
Abstract
Falls occur frequently in older adults. With ageing populations worldwide, an increase in fall-related traumatic head injuries can be expected. The aim of our study was to determine trends in traumatic head-injury–related hospitalizations among older adults. Therefore, a secular trend analysis of fall-related traumatic head injuries in the older Dutch population between 1986 and 2008 was performed, using the National Hospital Discharge Registry. All significant fall-related traumatic head injury hospitalizations in persons aged ≥65 years were extracted from this database. During the study period, traumatic head-injury–related hospitalizations increased by 213% to 3,010 in 2008. The incidence rate increased annually by 1.2% (95% CI: 0.6; 1.9) between 1986 and 2000. Since 2001, the increase has accelerated up to 11.6% (95% CI: 9.5; 13.8) per year. Overall, the age-adjusted incidence rate increased from 53.1 in 1986 to 119.1 per 100,000 older persons in 2008. Age-specific incidence rates increased in all age groups, especially in persons aged ≥85 years. Despite an overall reduction in the length of hospital stay per admission, the total number of hospital-bed-days increased with 31.5% to 20,250 between 1991 and 2008. In conclusion, numbers and incidence rates of significant traumatic head-injury–related hospitalization after a fall are increasing rapidly in the older Dutch population, especially in the oldest old, resulting in an increased health care demand. The recent increase might be explained by the ageing population, but also other factors may have contributed to the increase, such as an increased awareness of traumatic head injuries, the implementation of renewed guidelines for traumatic head injuries, and improved radiographic tools.
Introduction
A recent study in the older Finnish population aged ≥80 years showed an increase of 200% in the incidence rate of severe traumatic head injuries in females between 1970 and 2004 (Kannus et al., 2007). Also an increase in the number and age-specific incidence rates of injurious falls and concomitant health care consumption was shown for the older Dutch population (Hartholt et al., 2010b). The increased awareness of the likelihood of structural brain damage and traumatic head injuries over the last decades has resulted in new national and international guidelines for the diagnosis and management of traumatic head injuries (Maas et al., 1997; Vos et al., 2002). In 2001 a renewed national guideline with a diagnostic and therapeutic algorithm for traumatic head injuries has been implemented in the Netherlands (Commission for Healthcare Improvement of the Dutch Neurology Society, 2001), e.g., when to order a CT scan (Haydel et al., 2000) or hospitalize a patient. Furthermore, the quality and availability of diagnostic tools such as the CT scanner, has improved rapidly.
For health care services and health care economics it is essential to gain insight into the epidemiology, trends, and forecast for the future. The aim of this study was to quantify secular trends of fall-related hospitalizations resulting from traumatic head injuries in older adults in the Netherlands.
Methods
For this study, all significant traumatic head-injury–related hospitalizations caused by a fall between 1986 and 2008 were collected. Throughout the study period a significant traumatic head injury was defined using the International Classification of Diseases, 9th revision (ICD9) codes for traumatic head injuries: more specific code (skull fracture) 800-804.X, (contusion and concussion) 850-851.X, (bleeding) 852-853.X, and (other) 854.X (Table 1). A fall was defined by the ICD9 codes for external cause of injuries code E880-E889 and E929.9. Older persons were defined as persons aged ≥65 years. Data were retrieved from the National Medical Registration (LMR). The LMR collects hospital data in the Netherlands with a uniform classification system with a high national coverage (missing values <5%, except in 2007, when they were 12%) (van der Stegen, 2009). These figures were extrapolated by the Consumer and Safety Institute to full national coverage for each year. An extrapolation factor was estimated by comparing the adherence population of the participating hospitals with the total Dutch population in each year (van der Stegen, 2009). Data regarding hospital admissions, admission diagnosis, length of hospital stay (days), gender, age, and causes for external injuries are stored in this database. For each individual patient only one injury code, the primary diagnosis, was used. The primary diagnosis is based upon the medical records completed by the physicians treating the patient, and has been used as main diagnosis at discharge (in general the most severe injury).
Numbers of significant traumatic head-injury–related hospital admissions and admission duration were specified for age and gender in 1986, 1991, 1996, 2001, 2006, and 2008. The age-specific incidences were calculated in 5-year age groups using the number of fall-related hospital admissions resulting from a traumatic head injury in that specific age group, divided by the midyear population size within that specific age group for male and female patients, and was expressed per 100,000 persons in that age group. Age adjustment was done by “Direct Standardization”. Overall growth in the number of hospital admissions was calculated for 2008 in percents relative to the year 1986. The midyear population was used in each year of the study (Statistics Netherlands, 2009).
In order to model the trend in hospital admissions, a linear regression model with Poisson error and log link was built with log (midyear population size of each year of the study) as offset factor. A linear spline model (McNeil et al., 1977), with age, year, gender, and population size, was built to assess whether the annual growth changed over the study period for both genders. The parameter for calendar year, corrected for gender and age group, was transformed into percentage annual change (PAC). The spline function accommodated two piecewise linear fits, connected with one another at the knot. The best knot was estimated using the Joinpoint Regression Program, Version 3.4.3. April 2010. (Statistical Research and Applications Branch, National Cancer Institute; Information Management Services, Inc., Silver Spring, MD), and found to be January 1, 2001. The analysis including splines yielded estimates of annual changes in admission rates within each period (1986–2000 and 2001–2008). Comparison of these two periods enabled us to detect and quantify changes in the secular trend in admission rates, such as a stagnation or and increase of admission rates. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) software (version 16.1.1). A p-value<0.05 was considered statistically significant.
Results
During the study period from 1986 through 2008, a total number of 32,133 patients in the Netherlands aged ≥65 years, who had a significant traumatic head injury, required hospitalization after a fall. The annual number of older persons admitted with a significant traumatic head injury increased from 932 in 1986 to 3,010 (223% increase) in 2008 (Fig. 1). In the same period, the population of adults aged ≥65 years increased from 1.8 million in 1986 to 2.4 million (33% increase) in 2008 in the Netherlands.
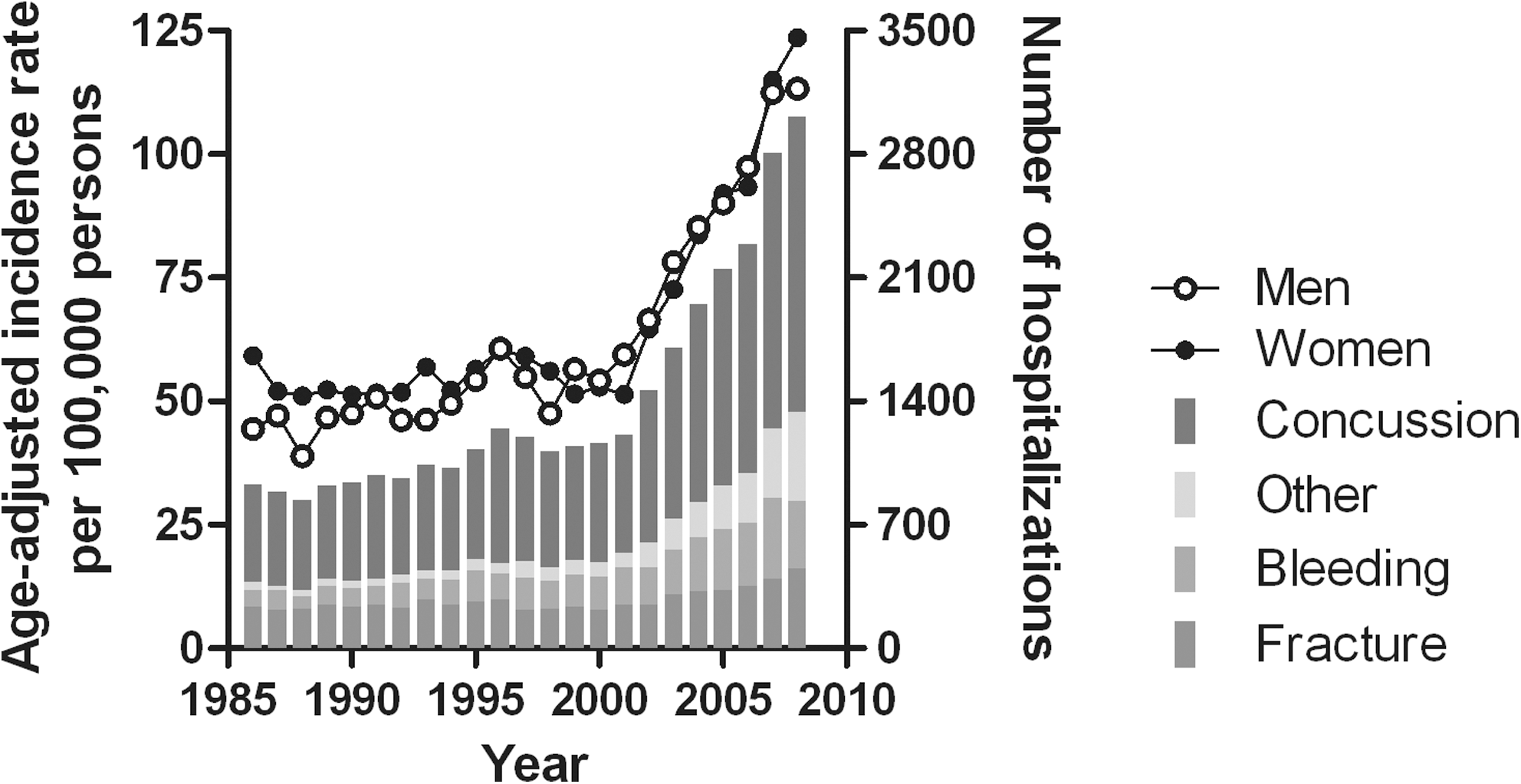
Numbers and type of traumatic head injury and age-adjusted incidence for fall-related traumatic head injuries, requiring hospitalization in persons ≥65 years in the Netherlands, 1986–2008.
The overall age-adjusted incidence rate of hospitalization of head trauma patients increased from 53.1 per 100,000 persons in 1986 to 119.3 per 100,000 persons in 2008. In men, the age-adjusted incidence rate increased from 44.4 per 100,000 persons in 1986 to 113.3 per 100,000 persons in 2008. In women it increased from 59.2 to 123.6 (Fig. 1).
Using a joint point analysis, the study period could be divided into two periods (1986–2000 and 2001–2008). The incidence rate increased annually by 1.2% (95% CI: 0.6; 1.9) between 1986 and 2000. From 2001 onwards, the increase accelerated up to 11.6% (95% CI: 9.5; 13.8) per year. The PAC of hospitalizations resulting from significant fall-related traumatic head injuries was different for men and women throughout the study period. Between 1986 and 2000 inclusively, the PAC for men was 1.8% (95% CI: 0.8; 2.9) and it increased to 9.9% (95% CI: 7.4; 12.4) from 2001 onwards. For women a comparable pattern was observed. The PAC increased from 0.6% (95% CI:−0.1; 1.3) between 1986 and 2000 to 12.3% (95% CI: 10.1; 14.5) from 2001 onwards.
The age-specific hospitalization rates increased throughout the study period for both genders and in all age groups (Table 2). The age-specific incidences increased with age and were highest among persons aged ≥85 years. The largest increase in incidence rate was seen in persons aged ≥90 years, in both men (180% increase to 357.1 per 100,000 persons) and women (301% increase to 352.9 per 100,000 persons) (Table 2).
Change is 2008 compared with 1986.
The majority of hospitalizations resulting from a traumatic head injury were because of a concussion or contusion (57.3%). Fractures, bleeding, and other/unspecified injuries were seen less frequently (Table 3). Increases in incidence rates were mostly attributed to an increase in concussions/contusions and bleedings. The number of patients admitted because of a fall-related concussion/contusion increased from 552 admissions in 1986 to 1,666 admissions in 2008. Fall-related bleedings in the head increased from 96 in 1986 to 382 in 2008 (Table 3).
The mean admission duration in older adults decreased over the last 17 years for all age-specific groups, from 16.5 days in 1991 to 6.7 days in 2008 (Fig. 2). Length of hospital stay for fall-related traumatic head injuries increased with age and peaked in patients 85–89 years of age.
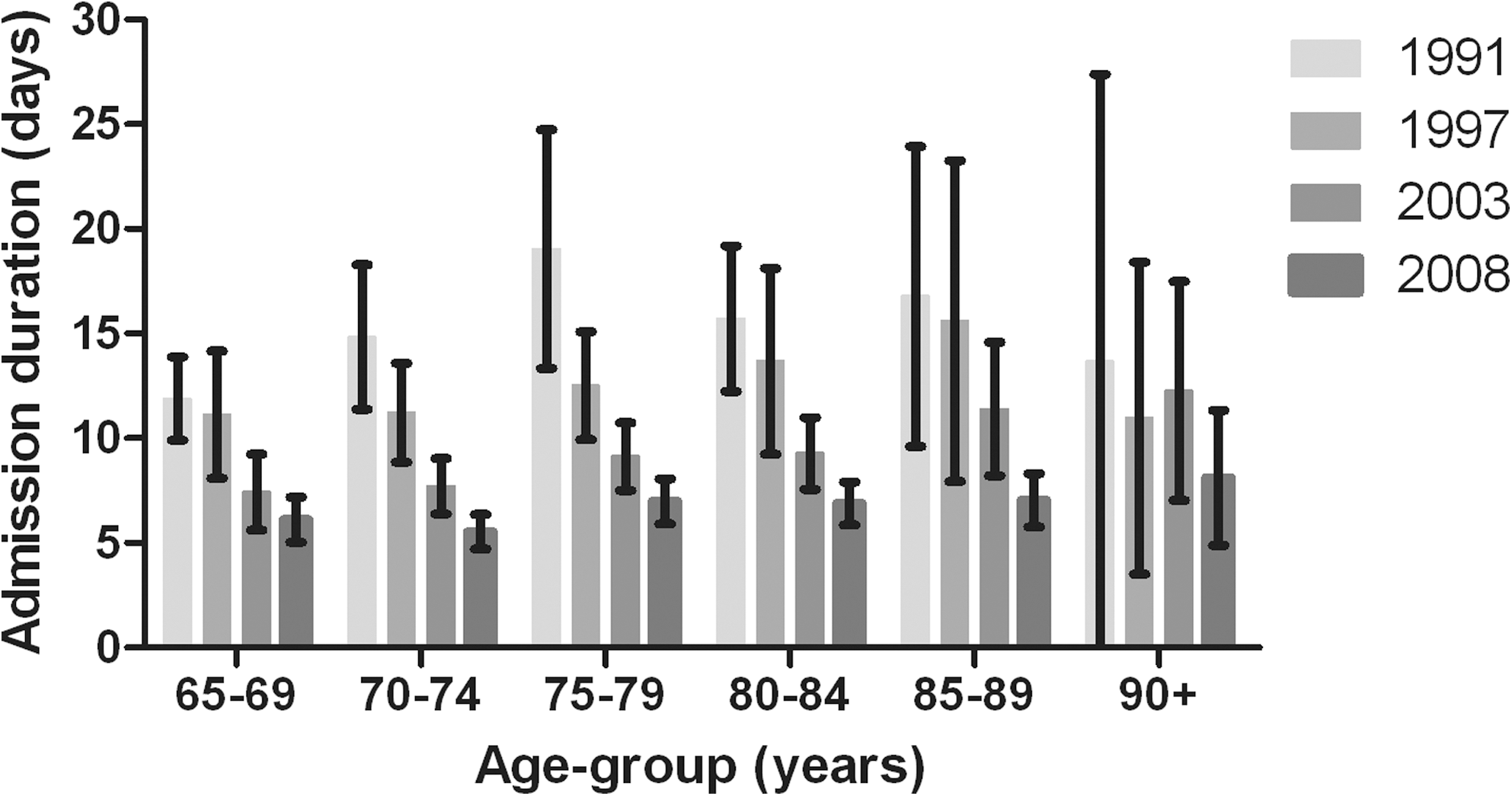
Mean admission duration for fall-related traumatic head injuries per age group in persons ≥65 years in the Netherlands, 1991–2008. Error bars indicate the 95% confidence interval.
Despite a decreased admission duration per admission, the total number of hospital-bed-days increased by a third, from 15,402 days in 1991 to 20,250 days in 2008, because of a rising number of admissions. For both men and women, the overall number of hospital-bed-days increased gradually. In older men it increased from 5,346 days in 1991 to 7,822 days in 2008 (46% increase). In all women aged ≥65 years the number of hospital-bed-days increased from 10,056 in 1991 to 12,428 in 2008 (24% increase; Fig. 3).

Total number of hospital-bed-days resulting from fall-related traumatic head injuries in persons ≥65 years in the Netherlands, 1991–2008.
Discussion
In this study, the number of significant fall-related traumatic head injuries in all persons aged ≥65 years in the Netherlands was quantified, in order to gain insight into time trends in admissions related to these injuries in older adults from 1986 throughout 2008. The incidence rates and numbers of hospitalizations increased in both men and women throughout the study period, especially among the oldest old.
In the first period (1986–2000) of this study, the overall age-adjusted incidence changed only marginally. This is comparable to data from the United States, where the incidence of traumatic head-injury-related hospitalizations in persons ≥65 years hardly changed between 1980 and 1981 and between 1994 and 1995 (Thurman and Guerrero, 1999). However, Kannus et al. reported an increasing incidence rate between 1970 and 2004 in fall-related traumatic head injuries among Finnish men and women >80 years of age (Kannus et al., 2007). In the current study, a similar increasing trend from 1986 was noted for the oldest old. The increase between 1986 and 2000 might have several causes. It could, at least partly, be explained by “the aging society” in the Netherlands (Statistics Netherlands, 2009). As life expectancy is increasing, older persons live longer, but with multiple medical problems. This may lead to increased risk of falls and fall-related injuries, such as traumatic head injuries (Bruggink et al., 2010). Although the age-adjusted incidence rates for men and women were similar, the absolute number of hospitalizations in women was higher than for men because of a female preponderance in the older Dutch population (Statistics Netherlands, 2009). Second, population-based health analyses in the Netherlands have shown that older adults are reporting fewer problems with their mobility (Hoeymans et al., 2009), which may partly be explained by improved medical care and the widespread introduction and use of walking and transportation mobility aids. As a result of improved mobility, patients may be at higher risk for falls. A similar trend of improved mobility in older adults has been reported for the United States (Freedman et al., 2002). The observed increased incidence rate of significant traumatic head injuries might also be the result of a more active lifestyle, such as walking, cycling and sport (Stamatakis and Chaudhury, 2008).
Hospitalization rates resulting from falls among the older population in general increased by 137% over the last decades (Hartholt et al., 2010b). Hospitalization rates resulting from fall-related traumatic head injuries increased more rapidly. A clear explanation for this finding is not known yet. Possible factors that may have contributed might be that traumatic head injuries have been a topic of research and preventive medicine over the last decades. This could have led to an increased awareness of the likelihood of structural brain damage in the elderly among health care professionals, and, consequently, to increased use of CT scanning and recognition of injuries. Moreover, the availability and quality of CT scanners has improved over the last decades, which also might have led to increased detection of minimal clinical symptomatology.
In 2001, a guideline for traumatic head injuries was introduced in the Netherlands (Commission for Healthcare Improvement of the Dutch Neurology Society, 2001). This guideline instructs, for example, that patients with specific risk factors such as anticoagulant drug intake should be screened radiographically. In 2000 and 2002, similar guidelines were introduced in the Scandinavian countries (Ingebrigtsen et al., 2000) and the United States (Faul et al., 2010; Jagoda et al., 2002), respectively. A recent report of the Centers for Disease Control and Prevention of the United States on traumatic brain injuries was published. During the period from 2002 to 2006 the incidence rate of hospitalizations increased from 67.6 in 2002 to 90.7 in 2006 per 100,000 older adults in the United States (Faul et al., 2010). This increase is similar to our results (increase from 65.4 in 2002 to 95.0 in 2006 per 100,000 older adults). Although no data are available to confirm a causal relation, the increased awareness in scientific literature and the implementation of the guideline, and consequently an increased use of radiographic imaging could have contributed, at least partly, to the increased detection of traumatic head injuries that require observation and hospitalization.
The recent development of admissions in significant fall-related traumatic head injuries has broad consequences for the required number of hospital beds and the related health care expenses. Although the length of hospital stay decreased between 1991 and 2008, it was not enough to compensate for the increased number of admissions. The decrease in length of hospital stay is in line with the general trend of reduced admission duration for injuries in our previous study (Hartholt et al., 2010b). The length of hospital stay was age-related and increased with age. However, the oldest old (persons aged ≥90 years) had a shorter admission duration, which might be explained by a higher number in this age group who are already living in a nursing home and consequently can be discharged from the hospital more rapidly.
A strength of this study is the availability of a highly accurate, electronic national population-based in-hospital database for an extensive period of 22 years (1986–2008) with the same coding system. But this study has also some limitations. In the Netherlands there is full national health care insurance, therefore the study results may not be directly translated to other countries. Further studies should confirm similar trends in other countries. Also some “double registration” could have occurred, as readmissions were not excluded. However, it is unlikely that readmissions influenced our results, because readmissions because of a trauma constitute in general only 2.6% of admissions in the Netherlands (Polinder et al., 2005). Another limitation of this link administrative database is that it does not contain data regarding underlying diagnoses, co-morbidities, treatments, injury severity, lifestyle, or medication use of the patients. This hampers the interpretation of causal mechanisms behind the observed trends.
In conclusion traumatic head injuries are frequently observed after a fall, and the number of these is increasing rapidly. As falls are the leading cause of traumatic head injuries and other types of injury in older adults (Jager et al., 2000), preventative strategies should focus on the prevention of falls. Known effective strategies (Gillespie et al., 2009; Kannus et al., 2005; Logan et al., 2010) should be further implemented to slow down the rising incidence of traumatic head injuries and their related therapies and morbidities, and to optimize the quality of life and functional outcome in elderly patients.
Footnotes
Acknowledgments
Klaas Hartholt is a research fellow at the Erasmus MC, appointed on a research grant from “The Netherlands Organization for Health Research and Development” (ZonMw), project number 170.885.607.
Author Disclosure Statement
No competing financial interests exist.