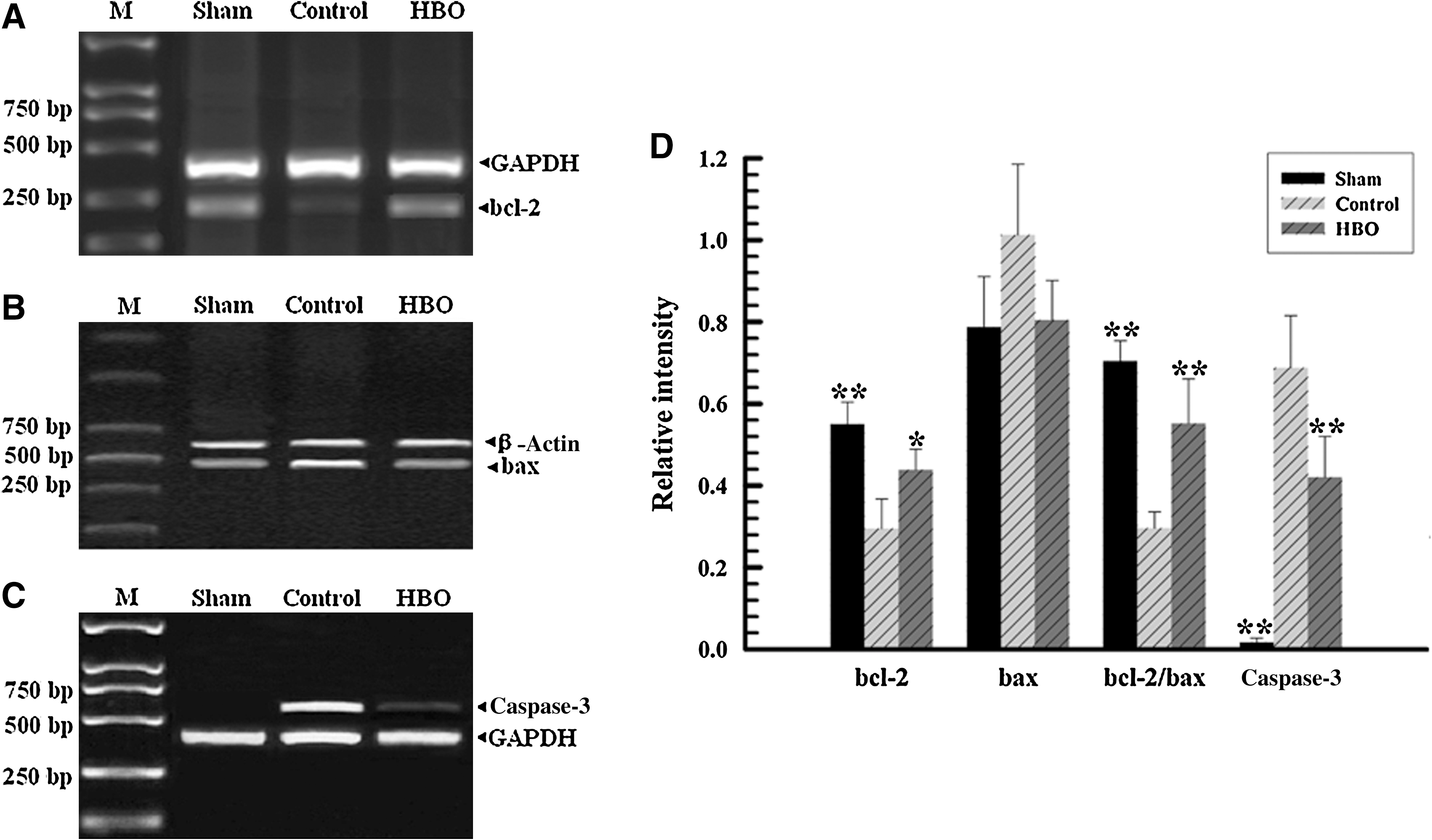
The expression of bcl-2, bax, and caspase-3 mRNA in the right parietal cortex. (
Few TUNEL-positive apoptotic cells were found in the cortex of sham-operated rats (Fig. 7A and D). In the control group, the numbers of apoptotic neurons in the cortex surrounding the primary injury site were significantly increased after TBI (p < 0.01, Fig. 7B and D), but were decreased by HBO treatment (p < 0.05, Fig. 7C and D).
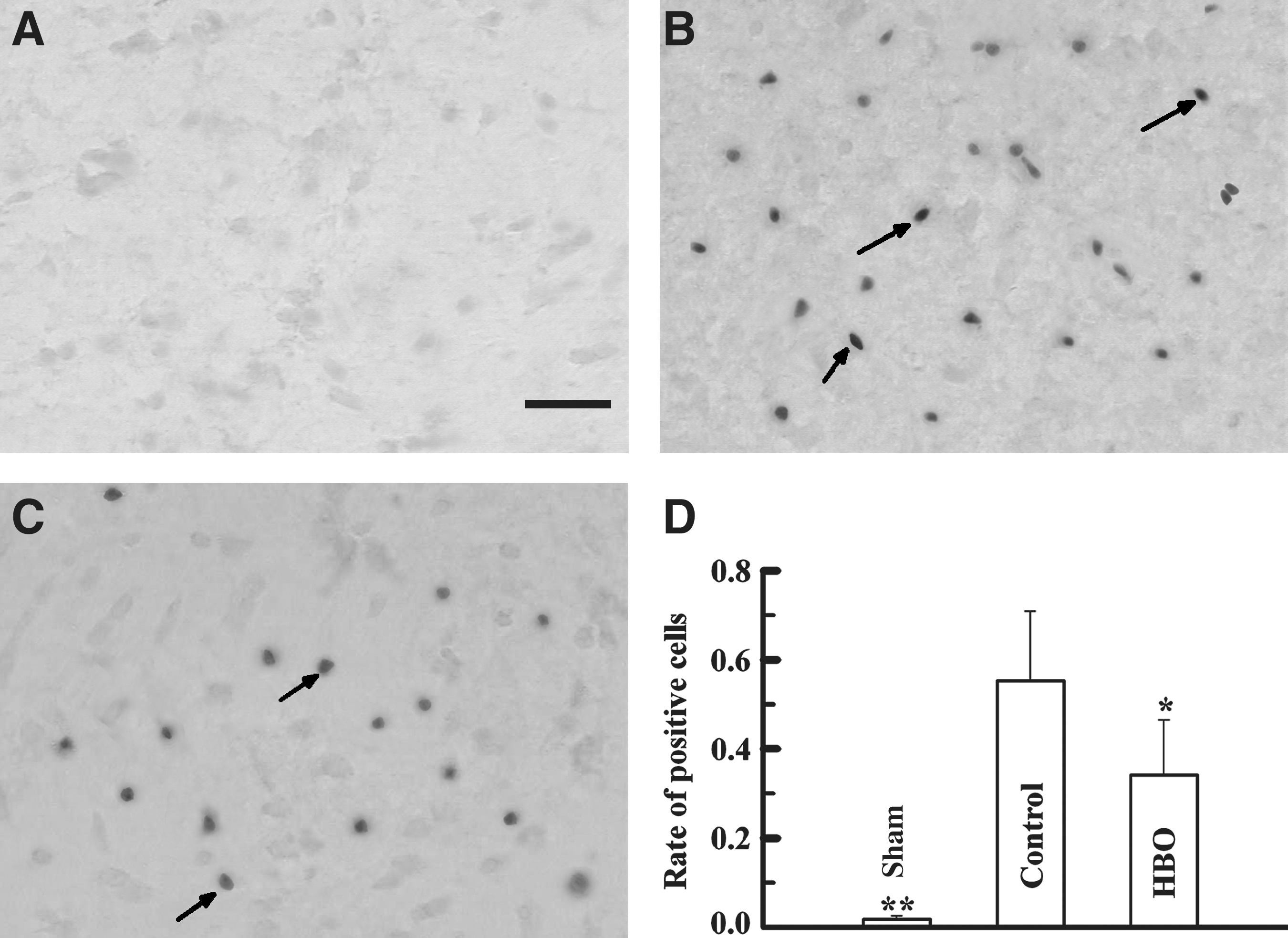
TUNEL staining of the right parietal cortex in the different treatment groups. (
Discussion
On the basis of the neurological functions and histopathological changes seen in the present study, we found that HBO treatment after TBI can exert significant neuroprotective effects. We found that HBO treatment in rats after experimental TBI decreased cerebral water content, improved neurological recovery, and reduced hippocampal neuron loss, thus providing clear experimental data to validate the efficacy of HBO treatment. This effect appears to be attributable to exposure to pure hyperbaric oxygen, since hyperbaric normoxia and normobaric hyperoxia treatment had no significant effect on the aforementioned parameters. The effects of these three different treatment protocols have rarely been compared before. Our results using HBO treatment for TBI are consistent with those of many other researchers (Neubauer et al., 1994; Niklas et al., 2004; Rockswold et al., 2001, 2009; Zhou et al., 2007). Although a few investigators have reported that early normobaric hyperoxia therapy has beneficial effects on TBI (Menzel et al., 1999a, 1999b; Palzur et al., 2004; Rockswold et al., 2009; Tolias et al., 2004), the present data and those of other studies (Diringer et al., 2007; Zhou et al., 2007) do not support this conclusion.
Ischemia, elevated intracranial pressure, and reduced cerebral blood flow are widely recognized as major factors causing secondary brain injury after severe TBI (Cormio et al., 1997). HBO treatment is thought to improve the ischemic condition of the brain tissue surrounding the primary injury (Calvert et al., 2007; Palzur et al., 2004). Because the volume of oxygen in the blood is proportional to the increase in partial oxygen pressure, according to Henry's law (Calvert et al., 2007;Gill and Bell, 2004), there is a massive increase in blood oxygen levels with the use of hyperbaric oxygen (Calvert et al., 2007; Goldman, 2009; Niklas et al., 2004; Tibbles and Edelsberg, 1996;). Insufficient transport and delivery of oxygen to tissues can be compensated for by a high P
Inconsistent data have been reported about the effectiveness of HBO on TBI (Adamides et al., 2006; Rockswold et al., 2007). The contradictory reports probably result from differences in TBI models and HBO treatment methods, including the timing of HBO and the number of treatments, which are two of the most important factors affecting the efficacy of HBO. In the present study, we found that HBO given at 3–12 h following TBI reduced neurology deficit scores, brain water content, and neuronal loss, but HBO given at 24–72 h had fewer neuroprotective effects. These time-dependent differences in the efficacy of HBO suggest that it should be implemented as soon as possible after TBI. Our study also demonstrated that delayed but repeated HBO treatments could also exert protective effects against secondary brain injury in rats. The efficacy of HBO treatments can thus be obtained, even when the first treatment is delayed by 48 h. Thus repeated treatments could extend the time window of effective HBO therapy to 48 h after TBI. This result is consistent with the report by Yin and Zhang (2005), who studied HBO treatment of experimental ischemic stroke in rats. Nonetheless, we found that repeated HBO treatments were less effective when the first treatment session was much delayed. Moreover, we found that the efficacy of five consecutive HBO treatments appeared to be no better than that of three treatments. This indicates that HBO treatment does not have to be repeated indefinitely when the first HBO intervention is given 48 h after TBI, as this appears to be the time point at which the optimal effects of hyperbaric oxygen therapy are seen (Rogatsky et al., 2003). These findings about the therapeutic time frame for optimal dosing, which has not been systematically studied before, extend our knowledge about the use of HBO to treat TBI.
Numerous TBI models have been designed to study human brain injury, and an ideal model would replicate all aspects of human brain injury. In addition, the responses to injury specified in physiological, behavioral, and anatomical terms should be reproducible and quantifiable over a continuum of injury severity (Park et al., 1999). The neocortical contusion procedure and focal cortical weight-drop procedure that we used that were based on Feeney's model produced cerebral lesions that are structurally similar to those observed clinically. The injury results in a cortical cavity that extends into the underlying white matter, with microscopic injury to underlying structures, including the hippocampus (Golarai et al., 2001; Weisend and Feeney, 1994). In our study, this TBI model yielded findings similar to those reported by Chen and associates (2008). Both the macroscopic appearance and the microscopic findings were similar to those seen in clinical situations. A peri-lesional penumbra could clearly be seen and was easily differentiated from the spared surrounding brain tissue. These characteristics justified the selection of this model for the investigation of focal TBI in our study.
It is well known that one important factor hindering the use of HBO therapy is the risk of oxygen toxicity resulting from breathing 100% oxygen under high pressure (Kleen and Messmer, 1999). In general, HBO is a relatively safe treatment (Gill and Bell, 2004), but it does carry some risk, especially when given at high pressure (>3 ATA) and for long duration (Blenkarn et al., 1969; Plafki et al., 2000). Blenkarn and associates (1969) reported that HBO given at 4.96 ATA for 1 h caused central nervous system toxicity in rats. Hampson and Atik (2003) reported an overall incidence of oxygen-toxic seizures of 0.03% when HBO treatment was routinely used in all kinds of patients. The Committee of the Undersea and Hyperbaric Medical Society (CUHMS) recommends that levels of 2.4–3.0 ATA should be used, or the lowest pressure that is effective, to avoid oxygen-induced convulsions (Zhang et al., 2005). Using a relatively low pressure, Mink and Dutka (1995) found that HBO (2.8 ATA for 75 min) did not increase lipid peroxidation and promote early brain injury. We did not study the potential side effects of HBO treatment in this study. However, the pressure we selected was in the range recommended by the CUHMS for patient use. Moreover, HBO treatment at 2.5–3 ATA for 1–2 h is usually used for experimental studies in rats (Calvert et al., 2003; Niklas et al., 2004; Qin et al., 2008; Vlodavsky et al., 2005).
Growing evidence suggests the involvement of apoptotic processes in delayed post-traumatic neuronal death (Ng et al., 2000; Smith et al., 2000). In this study, we found that the numbers of TUNEL-positive cells seen in the cerebral cortex surrounding the primary injury site were significantly increased after TBI, but were reduced with HBO treatment. In addition, we observed with RT-PCR that the expression of bcl-2 mRNA was decreased and caspase-3 mRNA was elevated after TBI. HBO treatment increased the expression of bcl-2 mRNA with enhancement of the ratio of bcl-2 to bax, and reduced caspsase-3 mRNA levels. These results support the involvement of apoptosis in secondary brain injury after TBI (Liu et al., 2006; Ng et al., 2000; Palzur et al., 2004; Smith et al., 2000; Vlodavsky et al., 2005). This suggests that the protective effects of HBO may be at least partly attributable to reductions in apoptotic activity of brain tissue after TBI (Liu et al., 2006; Palzur et al., 2004; Vlodavsky et al., 2005).
In conclusion, our results suggest that HBO treatment can help alleviate brain damage after TBI. With a single HBO treatment, the most effective time point at which to give it is about 12 h post-TBI, and multiple HBO treatments may help extend the time window of efficacy. Taken together, our results considerably extend current knowledge about the application of HBO post-TBI. We conclude that HBO therapy is potentially beneficial as an adjunctive treatment for TBI.
Footnotes
Acknowledgments
The authors wish to thank Dr. Temugin Berta for help revising the manuscript, and Dr. Yong-Jing Gao for constructive suggestions about the writing of the manuscript. This study was supported by a grant from the Administration of Science and Technology of Nantong (project no. S5031), Jiangsu Province, China.
Author Disclosure Statement
No conflicting financial interests exist.