
Abstract
In the setting of acute brainstem herniation in traumatic brain injury (TBI), the use of hyperventilation to reduce intracranial pressure may be life-saving. However, undue use of hyperventilation is thought to increase the incidence of secondary brain injury through direct reduction of cerebral blood flow. This is a retrospective review determining the effect of prehospital hyperventilation on in-hospital mortality following severe TBI. All trauma patients admitted directly to a single level 1 trauma center from January 2000 to January 2007 with an initial Glasgow Coma Scale (GCS) score ≤8 were included in the study (n = 77). Patients without documented or with late (>20 min) arterial blood gas at presentation (n = 12) were excluded from the study. The remaining population (n = 65) was sorted into three groups based on the initial partial pressure of carbon dioxide: hypocarbic (P
Introduction
The effect of hyperventilation to reduce ICP is well understood. Hyperventilation causes cerebral vasoconstriction through the potent vasomotor effect of hypocarbia, thus decreasing ICP by reduced cerebral blood volume (Chestnut et al., 2002; Raichle and Plum, 1972). Experimentally this effect is evident; the potent vasomotor effects of carbon dioxide induce a 3% decrease in cerebral blood flow (CBF) for every 1 mm Hg drop in P
With clear theoretical benefits but little clinical proof of efficacy, the Brain Trauma Foundation (BTF) has published guidelines for the use of hyperventilation in trauma (The Brain Trauma Foundation, 2000b, 2007). The basis of these guidelines is the overwhelming evidence of the detrimental effects of hyperventilation in the setting of severe TBI with regard to increasing secondary brain injury by decreasing CBF, but sporadic success of ICP reduction in the face of acute herniation.
Experimental studies of cerebral blood flow following severe TBI have elucidated the mechanism by which hyperventilation may be detrimental shortly following trauma. Many authors have confirmed decreased global CBF in the first day after TBI (Bouma et al., 1991; Coles et al., 2004; Marion et al., 1991; Overgaard and Tweed, 1974). This is particularly true in patients with diffuse cerebral edema, and has been characterized as well in patients with traumatic mass lesions (Bouma et al., 1991; Schmidt et al., 2003). This drop in CBF normalizes and typically develops into a relatively hyperemic state, with cerebral blood flow exceeding metabolic demand in the 24- to 48-h window post-injury (Martin et al., 1997). Data extrapolated from these studies suggest that the decrease in CBF following TBI is of greatest significance immediately following the injury (Bouma et al., 1991; Marion et al., 1991). This is supported by animal models, that show a decrease in CBF (Pfenninger et al., 1989) and CPP (Zauner et al., 2002) within minutes following fluid percussion injury.
When hyperventilation is superimposed on this phenomenon, a relative ischemia ensues, resulting in tissue acidosis tantamount to secondary brain injury. This theory is strengthened by studies showing that following trauma metabolites such as lactic acid are found in higher concentrations, and that these higher concentrations are seen following even very short periods of hyperventilation (Marion et al., 2002). On autopsy, the effect of ischemic changes on brain tissue have been confirmed in most patients with fatal severe TBI (Graham and Adams, 1971).
If the concept of relative ischemia in the early post-injury period is accepted, very early (i.e., prehospital) intervention to prevent secondary injury should be a goal in the management of TBI. This role will fall into the hands of first responders and transport teams en route to the trauma center. As noted in the literature, the tendency of prehospital ventilation of patients with TBI is toward hyperventilation, whether indicated or not by the BTF guidelines (Helm et al., 2003; Lal et al., 2003). We anecdotally noted at our center that patients with TBI tended to be indiscriminately hyperventilated regardless of the presence or absence of signs of brainstem herniation. This observation is not unique to our hospital and has been commented on previously (Di Bartolomeo et al., 2003; Thomas et al., 2002). This observation prompted our study, the primary goal of which was to determine if inappropriate hyperventilation in head-injured patients was contributing to mortality of brain-injured patients, presumably through secondary brain injury.
Methods
This study is a retrospective chart review. Data were extracted from our institutional trauma database collected from chart review by non-physician members of the trauma team. At our institution the trauma database was reformed as of January 2000, thus no data prior to this date were used. Study subjects included all patients age >17 years presenting directly to Fletcher Allen Health Care (FAHC) from site of injury between the dates of January 2000 and January 2007 with initial Glasgow Coma Scale (GCS) scores <8 (n = 77). This eliminates a significant portion of our trauma population, those patients presenting to non-tertiary care centers, who are typically transferred to our facility following primary survey. Patients with no documented presenting arterial blood gas or blood gas acquired more than 20 min after arrival (n = 12) were excluded from this study. The remaining population (n = 65) was sorted based on initial partial pressure of carbon dioxide (P
Patients are not intubated by first responders or during transport at our hospital, thus no patients in this group were intubated prior to arrival at the hospital. Patients receive manual bag-mask breaths throughout transport to the trauma center. Routine trauma protocol is for arterial blood gas to be acquired concurrently with commencement of primary survey. Our standard of data collection is for arterial blood gas to be acquired as rapidly as possible, with using portable point-of care analyzers. Point-of-care analyzers allow alterations in physiological state such as hypothermia, and provide results within minutes. Due to the technical detail of acquisition of arterial blood gases, no standards of time of intubation or initiation of mechanically delivered ventilation exist. All blood gas levels acquired 20 min or more following arrival in the hospital were eliminated from the study.
Variables thought to be potential confounders, including age, sex, level of arousal (GCS; Teasdale and Jennett, 1974), Injury Severity Score (ISS; Baker et al., 1974), evidence of brainstem herniation or mass lesion by examination, partial pressure of oxygen, transit or intra-resuscitative hypoxia and apnea, and time of transit, were either extracted from the original record or the database as available. With few exceptions, an intracranial pressure (ICP) monitor or ventriculostomy were placed in this population shortly following admission. Craniotomy performed during admission was recorded. Primary outcome was in-hospital mortality.
The GCS score was that recorded on arrival by the appropriate member of the trauma team, typically the on-call neurosurgery resident. ISS was defined as initially described (Baker et al., 1974), and was included as a measure of multi-system trauma. Brainstem herniation was defined as localizing findings on initial examination. Hypoxia was defined as Pa
The independence of analog data variables considered to be potentially confounding, and primary outcome of in-hospital mortality, was analyzed with a 3 × 2 Fischer's exact test. The independence of normal variables was analyzed with analysis of variance (ANOVA). For both Fischer's exact test and ANOVA analysis, the 5% level was used to define statistical significance. Data were compared with online statistics calculation software (
Statistical analysis
For multivariate analysis, continuous and nominal data were dichotomized and binary logistic regression performed using SPSS software (SPSS 16.0 for Windows). Data were dichotomized as follows: P
Results
In-hospital mortality
Sixty-five patients were included in the study group. The mechanism of injury was most commonly motor vehicle collisions (32/65, 49%). The remaining half of injuries were acquired via fall (20), gunshot wound (5), skiing (3), or other (8). The inequity of penetrating to blunt trauma is characteristic for our center. The most frequent injury diagnosed was subdural hematoma (17/65, 26%). The remaining list of injuries includes subarachnoid hemorrhage (8), contusion/concussion (7), diffuse axonal injury (6), diffuse edema/hypoxia (6), epidural hematoma (5), ballistic/penetrating (5), fracture (5), intraparenchymal hematoma (4), and undiagnosed (2).
The characteristics of the study group are outlined in Table 1. The groups are statistically matched in all groups with the exception of age (p = 0.003). The hypocarbic group had a significantly older population (mean age 54.1 years) compared with the other groups (mean age 36.4 years). The normocarbic and hypercarbic groups were matched for age (p = 0.787).
Statistically significant to p < 0.05 between groups.
P
Our data display a correlation between presenting P
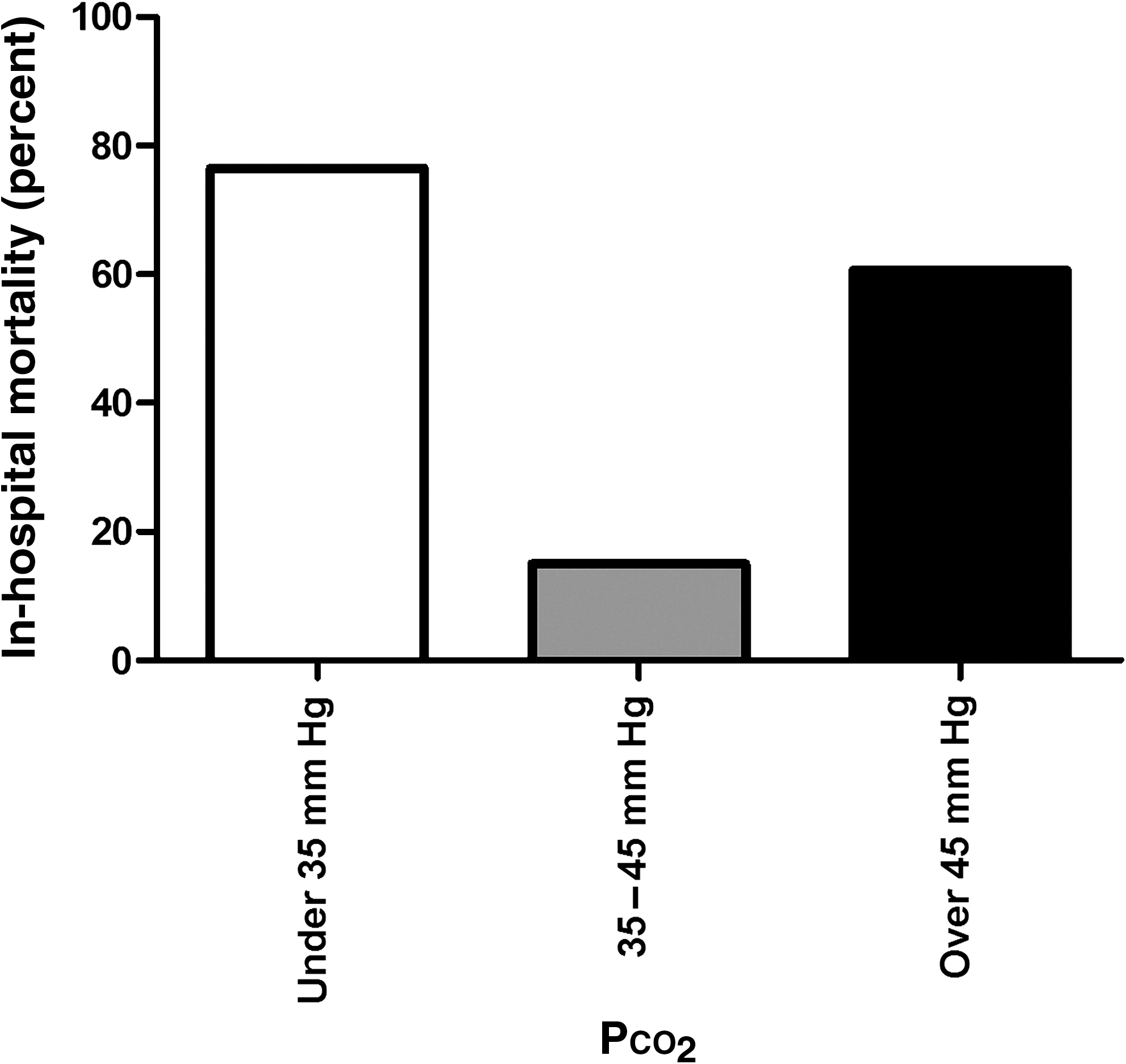
Partial pressure of carbon dioxide (P
For non-survivors, the cause of death was from head injury for nearly all (26 of 33, 79%) patients. The most frequent cause of death was brain death (12/33, 36%) or withdrawal (14/33, 42%) of care by family request due to severity of coma in the absence of brain death. Seven patients had non-neurological causes listed as the primary cause of death. Of these patients, four had asystole (3 on the day of trauma, 1 on hospital day 14), two died of hemorrhagic shock, and one had sepsis from colitis before care was withdrawn on the 26th day after trauma.
Inappropriate use of hyperventilation
In our study group, a majority of patients 46 of 65 (72%) had no evidence of brainstem herniation on initial CT scan. Only 3 of 17 (18%) hypocarbic (hyperventilated) patients had evidence of brainstem herniation, while ironically 25% of normocarbic (normoventilated) and 36% of hypercarbic (hypoventilated) patients had evidence of brainstem herniation.
Overall, only 3 of 19 (16%) patients with evidence of brainstem herniation were hyperventilated, while 14 of 46 (30%) severely head-injured patients with no evidence of brainstem herniation were improperly hypocarbic (hyperventilated). Nearly half of patients (30/65, 46%) were not treated in accordance with the recommendations of the BTF. For example, 15 patients with signs of brainstem herniation were not hyperventilated. These results are summarized in Fig. 2.

Hyperventilation, normoventilation, and brainstem herniation.
Multivariate analysis
Because of the potential confounding factors delineated above, a multivariate analysis was performed for predictors of in-hospital mortality. Recorded variables found to be independent risk factors for in-hospital mortality were included in this analysis (Tables 2 and 3). For this cohort of patients, the most significant risk factors for prediction of death included age older than 50 years and abnormal Pa
ISS, Injury Severity Score; GCS, Glasgow Coma Scale; P
ISS, Injury Severity Score; GCS, Glasgow Coma Scale; P
P
Discussion
Measurement of the partial pressure of carbon dioxide and ventilatory status
Ventilatory status following brain injury has been well studied (Vicario et al., 1983). It is not surprising that there is a direct correlation between low level of arousal and a decrease in ventilatory drive and hypercarbia. A patient suffering severe brain injury may have patterns of both spontaneous hyperventilation and hypoventilation, though there is a tendency toward hypoventilation and hypercarbia in those with the lowest scores on the Glasgow Coma Scale (Vicario et al., 1983). Because of the irregular breathing patterns and frequent hypoventilation encountered with severe TBI, early intervention with control of airway and manual or mechanized ventilation is recommended for optimal outcome (Davis et al., 2005).
At our institution, prehospital trauma care is implemented by trained emergency technicians and volunteers, but few trained paramedics. As a result, patients arriving directly to the hospital from the site of injury are not intubated, but instead mechanical breaths are delivered manually via bag-mask throughout transport, if needed.
Throughout this article, the terms hypocarbia/hyperventilation and hypercarbia/hypoventilation are used in an interchangeable manner. It is important to recognize the limitations of using P
A superior study would involve patients suffering TBI randomized into equal groups of hyperventilated, normoventilated, and hypoventilated groups, with in-transit monitoring of P
Inappropriate prehospital ventilation increases in-hospital mortality from traumatic brain injury
The primary outcome of in-hospital mortality had significant variance between the three groups (Fig. 1). This effect appears to be independent of other variables known to be correlated with poor outcome from TBI. We propose that these differences are accounted for by the complex physiological changes induced by alterations in the partial pressure of carbon dioxide. These physiologic responses promote suboptimal conditions following TBI, which induces secondary brain injury and associated clinical morbidity. This presents a potential therapeutic strategy for the prevention of secondary brain injury in TBI, via normalization of P
The hypocarbic group had the greatest in-hospital mortality rate. The presumed physiologic response to P
The hypercarbic group had higher mortality than average. To some degree this was surprising, as we have seen improvement in physiological parameters with permissive hypercarbia/hypoventilation in a fluid percussion model of TBI in swine (unpublished data), and other authors have suggested hypoventilation as a potential therapeutic strategy (Manley et al., 2000). In a normal physiological setting, hypercarbia/hypoventilation induces an increase in CBF by a reverse mechanism of hypocarbia/hyperventilation (Deem, 2006; Stochetti et al., 2005). In concert with the known decrease in CBF following TBI, this vasodilating response to hypercarbia would normalize CBF. As an additional benefit, the oxygen-hemoglobin dissociation curve would be right-shifted due to the change in P
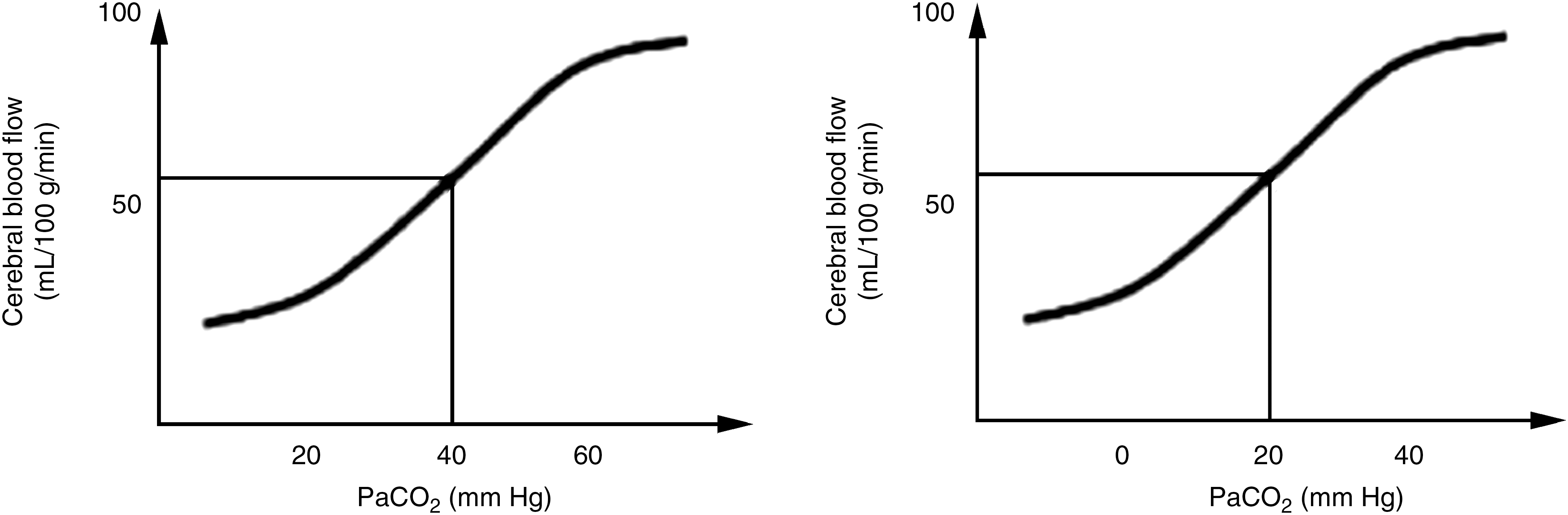
Left shift of cerebral vasculature reactivity to carbon dioxide in traumatic brain injury (P
Normocarbic patients had low mortality compared with the average. These patients presumably have optimized CBF following TBI, thus minimizing secondary brain injury. Using presenting P
Subgroup analysis: Age
A potential confounding factor in this study is age, which is known to have prognostic value following TBI. Patients aged more than 50 years suffering TBI have been shown to have poor outcomes (The Brain Trauma Foundation, 2000c). There was a statistically significant increase in age in the hypocarbic group (p = 0.003). This difference may be explained by undiagnosed pulmonary disease in the hypocarbic group, which could change baseline P
The inequity in age between the groups allows for subgroup analysis. The cohort of 65 patients was divided into two groups: patients aged 50 or less, and patients older than age 50. These two groupings were then subdivided into hypocarbic, normocarbic, and hypercarbic groups as previously defined, and in-hospital mortality was compared. The results are summarized in Table 4. This yields a strong association between normocarbia and diminished in-hospital mortality (p < 0.003) in the group aged 50 years or less. In-hospital mortality was very high for all patients aged 50 or more (17/21, 81%). In this group, the trend toward improved survival is seen with all patients and patients aged under 50 years (Fig. 4), though the difference was not statistically significant (p = 0.175) due to limited power. Overall, the results suggest a strong correlation between in-hospital mortality and P

Age-adjusted in-hospital mortality (P
Subgroup analysis: Glasgow Coma Scale score
While there was no significant differences (p = 0.071) between GCS scores between the study groups, there was a clear trend toward improved level of consciousness in the normocarbic group (average GCS 6.00) compared with all other patients (GCS 4.76). As GCS is known to be an independent prognostic indicator of morbidity and mortality in TBI (The Brain Trauma Foundation, 2000a), subgroup analysis was performed to determine if this was a confounding factor.
The study population was divided into groups based on initial GCS score: those with GCS scores 3–5 and those with GCS scores 6–8. These two groupings were then subdivided into hypocarbic, normocarbic, and hypercarbic groups, as previously defined, and in-hospital mortality was compared. These results are summarized in Table 5. The results suggest a strong correlation (p < 0.010) between presenting P
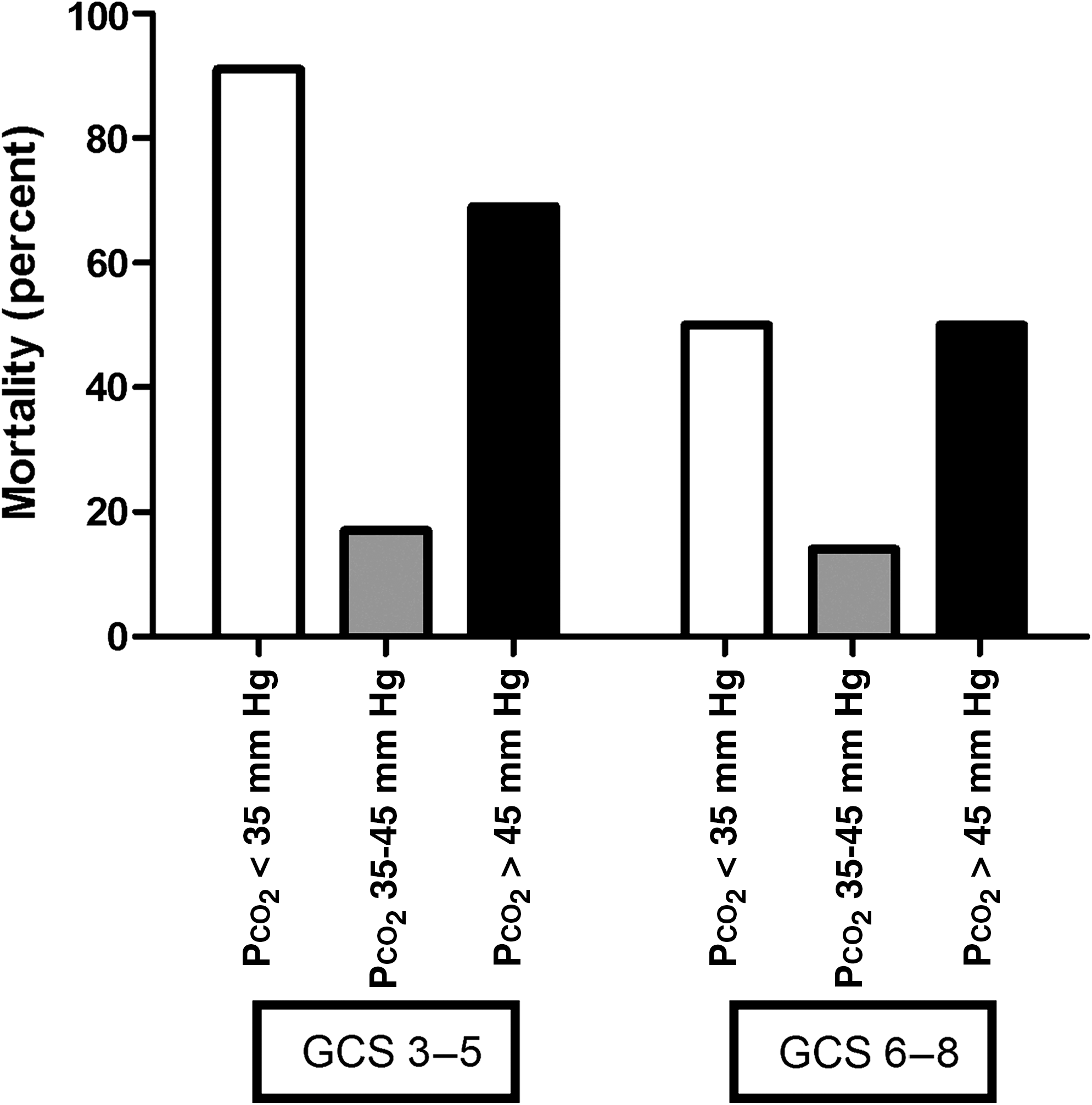
GCS-adjusted in-hospital mortality (GCS, Glasgow Coma Scale score; P
GCS, Glasgow Coma Scale; P
Avoidance of inappropriate hyperventilation in prehospital care of TBI patients
The BTF guidelines for prehospital ventilatory management recommend hyperventilation as an option for patients with signs of brainstem herniation upon examination (The Brain Trauma Foundation, 2000a, 2000b). There is no recommendation for prolonged hyperventilation, however. Using P
Several authors have discussed the virtues of noninvasive surrogate measures of P
This study represents a small sample and may be limited in its global applicability due to the modern prehospital care present in most trauma systems. However, in this cohort there was a significant correlation between reduced mortality and normocarbia. The patients in our study group were transported an average of 41 min (range 9–136 min), and the results of this study indicate that there is an opportunity for improvement in patient care. We propose that a reasonable strategy for trauma centers such as ours is to aim for normocarbia using end-tidal CO2 monitoring throughout transport from injury site to trauma center. At the trauma center, proper neurosurgical evaluation would determine whether hyperventilation is appropriate based on the Brain Trauma Foundation guidelines.
Conclusions
Our findings indicate: (1) hypocarbia/hyperventilation and hypercarbia/hypoventilation following TBI increases the risk of in-hospital mortality; and (2) normocarbia following TBI decreases the risk of in-hospital mortality.
We propose from these conclusions that abnormal physiologic states of hypercarbia and hypocarbia may induce secondary injury by inducing suboptimal oxygenation of brain tissue during early (prehospital) management. Normocarbia appears to decrease the risk of mortality by maintaining a normal physiologic state and minimizing secondary brain injury.
We suggest that implementation of universal normoventilation of patients with TBI may be optimal prehospital management until an initial evaluation by neurosurgery personnel can be carried out. Alternatively, we advocate efforts to follow the guidelines of the BTF, and to initiate hyperventilation only with elevated intracranial pressure with signs of acute brainstem herniation on examination.
Footnotes
Author Disclosure Statement
No competing financial interests exist.