
Abstract
Transplantation of bone marrow mesenchymal stromal cells (MSCs) has been shown to improve the functional recovery in various models of spinal cord injury (SCI). However, the issues of the optimal dose, timing, and route of MSC application are crucial factors in achieving beneficial therapeutic outcomes. The objective of this study was to standardize the intrathecal (IT) catheter delivery of rat MSCs after SCI in adult rats. MSCs labeled with PKH-67 were administered by IT delivery to rats at 3 or 7 days after SCI as one of the following treatment regimens: (1) a single injection (5×105 MSCs/rat), or (2) as three daily injections (5×105 MSCs/rat/d for a total of 1.5×106 MSCs/rat over 3 days, injected on days 3, 4, and 5, or days 7, 8, and 9 following SCI. The animals were behaviorally tested for 4 weeks using the Basso, Beattie, and Bresnahan (BBB) locomotor rating scale, and histologically assessed for MSC survival, distribution, and engraftment properties after 28 days. Rats treated with a single injection of MSCs at 3 or 7 days post-injury showed a modest, non-significant improvement in function and low survival of grafted MSCs, which were found attached to the pia mater or accumulated around the anterior spinal artery. In contrast, rats treated with three daily injections of MSCs at days 7, 8, and 9, but not on days 3, 4, and 5, showed significantly higher motor function recovery (BBB score 16.8±1.7) at 14–28 days post-injury. Transplanted PKH-67 MSCs were able to migrate and incorporate into the central lesion. However, only a limited number of surviving MSCs, ranging from 24,128±1170 to 116,258±8568 cells per graft, were observed within the damaged white matter. These results suggest that repetitive IT transplantation, which imposes a minimal burden on the animals, may improve behavioral function when the dose, timing, and targeted IT delivery of MSCs towards the lesion cavity are optimized.
Introduction
Therefore, because of these complexities, therapeutic interventions following SCI require a combination of at least three main strategies: (1) attenuation of the secondary injury processes (such as inflammation and glutamate excitability), and inactivation of axonal growth inhibitors (Liu et al., 2008); (2) stimulation of endogenous spinal cord neurogenesis (generating new spinal progenitors) through enhanced physical activity, enrichment environment, and pharmacological manipulation (Berrocal et al., 2007; Eaton et al., 2008); and (3) cell and gene therapy that aims to replace dead cells (neurons and oligodendrocytes), and induce a more favorable environment for axon regeneration (Cizkova et al., 2007; Coutts and Keirstead, 2008; Keirstead et al., 2005; Webber et al., 2007).
The impressive demonstration of regenerative medicine using embryonic and adult stem cells to trigger healing and functional restoration of various tissues has focused attention on the development of cellular therapies that can promote regeneration of the damaged spinal cord as well (Conrad et al., 2008; Garbuzova-Davis and Sanberg, 2009; Safinia and Minger, 2009). Several different types of cells, such as embryonic stem cells (Elisseeff, 2004), neural progenitors (Cizkova et al., 2007; Su et al., 2009), bone marrow-derived mesenchymal stromal cells (BMSCs; Cizkova et al., 2006a), Schwann cells (Pearse et al., 2007), and olfactory ensheathing cells (OECs; Ruitenberg et al., 2005) have been explored in the search for efficient SCI therapies.
BMSCs or umbilical cord blood cells (hematopoietic and mesenchymal stromal cells), which have been primarily used for the treatment of serious and life-threatening blood-related diseases, have more recently been used clinically in broader applications for the treatment of various bone, cartilage, cardiac, and neurological diseases (Orlic, 2003; Sykova et al., 2006). However, in many cases, their beneficial effect is most likely due to the release of pro-regenerative growth factors or cytokines (Zacharek et al., 2007), or by indirect immunomodulatory effects (Djouad et al., 2003), rather than by direct cell replacement (Jorgensen, 2009). Despite these findings, the transplantation of autologous or allogeneic mesenchymal stromal cells has been considered as a potential therapeutic approach to a wide variety of neurodegenerative diseases (Cizkova et al., 2006a; Hofstetter et al., 2002; Nandoe Tewarie et al., 2009; Sykova and Jendelova, 2005). However, one of the key challenges for successful transplantation is to use the least invasive approach that is locally-targeted and minimizes cell loss and surgical procedure-induced tissue damage.
Therefore, in the present study we used MSCs derived from rat bone marrow to standardize and optimize the intrathecal (IT) transplantation of stem cells after a moderate (12.5 μL) balloon-compression SCI in adult rats. Our results confirm that IT delivery represents a non-invasive transplantation strategy, which may improve post-injury locomotor function, and provides a promising strategy for additional testing of embryonic stem cells or spinal oligodendroglial progenitor transplantation therapies in preclinical models with small animals or primates.
Methods
Isolation and culture of rat mesenchymal stromal cells
MSCs were isolated from the bone marrow of three adult male Wistar rats (300 g), that had been collected from the long bones (femur and tibia), and were characterized as previously described (Cizkova et al., 2006b; Sykova and Jendelova, 2005). The isolated bone marrow was dissected into small pieces, gently homogenized, and filtered (70 μm) to remove bone fragments. Mononuclear cells (MNCs) were isolated by Ficoll density gradient centrifugation (1.077 g/mL; Sigma-Aldrich, Steinheim, Germany) at 400 g for 20 min. MNCs were collected from the interface, washed in Dulbecco's modified Eagle's medium (DMEM), and centrifuged at 600×g for 10 min. The cell pellet was re-suspended in 1 mL of DMEM, the pooled cells were counted, and their viability was assessed using the trypan blue dye exclusion method. MNCs were subsequently resuspended in culture medium composed of DMEM supplemented with 10% fetal calf serum (FCS; GIBCO Laboratories, Grand Island, NY), antibiotics (100 U/mL penicillin G and 100 μg/m streptomycin sulfate; Invitrogen, Carlsbad, CA), and plated at a density of 1×106 cells/25 cm2 in tissue culture flasks. The cells were incubated in a humidified atmosphere with 5% CO2 at 37°C. The medium was exchanged every 3–4 days thereafter. When the cultures reached 80% of confluence, the MSCs were passaged with 0.25% trypsin/0.53 mM EDTA (Invitrogen), and re-plated at a density of 5000 cells/cm2. Cells at passage 3–4 were used for the PKH-67 labeling procedure and thereafter for transplantation.
Labeling of mesenchymal stromal cells with the cell linker dye PKH67
MSCs were labeled with the green fluorescent cell linker PKH-67 according to the Sigma protocol (PKH67-GL) 24–48 h prior to transplantation. At passage 3–4, adherent MSCs were detached with 0.25% trypsin/0.53 mM EDTA to obtain a single cell suspension. After detachment, 1×107 cells were centrifuged (600×g for 10 min), washed, and then the final pellet was resuspended in 1 mL of Diluent C (an iso-osmotic mannitol loading medium), with freshly prepared PKH-67 (2–4 μL) membrane linker (4×10−6 molar PKH-67). The sample was then incubated at room temperature for 5 min followed by incubation at 4°C for 10 min. The staining reaction was stopped by adding an equal volume of α-MEM with 5% FCS. The labeled MSCs were collected by centrifugation at 400×g for 10 min, and diluted in 500 μL of sterile saline, which was used for IT transplantation (300 μL/15 rats). In addition, a sample (∼ 200 μL) of labeled PKH-67 MSCs (1×105 cells) was resuspended in DMEM supplemented with 10% FCS and antibiotics (100 U/mL penicillin G and 100 μg/mL streptomycin sulfate; Invitrogen), plated at a density of 5000 cells/cm2 in 6-well culture plates, and incubated in a humidified atmosphere with 5% CO2 at 37°C for two additional weeks in order to confirm the efficacy of PKH-67 labeling in fully differentiated MSCs under in vitro conditions.
Evaluation of PKH-67 labeling efficacy
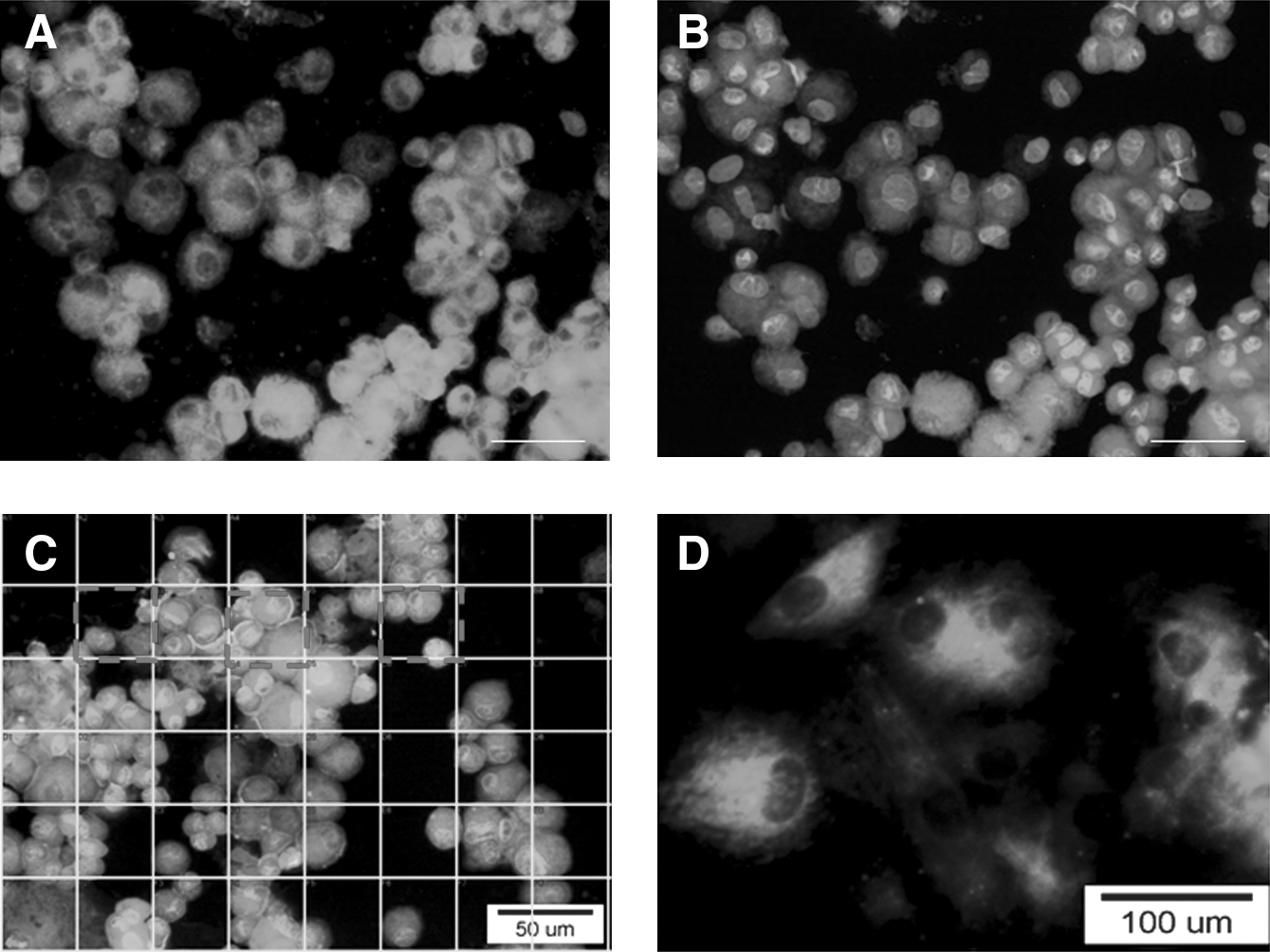
Prior to transplantation, the efficacy of PKH-67 MSC labeling was determined using the cytocentrifuge method (StatSpin Cytofuge; Iris Sample Processing, Inc., Westwood, MA), in which centrifugal force is to used to deposit a monolayer of cells onto microscope slides. Four samples of PKH-67-labeled MSCs (80–100 μL cell suspension) were centrifuged at 27×g for 6 min in disposable chambers. Samples of labeled MSCs were concentrated in a monolayer that covered approximately a 7-mm-diameter area on the slide with minimal cell loss to the filter. The cells were then fixed with 4% paraformaldehyde (PFA), washed two times with phosphate-buffered saline (PBS), and 200 μL of 4′,6-diamidino-2-phenylindole (DAPI) was incubated with the cells at room temperature for 20 min in a dark humidified chamber. Finally, the slides were washed two times in PBS and covered with mounting medium for analysis (Vectashield; Vector Laboratories, Burlingame, CA). The efficacy of the PKH-67 staining procedure was investigated by fluorescence microscopy (Nikon Eclipse Ti), with FITCI and DAPI filters. The number of labeled cells (merged PKH-67+DAPI) was analyzed in a standard counting grid (40 μm×40 μm frame), and a total of 100 squares/per slide were counted from 4 histological slides (Fig. 1A–C).
(
Spinal cord trauma
All experimental procedures were approved by the institutional ethical committee for animal research, and were in accordance with the Slovak Law for Animal protection (no. 115/1995). The SCI was induced using the modified balloon-compression technique in adult male Wistar rats (n=63, n=60 for the transplantation experiments; n=3 for the preliminary IT dose and volume distribution study), weighing between 300 and 320 g, according to our previous study (Vanicky et al., 2001). Manual bladder expression was required for 7–14 days after the injury until the bladder reflex was established. No antibiotic treatment was used.
Intrathecal implant procedure
IT catheter implantation was performed according to our previously published procedure (Hayes et al., 2003). The rats were anesthetized with 1.5–2% halothane, and following a loss of responsiveness, the head was fixed in a stereotaxic head holder and a face mask was fixed over the rat's muzzle to maintain anesthesia administration. The posterior scalp was incised (2–3 cm) at the midline and the muscles were gently separated by blunt dissection with forceps. At the junction of the occipital bone and atlas, the fascia overlying the cisterna magna was removed until the slightly transparent, white dura was visualized. The atlanto-occipital membrane was blotted dry to visualize the entire area, and a 3- to 4-mm incision was made through the dural midline using a 30-gauge needle with the tip bent at a 45° angle. The PE-5 end (3.4 cm long) of the IT catheter was inserted into the IT space and carefully pushed using a slight rotating movement to the required depth with gentle pulling of the tail at the same time. The opposite PE-10 catheter end was externalized on the forehead and the end was plugged with 4–5 mm of stainless steel 28-gauge wire. The overlying muscles and skin were sutured using a silk suture to fix the catheter in place. All implanted IT catheters were flushed with 10.0 μL of saline for 5 min to test their transition, and in the case of an obstruction, the catheter was repositioned or exchanged. After recovery, each rat was evaluated for additional limb dysfunction, spinal asymmetry, pain, or adverse surgical effects, and sacrificed immediately if any of these were observed.
Preliminary study: Evaluation of the intrathecal delivery distribution pattern within the spinal cord by DiI delivery
To evaluate the extent and the penetration pattern of the IT catheter delivery dose into the spinal cord tissue, three rats were injected by IT delivery 3 days after the SCI with a single 15-μL dose of DiI (4% in saline) flushed with 5 μL of sterile saline over 15 min (Vybrant® DiI cell-labeling solution; Invitrogen). After recovery, the rats were observed for possible locomotor impairments for an additional 4 h. Finally, all three rats were deeply anesthetized (IP injection of 50 mg/kg pentobarbital) and intracardially perfused with 0.1 M PBS (pH 7.4) for 3 min, followed by cold 2% PFA in PBS for 10 min. The spinal cord, brain, and externalized IT catheter were carefully dissected (Fig. 2A and B). The position of the IT catheter from its entrance (cisterna magna) throughout the entire spinal cord to the end of the tip (rostrally adjacent to the lesion site) was identified macroscopically (Fig. 2C and C′). The distribution of DiI was visualized by the presence of pink-stained spinal cord tissue. Samples taken 0.5–1.0 cm in each direction rostrally and caudally to the site of injury and from the central lesion were embedded in embedding medium. Serial transverse cryostat spinal cord sections (20 μm thick) were then cut and mounted directly onto slides. Sections were taken at 500- to 1000-μm intervals, and 5–10 sections were taken from each block. Representative slides were used for analysis of DiI distribution.
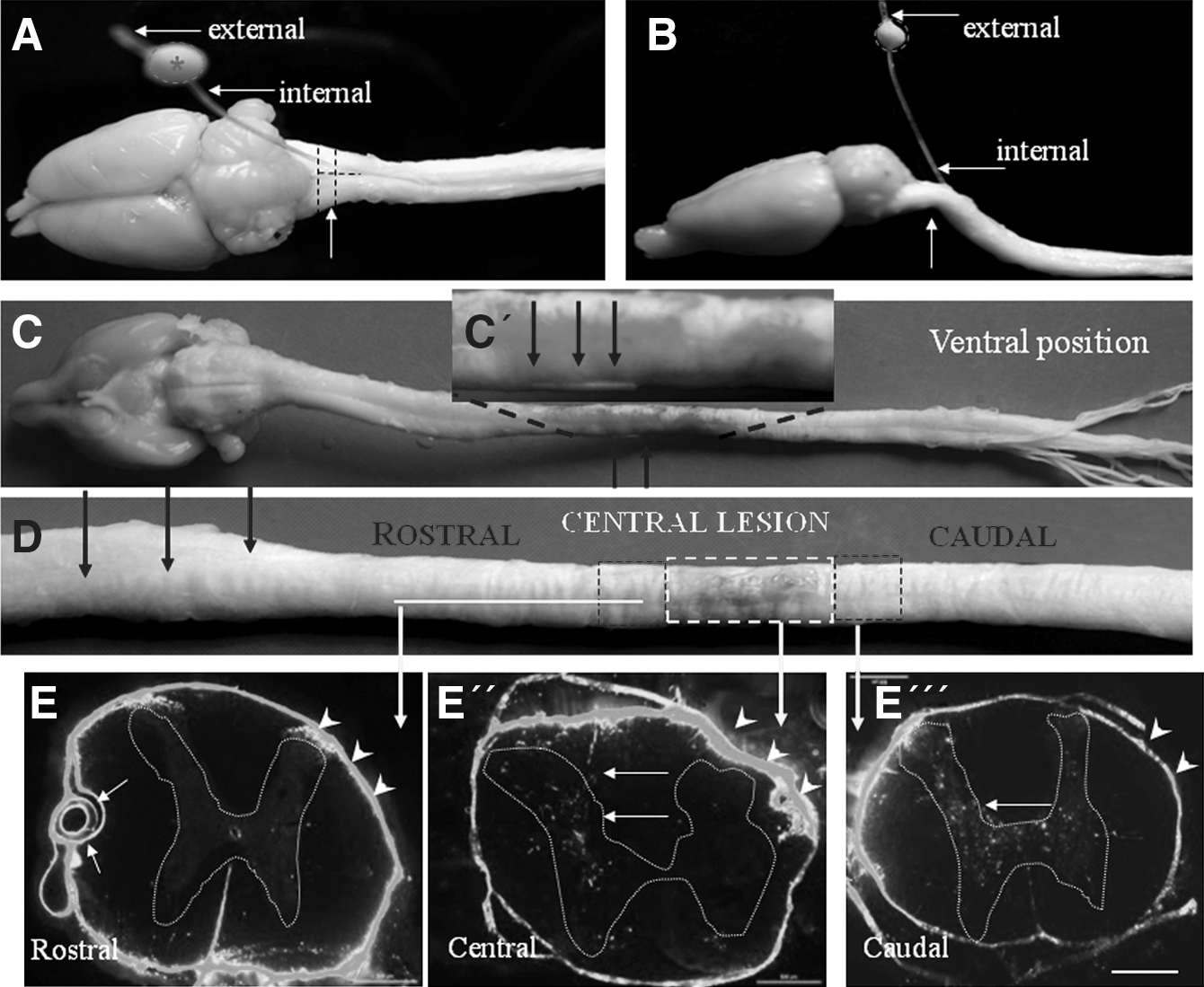
Macroscopic observation of the dissected brain and spinal cord with an implanted single-lumen catheter. The internalized PE-5 tubing with the lumen linked to the externalized PE-10 site is partially pulled out from the original insertion point (arrow); upper view (
Transplantation of mesenchymal stromal cells
All SCI rats were randomly divided into the following groups: (1) low-dose (LD) group receiving a single injection (5×105 MSCs/20 μL/rat/d) at 3 days; n=7; LD3D) or 7 days (n=8; LD7D) after SCI; (2) high-dose (HD) group receiving three daily injections of 5×105 MSCs/20 μL/rat/d for a total of 1.5×106 MSCs/rat for 3 days, either on days 3, 4, and 5 (n=7; HD3D), or on days 7, 8, and 9 (n=8; HD7D) after SCI; (3) a saline LD group (SLD) receiving 20 μL of saline per rat starting at 3 days (n=7; SLD3D) or 7 days (n=8; SLD7D); and (4) a saline HD group (SHD) receiving saline/20 μL/rat on days 3, 4, and 5 (n=7; SHD3D) or on days 7, 8, and 9 (n=8; SHD7D) after SCI. A maximum dose of 15 μL of MSCs resuspended in sterile saline was flushed with 5 μL of saline over 15 min through a calibrated PE10 catheter (calibrated by 5-μL increments up to 25 μL), which was connected to a 500-μL Hamilton syringe attached to a mechanical mini-pump. This procedure was performed in each rat of the LD3D, LD7D, HD3D, HD7D, SLD, and SHD groups. Implantation of the IT catheter was performed on the same day as transplantation, either 3 days or 7 days after SCI. All animals were intracardially perfused 28 days after SCI (21–25 days after transplantation).
Behavioral testing of motor function (BBB scoring)
Animals were evaluated before surgery and once a week after surgery for 4 weeks. Each rat was tested for 5 min by two blinded examiners. The motor performance was assessed using the Basso-Beattie-Bresnahan (BBB) 21-point open field locomotor scale (Basso et al., 1995). BBB scores, which categorize combinations of rat hindlimb movements, trunk position and stability, stepping, coordination, paw placement, toe clearance, and tail position, were analyzed. In this evaluation, 0 represents no locomotion and 21 represents normal motor function.
Quantification analysis
At the end of the study (28 days after SCI), all of the animals were deeply anesthetized with a ketamine-xylazine cocktail (15 mg/kg of xylazine and 150 mg/kg of ketamine), and transcardially perfused with 0.1 M PBS, followed by 2% paraformaldehyde in PBS. The spinal cord and externalized IT catheter were removed, post-fixed in the same fixative solution overnight at 4°C, and embedded in gelatin albumin substrate in 2% paraformaldehyde in PBS. Frozen spinal cord sections were cut from a 1.5-cm-long spinal cord segment positioned on the injury epicenter, embedded in embedding medium, dissected into three 0.5-cm-thick blocks (rostral, epicenter, and caudal), and stored at −20°C. Sections 10 μm thick were then serially cut from the epicenter and mounted directly onto slides. From the rostral and caudal regions, 40-μm-thick sections were cut and immersed in PBS (floating sections). Sections were taken at 200-μm intervals and 20 sections per block were obtained. Ten sections per block were stained with hematoxylin and eosin (H&E) to assess tissue morphology and determine the injury epicenter, and 10 sections per block were used for quantitative analysis of cellular PKH-67 distribution. The slides were analyzed using a Nikon light or fluorescence microscope (Nikon Eclipse), and captured with a Nikon digital camera DS Fi1 or DSQi1Mc. Quantitative analysis of transplanted PKH-67 MSCs was performed according to our previously published stereological technique (Cizkova et al., 2009; Marsala et al., 2004). PKH-67-positive fields were assessed from 10 sections per block under a 60× oil immersion objective (optical images were made using a motorized z stage, 1 μm), and the number of DAPI/PKH-67-positive (optical images were made using a motorized z stage, 1 μm), and the total numbers of DAPI/PKH-67-positive cells were calculated using stereological principles of systematic, random sampling, and the stereological fractionator sampling formula N=Q×1/hsf×1/asf×1/ssf, where N is the total number of positive nuclei, Q is the sum of the cells counted, hsf is the height sampling fraction, asf is the area sampling fraction, and ssf is the slice sampling fraction (Kakinohana et al., 2004). The slides were analyzed using a Nikon light or fluorescence microscope, and the images were captured with a digital camera. The images were prepared with Photoshop 7.0 and digitally stored for further processing.
Statistical analysis
Behavioral data determined from the BBB scores were averaged across the hindlimbs. Data from SLD animals at 3 days and at 7 days were pooled together for the SLD group, and the data from SHD animals at 3, 4, and 5 days, as well as 7, 8, and 9 days, were pooled for the SHD group. The differences between the experimental groups were analyzed using one-way analysis of variance (ANOVA) with a Tukey-Kramer multiple comparisons test. All data are presented as mean values±standard error of the mean (SEM). Differences between groups were considered statistically significant if p<0.05 or p<0.01.
Results
In vitro PKH-67 labeling
The viability of PKH-67-labeled MSCs was 91±3%, as assessed by the four independent calculations of the trypan blue exclusion test, which indicated the low cytotoxity of the PKH-67-fluorescent dye. However, we found that successful labeling of MSCs with PKH-67 required prolonging the labeling procedure from the recommended 5 min up to 15 min (5 min at room temperature followed by a 10-min incubation at 4°C). This modification enhanced the staining procedure and enabled more uniform labeling, which resulted in the majority of MSCs being completely stained (Fig. 1A–D). Using this protocol, we found that the efficacy of PKH-67 MSC labeling ranged between 87–95%. Although these modifications enhanced the staining of the cells, some variability between experiments still occurred. In addition, we also confirmed that PKH-67 labeling of MSCs was stable during differentiation (2–3 weeks) in vitro, where bright, PKH-67-positive, differentiated MSCs with processes were observed (Fig. 1D).
Intrathecal implantation/evaluation of DiI distribution
The dissemination of injected DiI was clearly visualized at the lesion site of the dissected spinal cord. The pink-stained tissue was mainly located over the ventral aspect of the spinal cord (total area of 1.5–2.0 cm; Fig. 2C and C′), while on the dorsal surface that contained hemorrhages, almost no colored tissue was observed macroscopically (Fig. 2D). The transverse cryostat spinal cord sections taken from the rostral, central, and caudal segments (Fig. 2D) confirmed the DiI distribution, which was observed as intense autofluorescence located within the subarachnoidal space of the spinal cord (pia mater and dura mater; Fig. 2E′, E″, and E′″). However, only scattered autofluorescence could be seen within damaged gray and white matter at the central lesion and caudal segments (Fig. 2E″ and E′″).
Improvement of motor locomotion
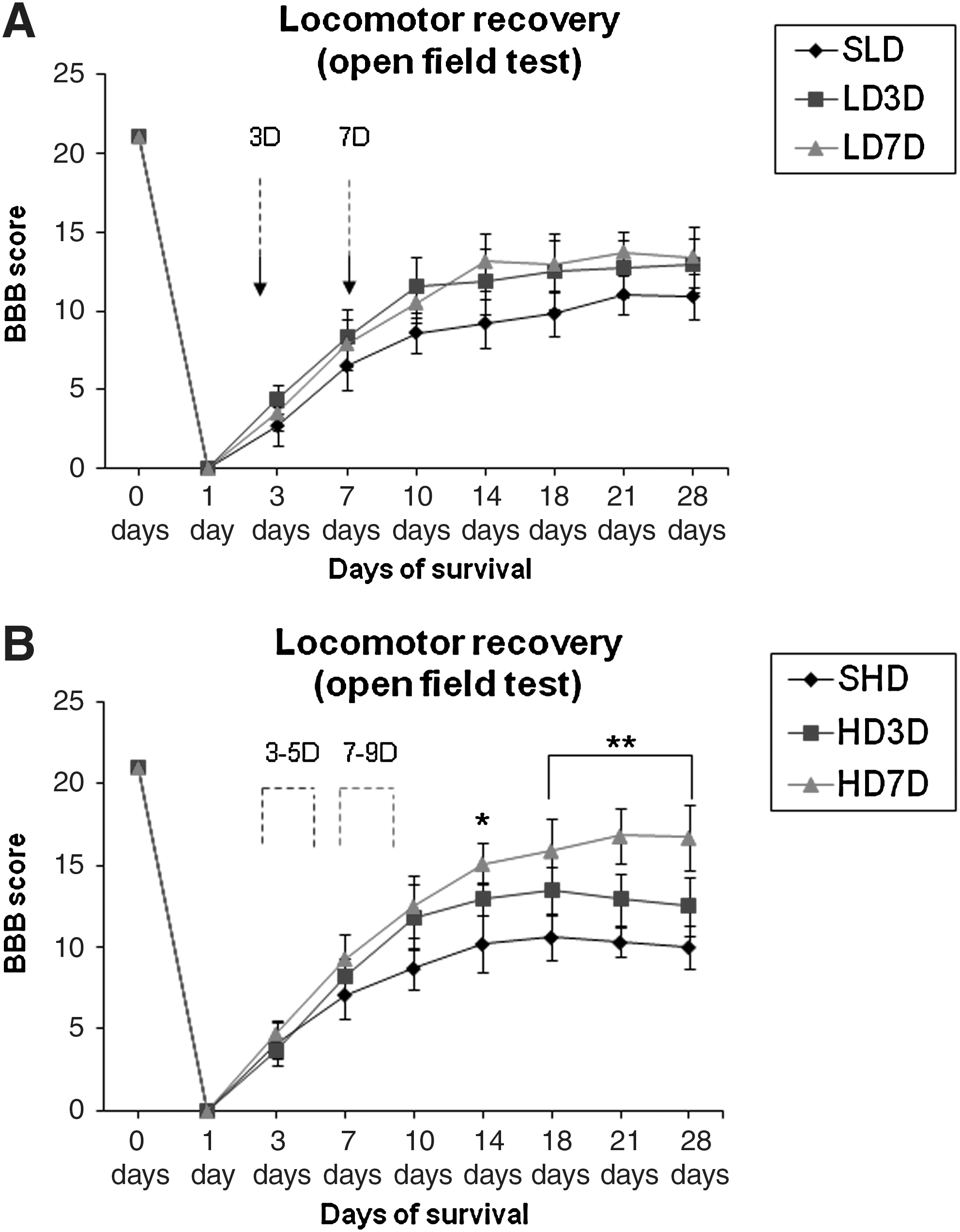
The LD group that received a single injection (5×105 MSCs/rat) at 3 days (LD3D) or 7 days (LD7D) after SCI did not show any significant functional recovery, and the BBB scores only slightly increased, reaching a maximum BBB score of 12.9±1.7 after 28 days when the cells were administered at 3 days, or 13.7±1.8 after 21 days when the cells were administered at 7 days, compared to the SLD group (BBB scores 11.0±1.2 at 21 days and 10.9±1.4 at 28 days; Fig. 3A).
(
A non-significant locomotor improvement was seen in the HD3D group receiving three daily injections (a total of 1.5×106 MSCs/rat) at 3, 4, and 5 days, which had a BBB score of 13.5±1.5 at 18 days. This score further decreased and closely correlated with the LD and saline groups (Fig. 3B). The only significant improvement in motor function was detected in the HD7D group, which received three daily injections (a total of 1.5×106 MSCs/rat) at 7, 8, and 9 days after SCI, and had final BBB scores of 15.1±1.3, 15.9±1.9, 16.8±1.7, and 16.7±2.0, at 14, 18, 21, and 28 days, respectively. The gradual recovery of hindlimb locomotion observed between the SHD and HD7D experimental groups was statistically significant at 14 days (p<0.05), and at 18, 21, and 28 days (p<0.01; Fig. 3B).
Mesenchymal stromal cell survival and distribution
The LD group
After a single IT delivery at 3 or 7 days, transplanted PKH-67 MSCs were found scattered and surviving within the subarachnoidal space (Fig. 4A–D). Grafted cells showed limited migration into the central lesion, although a few cells were found to be penetrating into the dorsal roots (Fig. 4A), as well as the ventral or lateral white matter (Fig. 4B and C). However, the majority of transplanted cells were mainly found attached to the ventral pia mater as individual or small clusters of cells surrounding the anterior spinal artery (Fig. 4B). Furthermore, a clear, thin stream of transplanted cells within the anterior median fissure was detected invading into the deeper ventral white matter (100–200 μm; Fig. 4B). A similar cluster of PKH-67-grafted cells was found at the lateral spinal cord regions, but with no or minimal migration (<100 μm) within the white matter (Fig. 4C).
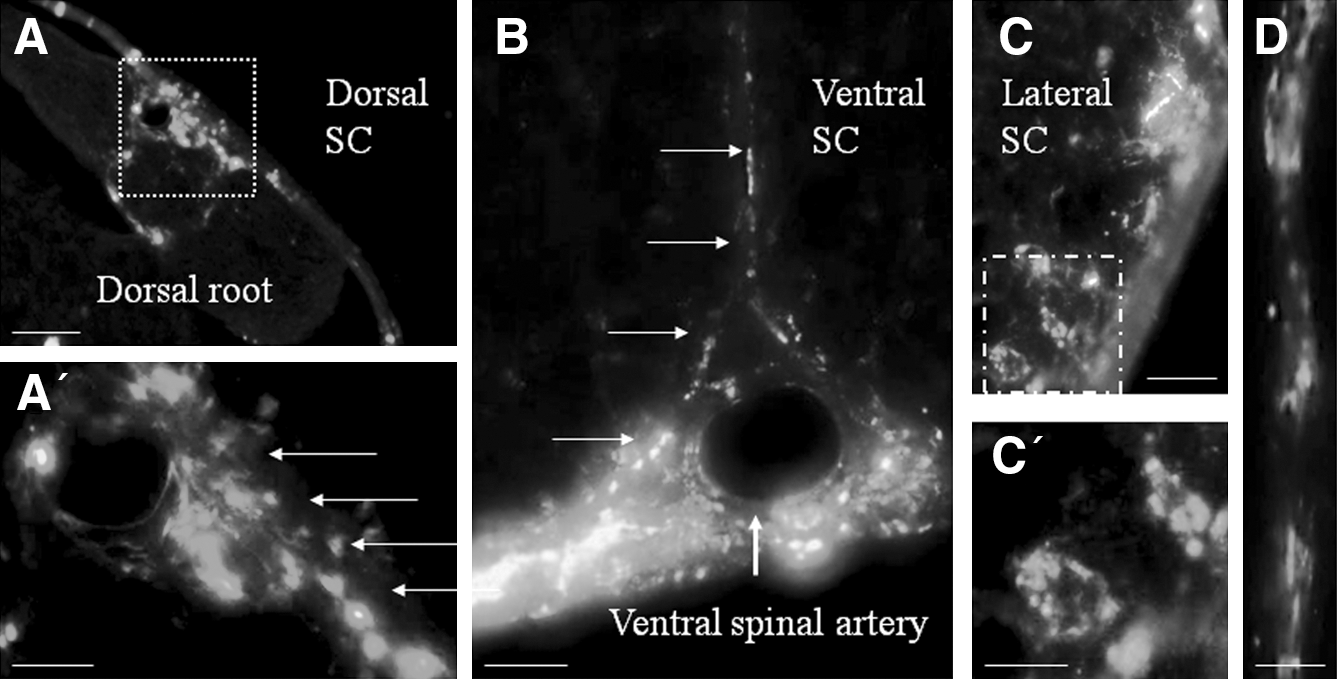
Distribution of PKH-67 mesenchymal stromal cells (MSCs) in the thoracic (T9) transverse spinal cord sections after a single intrathecal (IT) delivery in the low-dose (LD) 7-day group 28 days after spinal cord injury (SCI). MSCs were found within the subarachnoidal space (
The HD group
In contrast to the LD group, animals treated with three daily injections of MSCs at 7, 8, and 9 days showed engraftment of PKH-67 cells within the lesioned spinal cord tissue. Transplanted MSCs formed a migrating PKH-67 green fluorescence cell tract that continuously extended from the outer white matter regions towards the lesion cavity site (Fig. 5A). The PKH-67 grafts were organized into a network-like structure, composed of tight, adjacent, or scattered cells filling all or part of the lesion cavity (Fig. 5A and B). Serial sectioning of the spinal cord at a depth of 200 μm enabled us to distinguish almost complete grafts in 3 out of 8 transplanted rats (Fig. 5A), or scattered grafted cells within damaged tissue in 4 rats. One transplanted rat only had PKH-67 MSCs within the subdural space. Engrafted cells were found mainly in the white matter (rostral or central lesion site) as round, undifferentiated, or occasionally branch-like individual cells occasionally surrounded with fine fibers (Fig. 5B). Dissemination of PKH-67 cells was also clearly located within the subarachnoidal space, attached to the pia mater, or even located within the inner central canal area (Fig. 5C). In contrast, early transplantation at 3, 4, and 5 days led to a complete absence of PKH-67 MSCs in the damaged white matter. In addition, we were able to observe scattered PKH-67 MSCs around the anterior spinal artery, blood vessels, and axons, similar to that observed in the LD group (Fig. 5D and E). Moreover, the engraftment of injected PKH-67 MSCs within the lesioned spinal cord tissue mainly correlated with the position of the IT catheter (dorsal, lateral, or ventral) with both application strategies (Fig. 5F).
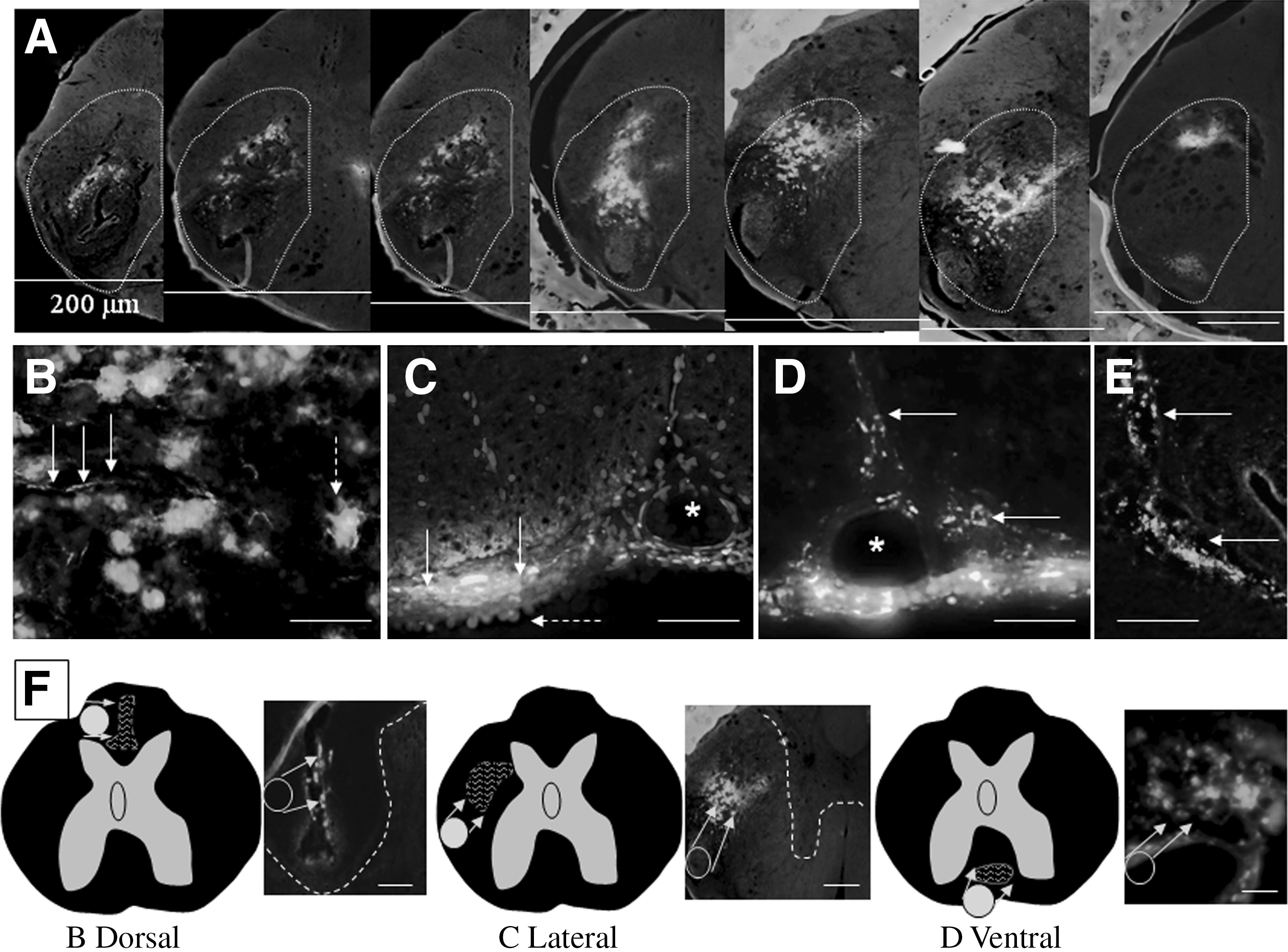
Engrafted PKH-67 mesenchymal stromal cells (MSCs) in the thoracic (T9) serially cut transverse spinal cord sections after intrathecal (IT) delivery in the high-dose (HD) 7- to 9-day group 28 days after spinal cord injury (SCI). (
Quantification of transplants
The majority of PKH-67-labeled cells were found within the damaged white matter with maximal spreading of cells 2–3 mm rostrally, but not caudally, from the lesion in the HD group transplanted at 7, 8, and 9 days post-injury. In four rats, we identified complete grafts spreading into the lateral/ventrolateral white matter. These rats had 116,258±8568, 81,024±3328, 111,878±10,631, and 92,064±2450 cells. The average cell number from these rats was 100,306±5092 cells per graft, which represented 6.85±0.41% of total transplanted PKH-67 MSCs (Fig. 6A and B; Table 1). In three rats, small clusters (partial grafts) of engrafted MSCs were found at the various sites of damaged white matter, and revealed even lower numbers of cells, with an average of 38,385±3556 cells per graft, representing 2.5±0.23% of the total transplanted PKH-67 MSCs (Fig. 6D). Therefore, an average of 4.67±0.32% of grafted cells was found in the HD group. In one rat, the PKH-67 MSCs cells remained attached to the pia mater, which was similar to what was seen in the LD group.

(
HD, high-dose; MSC, mesenchymal stem cell; compl, complete graft; part, partial graft containing scattered PKH67 cells; negat, negative, no cell engrafted into the white matter.
Discussion
In the present study, we have provided evidence that PKH-67-labeled MSCs can be delivered through an intrathecal catheter directly to the lesion site of rats that underwent a moderate SCI. We further showed that after three daily injections, MSCs migrated and integrated into the damaged spinal cord tissue when administered 7–9 days after SCI, but not at earlier applications (3–5 days), or after a single injection, which most likely contributed to the functional recovery. Since MSCs secrete a wide variety of trophic factors (Wilkins et al., 2009) that support host axonal growth and functional recovery and easily target sites of tissue injury (Stappenbeck and Miyoshi, 2009), they were ideal candidates for our IT delivery experiments. Visualization of MSC distribution within the recipient spinal cord tissue was made possible by using the PKH-67 membrane linker, which provided highly effective, homogenous cellular labeling with low cytotoxicity. The highly-stable PKH-67 autofluorescence enabled us to track the distribution of transplanted MSCs within the intrathecal space and the spinal cord tissue directly on the cryostat sections.
The key focus of our experiments was to standardize and optimize an IT application for the purpose of delivering PKH-67-labeled MSCs locally and as close as possible to the site of SCI. To achieve this goal, we chose the single-lumen catheter model that was developed primarily for experimental studies of spinal opiate tolerance and spinal drug delivery (Yaksh, 1999). With this IT technique, we were able to deliver repetitive doses of PKH-67 MSCs directly to the central lesion without the need for additional surgery or other stressful manipulations. The length of the intrathecal catheter (3.4 cm) matched the position of the primary lesion at the T9 segment, and therefore the tip of the catheter was located in close proximity to the injury.
Before our main experimental study, we had to verify the position of the catheter and expected volume of the dose distribution in three separate rats with SCI by using IT injection of the fluorescent dye DiI. A volume of 20 μL of DiI was selected based on a previous study, which was less than 10% of the total cerebrospinal fluid (CSF) volume (250 μL) in the rat (Hua et al., 1999; Yaksh, 1999). The injected DiI tended to gather primarily in the ventral portion of the central lesion site, which may be related to the physiological body position of the rat and gravity. Furthermore, the fluorescent dye accumulated along the central lesion within the range of 1–2 mm rostro-caudally, and entered the central white/gray matter at a very low density. One explanation for its low penetration into the lesioned tissue may be due to the lack of chemotactic signaling, which is most likely involved in the migration processes of stem cell transplantation, but is not applicable to dye penetration (Greco and Rameshwar, 2008). Alternatively, a more reasonable explanation is that the low DiI incorporation may be due to the short survival period of the rats after dye application (4 h).
Once we verified the technical parameters related to IT delivery, we focused our attention on defining two key parameters for the present experiment: (1) the optimal dose of transplanted PKH-67 MSCs, and (2) the ideal timing for cellular infusion. To determine the optimal dose of injected MSCs, we compared the effect of a single dose (LD) with that of three daily repetitive doses (HD). Our reasoning for the repetitive doses was not only to increase the number of delivered PKH-67 MSCs, but to also provide the CSF with fresh stem cells during three daily applications. As we expected, significant differences in the engraftment of PKH-67 MSCs between the two experimental groups were observed.
In the single-dose LD group, which received 5×105 of PKH-67 MSCs at 3 or 7 days post-injury, we observed a homogenous distribution of PKH-67-labeled MSCs that mainly attached to the pia mater surrounding the central lesion. It is well known that normal CSF produces trophic factors that are beneficial for stem cell survival and differentiation, whereas during pathological conditions, the altered substrate content causes apoptosis or other adverse effects (Oren et al., 2001). Since the majority of delivered cells were located within the subarachnoidal space, we hypothesize that the CSF of the injured spinal cord had no significant effect on MSC survival in these experiments. This has also been confirmed by a previous study, which showed high viability and proliferation of IT-delivered neural progenitors in a traumatic SCI model (Bai et al., 2003). However, in this group we did not observe the expected engraftment of transplants. The occasional invasion by injected PKH-67 MSCs into the ventral white matter occurred primarily along the anterior spinal artery. The fact that some MSCs were concentrated around major blood vessels in the ventral white matter may be due to the rich nutrient supply (Butler et al., 2010). Since many dose-response studies have shown rapid and major cell loss shortly after transplantation, we hypothesize that the LD (5×105 of PKH-67 MSCs) applied in the present experiment was too low, and therefore limited the number of grafted cells that survived at sites of suitable substrates, attached to the pia mater, or accumulated around blood vessels (Paul et al., 2009). Furthermore, LD transplantation had no beneficial effect on motor function improvement at both treatment times, which is in agreement with the low cell distribution seen in the subarachnoidal space and the lack of engraftment into the lesioned tissue.
A very similar distribution pattern of grafted MSCs within the recipient tissue was observed in the HD group injected with 3 daily doses (at days 3, 4, and 5, for a total of 1.5×106 of PKH-67 MSCs) with early grafting 3 days after SCI. Although higher numbers of surviving cells were attached to the pia mater or distributed around blood vessels, the animals showed only partial, non-significant improvements of motor function at the end of the study period. This may be caused by improper early IT delivery due to the strong inflammatory response that persisted within the damaged spinal cord parenchyma, which will be further discussed in more detail.
The most promising findings of this study were obtained in the HD group that received later delivery of MSCs, starting at 7 days post-injury (days 7, 8, and 9, for a total of 1.5×106 PKH-MSCs). In this group, the incorporation of transplanted cells and the formation of grafts within the white matter of the injured spinal cord parenchyma was observed. On the serial cryostat sections, we were only able to identify three complete grafts that could be seen from the beginning of the implantation site to the end. We noted a high variability in the numbers of surviving cells within the observed grafts, which ranged from approximately 24×103−116×103 cells, with an average of 73×103 cells per graft. The reason for this engraftment difference is not clear, but may be due to the incorrect position or transition of the catheter during cellular infusion.
If the tip of the catheter is adjacent to non-lesioned pia mater and white matter, penetration of cells is rather difficult, unlike when the catheter is in close proximity to the damaged tissue. Another complication may be related to catheter obstruction with clusters of transplanted cells, macrophages, or other substances that impede infusion (Allen et al., 2006; Miele et al., 2006). However, these limitations could easily be overcome in human trials by using radioimaging or ultrasound techniques, which are critical for guiding the IT catheter insertion, and allow confirming the correct positioning, or repositioning the catheter directly adjacent to the central lesion (Hassenbusch et al., 2002; Hebl, 2008; Karmakar et al., 2009). Correct placement of the IT catheter is an essential prerequisite for long-term use of the catheter and accurate engraftment of stem cells near damaged spinal cord parenchyma. This point was also confirmed in the present study, since the IT catheters were located laterally and in close proximity to the grafts in all of the successful engraftments. Furthermore, only the HD group at the late transplantation time point (7–9 days) showed significant improvement in motor function, which began at 14 days post-infusion and continued until sacrifice at day 28. Notably, in the case of the HD cellular infusion, we gradually injected 3 times more cells than in the LD transplant group. However, the goal of this application strategy was not only to deliver an increased number of cells, but to feed the IT system with freshly prepared MSCs daily for 3 days. We believe that this approach provides a new method for gradually replenishing stem cells within the damaged areas of nervous system tissue, which allows for better survival and incorporation of the transplant, and stimulates endogenous regenerative processes. The majority of the engrafted PKH-67 MSCs that survived had a round, undifferentiated morphology and occasional branch-like individual cells. We did not identify the specific expression of neuronal or glial markers, with the exception of nestin, which was only rarely found in PKH-67 MSCs (data not shown). Therefore, this study did not provide convincing evidence of a possible neural lineage for these cells.
Moreover, in both experimental groups, we sought to determine the ideal timing for transplantation. Our present findings are in agreement with the results from other previous studies, which confirmed that early transplantation, either by single or multiple injections 3–5 days after SCI, leads to very low cell survival, most likely due to an ongoing inflammatory response (Karimi-Abdolrezaee et al., 2006). It seems likely that after 1 week, a partial attenuation of the inflammatory process occurs, which allows for better survival of transplanted cells. In this study, we found that the optimal time for transplantation ranged between 7 and 9 days. In conclusion, we have confirmed the feasibility of delivering MSCs by IT catheter into the contused spinal cord. Multiple deliveries of MSCs through the CSF may be improved by utilizing a more sophisticated double-lumen catheter instead of a single-lumen catheter, which has a number of specific advantages for long-term transplantation studies, and allows for the injection of stem cells concurrently with trophic factors, biomaterials, or other substrates. Furthermore, we suggest that a higher dose, more than 1.5×106 injected cells, which is two to three times higher than that used in the present study, may lead to higher efficacy of cell survival, more engraftment into the host tissue, and improvement of functional recovery.
Footnotes
Acknowledgments
The authors wish to thank Dr. Stephen Minger from King's College for valuable comments and suggestions, and Marika Spontakova for technical assistance. This study was supported by grants VEGA 2-0114/11, VEGA 1-0674-09, MVTS-COST BM-1002, and APVV 51-002105.
Author Disclosure Statement
No competing financial interests exist.